Diaphragmatic hernia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me synthesize a complete response.
Diaphragmatic Hernia
Definition
Congenital diaphragmatic hernia (CDH) is a spectrum of developmental conditions characterized by a diaphragmatic defect that allows abdominal contents to protrude into the thoracic cavity, disrupting lung and pulmonary vascular development. — Sabiston Textbook of Surgery, p. 2675
Anatomy & Types
The diaphragm is embryologically derived from the septum transversum, pleuroperitoneal folds, abdominal wall components, and the dorsal mesentery. These structures begin fusing at 3–4 weeks of gestation, completely separating the pleural and peritoneal cavities by 9 weeks. Incomplete fusion produces distinct hernia types:
| Type | Location | Frequency |
|---|---|---|
| Bochdalek | Posterior-lateral | 70–75% |
| Morgagni | Anterior (retrosternal) | 23–28% |
| Central | Central tendon | 2–7% |
- Bochdalek hernias: Left-sided in ~85% of cases, right-sided in ~13%, bilateral in ~2%
- Morgagni hernias are often asymptomatic until childhood or later
Incidence & Etiology
- Incidence: ~1 in 2,000–5,000 live births
- Most cases are sporadic, isolated, and non-syndromic
- Exact etiology unknown; animal models implicate genetic, environmental, and nutritional factors
- Associated anomalies (especially cardiac defects) seen in 25–50% of cases
Pathophysiology
Abdominal contents (stomach, bowel, and occasionally liver) herniate through the diaphragmatic defect and compress the ipsilateral developing lung, resulting in:
- Pulmonary hypoplasia — smaller bronchi, reduced branching, decreased alveolar surface area; both lungs affected, ipsilateral more severely
- Pulmonary hypertension — increased arteriolar smooth muscle thickness; vasculature is highly reactive to vasoactive factors
- Mediastinal shift — compresses contralateral lung as well
The severity of pulmonary hypoplasia and pulmonary hypertension are the primary determinants of morbidity and mortality. — Sabiston Textbook of Surgery, p. 2675
Prenatal Diagnosis & Prognosis
Routine ultrasound can detect CDH as early as 15 weeks of gestation. Findings at 22–24 weeks include:
- Mediastinal shift
- Juxta-cardiac gastric dilatation
- Polyhydramnios
- Liver herniation into chest (right-sided CDH)
Prognostic tools:
- Lung-to-Head Ratio (LHR): Ratio of contralateral lung area to head circumference
- LHR < 1.0 → poor prognosis
- LHR > 1.4 → ~100% survival
- Observed/Expected LHR (O/E LHR): Normalized to gestational age
- O/E LHR < 25% → < 20% survival
- Total lung volume > 45% of normal → predictive of survival
- Intrathoracic liver herniation significantly worsens prognosis
Prenatal diagnosis is associated with worse survival because only larger defects are visible on fetal imaging. — Sabiston Textbook of Surgery, p. 2716
Clinical Presentation
Neonatal (typical):
- Persistent respiratory distress at birth with grunting, dyspnea, retractions, and cyanosis
- Characteristic "seesaw" (side-to-side) respiratory pattern
- Scaphoid abdomen (bowel contents in thorax)
- Bowel sounds auscultated in the chest
- Displacement of heart tones
- Significant preductal–postductal SpO₂ difference (right-to-left shunting)
