Diphragmatic hernia in pedictrics surgery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I have the chest X-ray image and extensive content. The second read_file went past the CDH section. I have enough information from all three sources to compile a comprehensive answer. Let me now synthesize everything into a well-structured response.
Congenital Diaphragmatic Hernia (CDH) in Pediatric Surgery
Definition & Overview
Congenital diaphragmatic hernia (CDH) is a spectrum of developmental conditions marked by a diaphragmatic defect that allows abdominal contents to protrude into the thoracic cavity, disrupting lung and pulmonary vascular development. Survival has improved significantly to 65–90% with advances in neonatal care.
- Incidence: ~1:2,000–5,000 live births; most cases are sporadic, isolated, and non-syndromic
Embryology & Types
The diaphragm is embryologically derived from the septum transversum, pleuroperitoneal folds, components of the abdominal wall, and the dorsal mesentery. Fusion begins at 3–4 weeks of gestation and is typically complete by 9 weeks.
| Type | Location | Frequency |
|---|---|---|
| Bochdalek (posterolateral) | Most common; left-sided 85%, right 13%, bilateral 2% | 70–75% |
| Morgagni (retrosternal/anterior) | Less common | 23–28% |
| Central hernia | Rare | 2–7% |
Pathophysiology
- Herniated abdominal contents (stomach, bowel, occasionally liver) compress the developing ipsilateral lung
- Results in pulmonary hypoplasia — smaller bronchi, less bronchial branching, reduced alveolar surface area; both lungs are affected, though ipsilateral worse
- Pulmonary vasculature shows increased arteriolar smooth muscle thickness → persistent pulmonary hypertension of the newborn (PPHN)
- Severity of pulmonary hypoplasia and PPHN is the primary determinant of morbidity and mortality
- Associated anomalies (cardiac defects, chromosomal abnormalities) are present in 25–50% of cases
Prenatal Diagnosis & Prognostic Markers
Routine prenatal ultrasound can identify CDH as early as 15 weeks, with key features at 22–24 weeks:
- Mediastinal shift
- Juxta-cardiac gastric dilatation
- Polyhydramnios
- Liver herniation into the right chest (in right-sided CDH)
Prognostic Tools
| Marker | Interpretation |
|---|---|
| Lung-to-Head Ratio (LHR) | LHR <1 = poor prognosis; LHR >1.4 = ~100% survival |
| Observed/Expected LHR (O/E LHR) | O/E LHR <25% = <20% survival |
| Total fetal lung volume (TFLV) | <20th percentile indicates severe hypoplasia |
| Liver position | "Liver-up" (intrathoracic liver) = worse prognosis |
Chest X-Ray
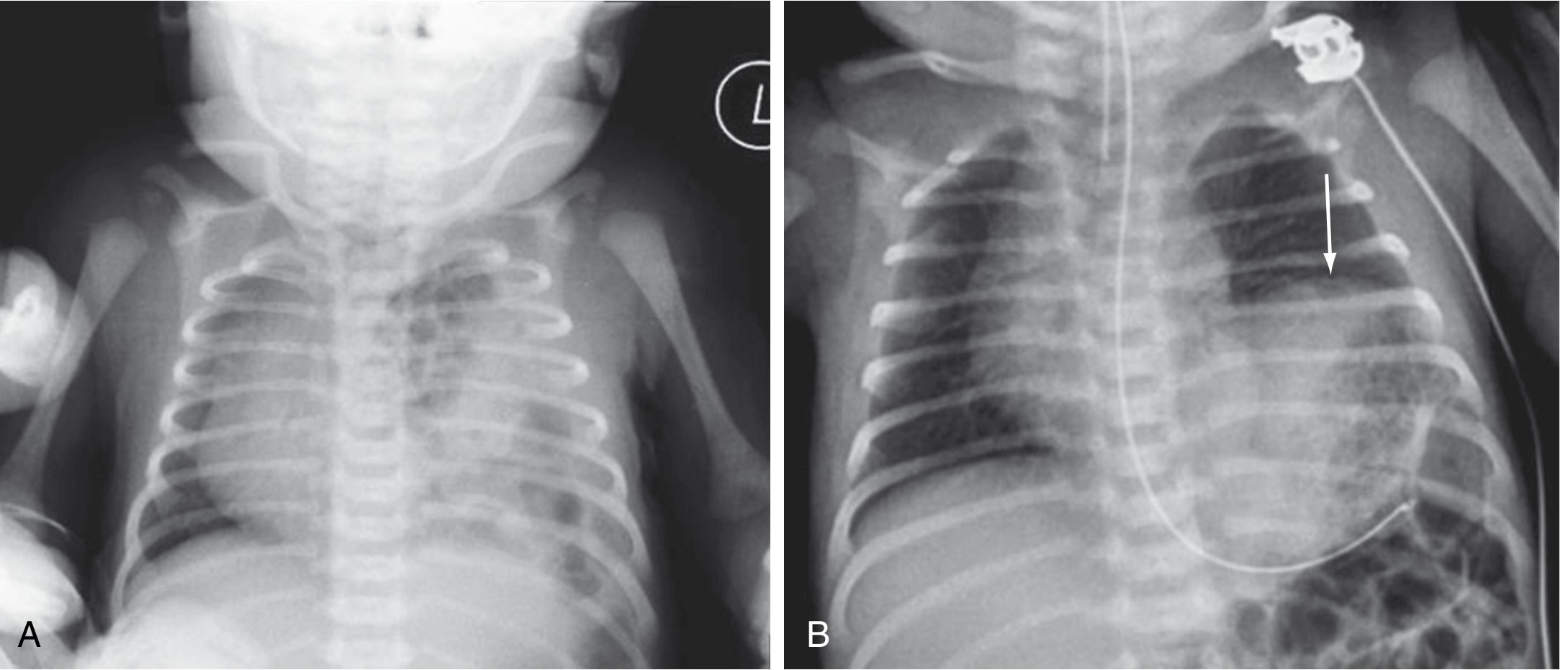
Left CDH: multiple gas-filled bowel loops in left hemithorax, mediastinum shifted to the right (Panel A). Panel B shows left diaphragmatic eventration (elevated hemidiaphragm, arrow) for comparison.
