
0ffa3acd-15aa-4d55-85a2-111f65c3084f.jpg
Mild chest pain with discomfort 28 yrs male with no co morbidity vitals bp 110/70 pulse 96 bpm n spo2 99%
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a structured clinical analysis for this case:
ECG Analysis - 28-Year-Old Male, Mild Chest Pain/Discomfort
Vitals: BP 110/70 | Pulse 96 bpm | SpO2 99%
ECG Findings (Systematic Read)
| Parameter | Finding |
|---|---|
| Rate | ~75-80 bpm (sinus) |
| Rhythm | Regular sinus rhythm; 1 isolated PVC noted |
| Axis | Normal (~+30-60°) |
| P waves / PR | Normal morphology; PR ~140-160 ms, constant |
| QRS duration | Normal (<100 ms) - no bundle branch block |
| R-wave progression | Poor R-wave progression V1-V4 (transition delayed to V5-V6) |
| ST segments | Mild diffuse concave (saddle-shaped) ST elevation in V2-V5 and leads II/aVF, ~0.5-1 mm |
| T waves | Upright, concordant, asymmetric; no hyperacute or inverted T waves |
| Reciprocal changes | None clearly present (ST depression absent in opposing leads) |
| PR depression | Not prominently seen (needs close clinical correlation) |
Differential Diagnosis
The combination of diffuse, concave-upward ST elevation in a young male with chest discomfort narrows to three main differentials:
1. Benign Early Repolarization (BER) - Most Likely
- Classic presentation: young male, concave ST elevation maximal in V2-V5
- Upward concavity of ST segment at J-point; concordant tall T waves
- No reciprocal depression, no PR depression, hemodynamically stable
- Per Rosen's Emergency Medicine: BER characteristics include "(1) ST segment elevation; (2) upward concavity of the initial portion of the ST segment; (3) notching of the terminal portion of the QRS complex at the J point; (4) symmetric concordant T waves of large amplitude; (5) diffuse ST segment elevation; (6) relative temporal stability over the short term"
- Typically seen in V2-V5 in young men; J-point elevation usually <3.5 mm
2. Acute Pericarditis - Must Exclude
- Also presents with diffuse concave ST elevation, often in all leads except aVR
- Key distinguishing features favoring pericarditis:
- PR segment depression (most specific ECG sign - seen best in leads II and V6; PR elevation in aVR)
- Pleuritic character of pain (worse lying flat, better sitting forward)
- Pericardial friction rub on auscultation
- Recent viral prodrome (fever, URTI)