Delayed presentation (10–20% of cases): Diagnosed after 24 hours with feeding difficulties, respiratory distress, or recurrent pneumonia.
Morgagni hernias: Often diagnosed incidentally in childhood or adulthood; most are asymptomatic. — Tintinalli's Emergency Medicine
Chest X-Ray
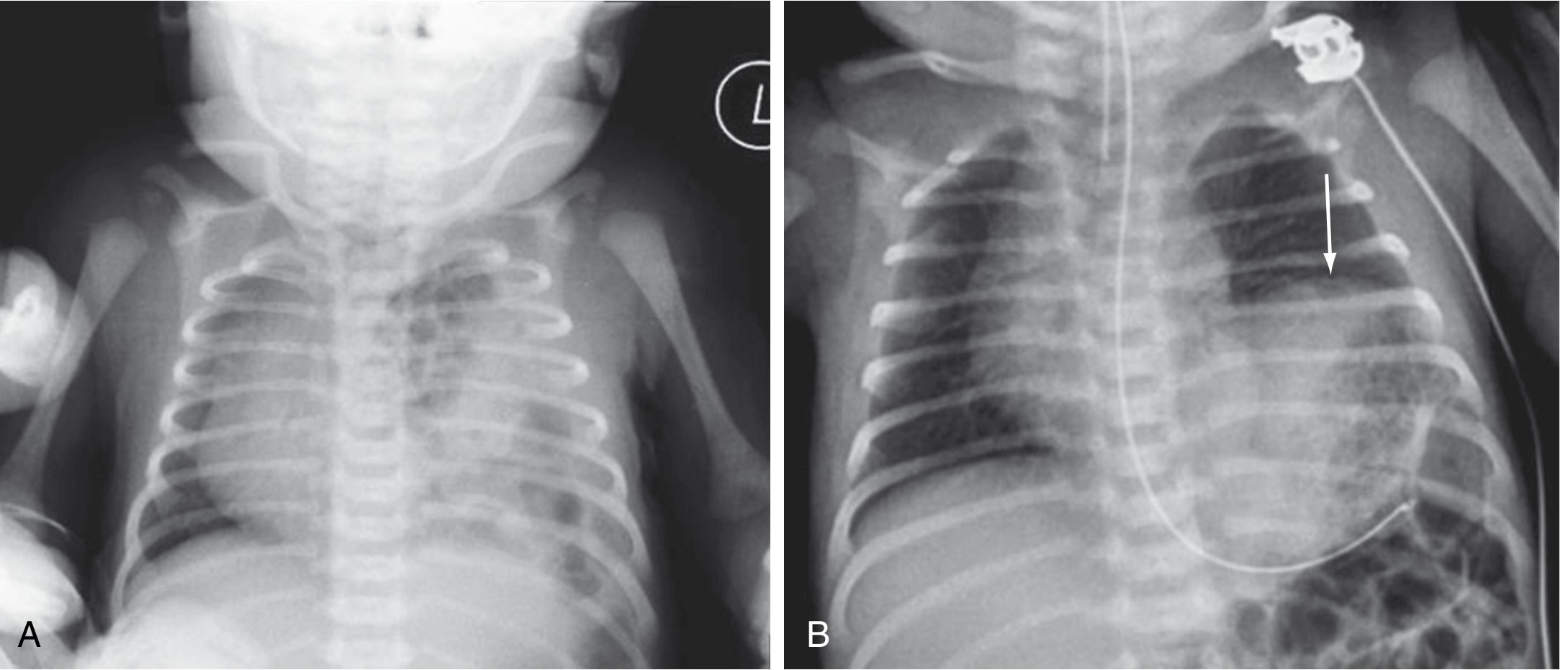
(A) Multiple gas-filled bowel loops in the left hemithorax with rightward mediastinal shift — classic CDH. (B) Left diaphragmatic eventration (arrow) from phrenic nerve injury-induced paralysis. — Sabiston Textbook of Surgery, p. 2675
Emergency Management
- Immediate endotracheal intubation — bag-mask ventilation is contraindicated (inflates GI contents in chest, worsening compression)
- Gentle ventilation: Rate 40–50 breaths/min, lowest peak inspiratory pressures that allow normal chest rise → prevents barotrauma to hypoplastic lungs
- Permissive hypercapnia with gentle hyperventilation targeting PCO₂ 30–35 mmHg to reduce pulmonary vascular resistance
- Large-bore orogastric tube (10F) on low continuous suction to decompress intrathoracic GI contents
- Chest and ABG to confirm diagnosis and guide stabilization
- Emergent referral to a pediatric specialty center — Tintinalli's Emergency Medicine
Definitive Management
Pulmonary hypertension treatment (pre-surgical stabilization):
- High-frequency oscillatory ventilation (HFOV)
- Inhaled nitric oxide (iNO)
- ECMO (extracorporeal membrane oxygenation) for refractory cases
- Vasodilators: PGE1, prostacyclin (PGI2), sildenafil (PDE-5 inhibitor), milrinone
Timing of surgical repair:
- Defer 48–72 hours after initial stabilization (not emergent)
- Allows treatment of pulmonary vascular lability before surgical stress
- In patients on ECMO: timing of repair remains controversial
Surgical approach:
- Open or minimally invasive (laparoscopic/thoracoscopic) repair
- Primary closure when possible; larger defects require prosthetic patch repair
- High-volume, protocolized centers have demonstrably improved outcomes
Overall survival: 65–90% — Sabiston Textbook of Surgery, p. 2675
Fetal Intervention: FETO
Fetal Endoluminal Tracheal Occlusion (FETO): Fetoscopic balloon placement in the trachea at 27–29 weeks to occlude airflow → accumulated lung fluid → stimulates lung growth.
Key trial results:
- Severe CDH (O/E LHR < 25%): TOTAL trial showed 40% survival with FETO vs. 15% with expectant management — stopped early for efficacy
- Moderate CDH (O/E LHR 25–34.9%): No significant survival benefit demonstrated
- Complications: Preterm labor, PPROM, premature birth, fetal demise
- Now offered at select fetal surgery centers in the US and Europe — Sabiston Textbook of Surgery, p. 2716
Summary Table
| Feature | Detail |
|---|---|
| Most common type | Bochdalek (posterior-lateral) |
| Most common side | Left (85%) |
| Key pathophysiology | Pulmonary hypoplasia + pulmonary hypertension |
| Key prenatal marker | O/E LHR, liver herniation |
| Clinical sign | Scaphoid abdomen + bowel sounds in chest |
| Emergency treatment | ETT intubation (NOT bag-mask) |
| Definitive treatment | Surgical repair (defer 48–72 h) |
| Survival | 65–90% |
This is a shared conversation. Sign in to Orris to start your own chat.