Clinical Presentation
The clinical hallmark is persistent respiratory distress at birth:
- "Seesaw" side-to-side respiratory pattern
- Halting, gasping respirations with persistent cyanosis
- Scaphoid abdomen (abdominal contents partially in the chest)
- Bowel sounds auscultated in the chest
- Chest X-ray is confirmatory — gas-filled loops in hemithorax, mediastinal shift
Fetal Intervention (Fetoscopic Endoluminal Tracheal Occlusion — FETO)
The rationale: the fetus normally expels lung fluid in utero; tracheal occlusion causes fluid accumulation → stimulates lung growth.
- Method: Fetoscopic balloon placement in the trachea (replacing older open surgical clips)
- TOTAL Trials (randomized controlled trials):
- Severe CDH (O/E LHR <25%): FETO showed significant benefit — 40% survival vs. 15% in expectant care → trial stopped early for efficacy
- Moderate CDH (O/E LHR 25–35%): No survival benefit of FETO at 30–32 weeks over expectant management
- First report of open fetal CDH repair: Harrison et al., 1990 (abdominal silo technique)
Postnatal Management
1. Initial Stabilization (Emergency)
- Immediate endotracheal intubation — bag-mask ventilation is contraindicated (inflates GI contents in chest, worsens compression)
- Ventilate at 40–50 breaths/min with lowest effective peak inspiratory pressures to prevent barotrauma to hypoplastic lungs
- Gentle hyperventilation targeting PaCO₂ 30–35 mmHg to reduce pulmonary vascular resistance
- Insert large-bore (10F) orogastric tube to low continuous suction (decompresses herniated GI contents)
- Chest and abdominal X-rays + arterial blood gas
2. Respiratory & Hemodynamic Support
- Gentle ventilation strategy — avoid high pressures; permissive hypercapnia (pH >7.2, PaCO₂ ≤65 mmHg)
- Inhaled nitric oxide (iNO) for PPHN management
- ECMO (Extracorporeal Membrane Oxygenation): reserved for severe cases failing conventional management
3. Surgical Repair
- Surgery is not an emergency — delayed repair after cardiorespiratory stabilization yields better outcomes
- Principles: reduce herniated contents, close the diaphragmatic defect
- Small defects: primary repair
- Large defects / absent hemidiaphragm: prosthetic patch repair (PTFE/Gore-Tex) or muscle flap
Surgical approaches:
- Open (subcostal or transabdominal): standard approach
- Minimally invasive (thoracoscopic/laparoscopic): increasingly used in stable patients; lower recurrence rates reported with open approach for large defects
Complications & Long-Term Morbidity
| Complication | Notes |
|---|---|
| Pulmonary hypertension | Major cause of early death |
| Recurrent hernia | Higher with patch repairs |
| Gastroesophageal reflux (GERD) | Very common long-term |
| Chest wall deformity | Scoliosis, pectus excavatum |
| Neurodevelopmental delay | Relates to ECMO use, prematurity, hypoxia |
| Pulmonary dysfunction | Obstructive/restrictive pattern |
| Nutritional failure / feeding difficulties | Especially in severe cases |
Summary of Key Points
- CDH is a posterior-lateral (Bochdalek) defect in 70–75%; left-sided in 85%
- Pathophysiology centers on pulmonary hypoplasia + PPHN
- Prenatal O/E LHR and liver position are the best prognostic predictors
- FETO improves survival in severe CDH (O/E LHR <25%)
- Postnatal: intubate immediately, avoid bag-mask, NGT decompression, ECMO if needed
- Surgical repair is elective after stabilization, not emergent
- Long-term morbidity is significant, particularly GERD, pulmonary dysfunction, and neurodevelopment
Sources: Sabiston Textbook of Surgery, pp. 2675–2678; Tintinalli's Emergency Medicine, p. 3954; Creasy & Resnik's Maternal-Fetal Medicine, p. 2716
This is a shared conversation. Sign in to Orris to start your own chat.