- Diagnosis requires ≥2 of 4 criteria: typical chest pain + pericardial rub + new widespread ST elevation + new/worsening pericardial effusion - per Goldman-Cecil Medicine
Below is the textbook comparison of BER (A) vs Pericarditis (B) ECG morphology:
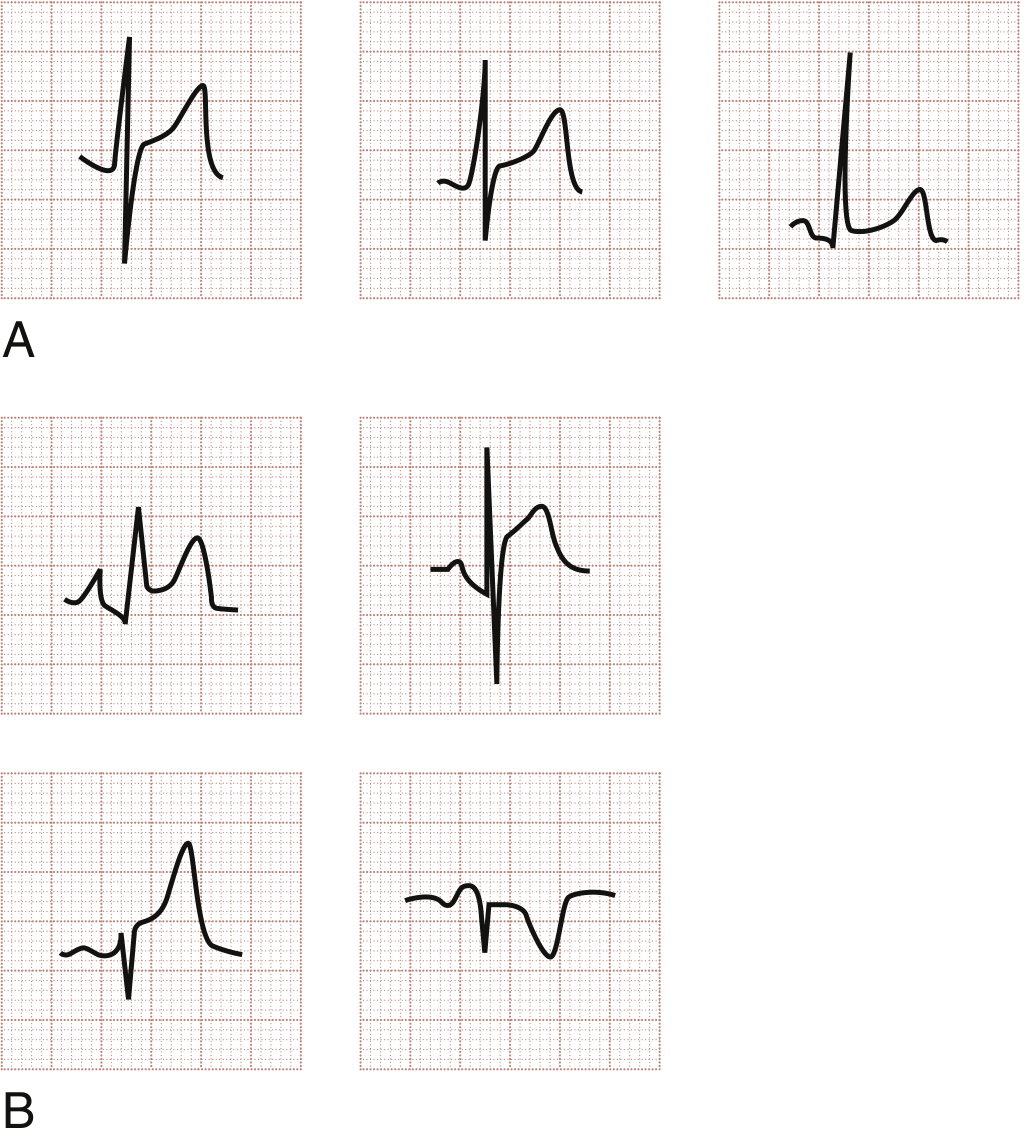
Fig. A = Benign Early Repolarization (concave STE, J-point notching); B = Acute Pericarditis (concave STE with PR segment depression)
3. Acute STEMI / ACS - Must Actively Exclude
- The young age (28), no risk factors, concave morphology, and absence of reciprocal changes all weigh against STEMI
- However, spontaneous coronary artery dissection (SCAD), coronary spasm, or anomalous coronary artery can cause MI in young patients
- Mandatory serial troponin testing before dismissing
Immediate Management Plan
Do now (all patients with chest pain + ST changes):
- Serial ECGs - repeat at 15-30 min intervals; look for dynamic changes
- High-sensitivity Troponin I/T - at 0h and 3h (or 0h/1h if hs-cTnI assay used)
- CXR - look for cardiomegaly, pulmonary edema, mediastinal widening
- Full blood work: CBC, CRP/ESR (elevated in pericarditis), BMP, LFTs
- Echocardiogram: check for pericardial effusion (supports pericarditis), wall motion abnormality (suggests ischemia)
History clues to obtain:
- Nature of pain - sharp/pleuritic vs pressure/squeezing?
- Positional change - better sitting forward? (pericarditis)
- Recent viral illness, fever, URTI in preceding 1-2 weeks?
- Family history of premature CAD or channelopathy
- Drug/substance use (cocaine - causes coronary spasm)
Likely Diagnosis
Given the patient's age, sex, hemodynamic stability, diffuse concave ST elevation without reciprocal changes, normal PR intervals, and mild symptoms, the most probable diagnosis is:
Benign Early Repolarization - a normal variant, requiring no treatment
However, acute pericarditis must be actively excluded clinically (check for pleuritic pain, fever, rub, CRP, echo), and ACS must be ruled out biochemically with serial troponins before discharge.
Clinical bottom line: Do not discharge this patient without serial ECGs, troponins x2, and a focused history for pericarditis features. If pericarditis is confirmed, treatment is NSAIDs + colchicine. If BER is confirmed and troponins are flat, reassurance is appropriate with cardiology follow-up.
Sources: Rosen's Emergency Medicine (9th ed.), Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.