Everything about UTI in detail including pathophysiology with reference to standard textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough, well-organized answer.
Urinary Tract Infection (UTI) — Comprehensive Review
1. DEFINITION & CLASSIFICATION
A urinary tract infection (UTI) is the presence of microorganisms in the urinary tract causing an inflammatory response of the urothelium. UTIs are classified by:
By Location
| Type | Location | Key Features |
|---|---|---|
| Cystitis | Bladder (lower UTI) | Dysuria, frequency, urgency |
| Urethritis | Urethra | Dysuria, discharge |
| Pyelonephritis | Kidney/renal pelvis (upper UTI) | Fever, flank pain, systemic illness |
| Prostatitis | Prostate (male) | Perineal pain, obstructive symptoms |
By Complexity
- Uncomplicated UTI: Healthy, non-pregnant adult female with no structural/functional abnormality
- Complicated UTI: UTI in a patient with structural anomaly, obstruction, immunocompromise, pregnancy, diabetes, male sex, indwelling catheter, or renal transplant
- Recurrent UTI: ≥2 infections in 6 months, or ≥3 in 12 months
By Presence of Symptoms
- Symptomatic UTI (cystitis / pyelonephritis)
- Asymptomatic bacteriuria (ASB): Significant bacteriuria without symptoms — only treated in pregnancy and before urologic procedures
— Campbell Walsh Wein Urology, 3-Volume Set; Rosen's Emergency Medicine
2. EPIDEMIOLOGY
- UTIs account for >7 million outpatient visits annually in the United States; the second most common bacterial infection encountered in clinical practice
- Women are disproportionately affected: 50–60% of women experience at least one UTI in their lifetime
- Among young adults, the female-to-male ratio is approximately 30:1, equalizing after age 60 due to prostatic hypertrophy in men
- Prevalence of ASB in pregnancy is 2–10%; up to 30% of pregnant women with untreated ASB develop pyelonephritis
- Catheter-associated UTI (CAUTI) is the most common healthcare-associated infection
— Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine
3. ETIOLOGY & MICROBIOLOGY
Common Causative Organisms
| Organism | Key Features |
|---|---|
| Escherichia coli | Most common (>80% of community UTIs); expresses type 1 and P-fimbriae for adhesion |
| Staphylococcus saprophyticus | 2nd most common in young sexually active women |
| Klebsiella pneumoniae | Often hospital-acquired; ESBL strains common |
| Proteus mirabilis | Urease producer → struvite (triple phosphate) stones; staghorn calculi |
| Enterococcus faecalis | Common in hospital-acquired UTI, elderly |
| Pseudomonas aeruginosa | Nosocomial, catheter-associated |
| Candida spp. | Immunocompromised, long-term catheters, broad-spectrum antibiotic use |
Triple phosphate (struvite) crystals form when urease-producing organisms (Proteus, Ureaplasma urealyticum, Corynebacterium urealyticum) split urea → ammonia → alkalinize urine → precipitate struvite. — Comprehensive Clinical Nephrology, 7th Edition
4. PATHOPHYSIOLOGY
4.1 Routes of Infection
A. Ascending Route (Most Common)
The vast majority of UTIs arise via ascending colonization:
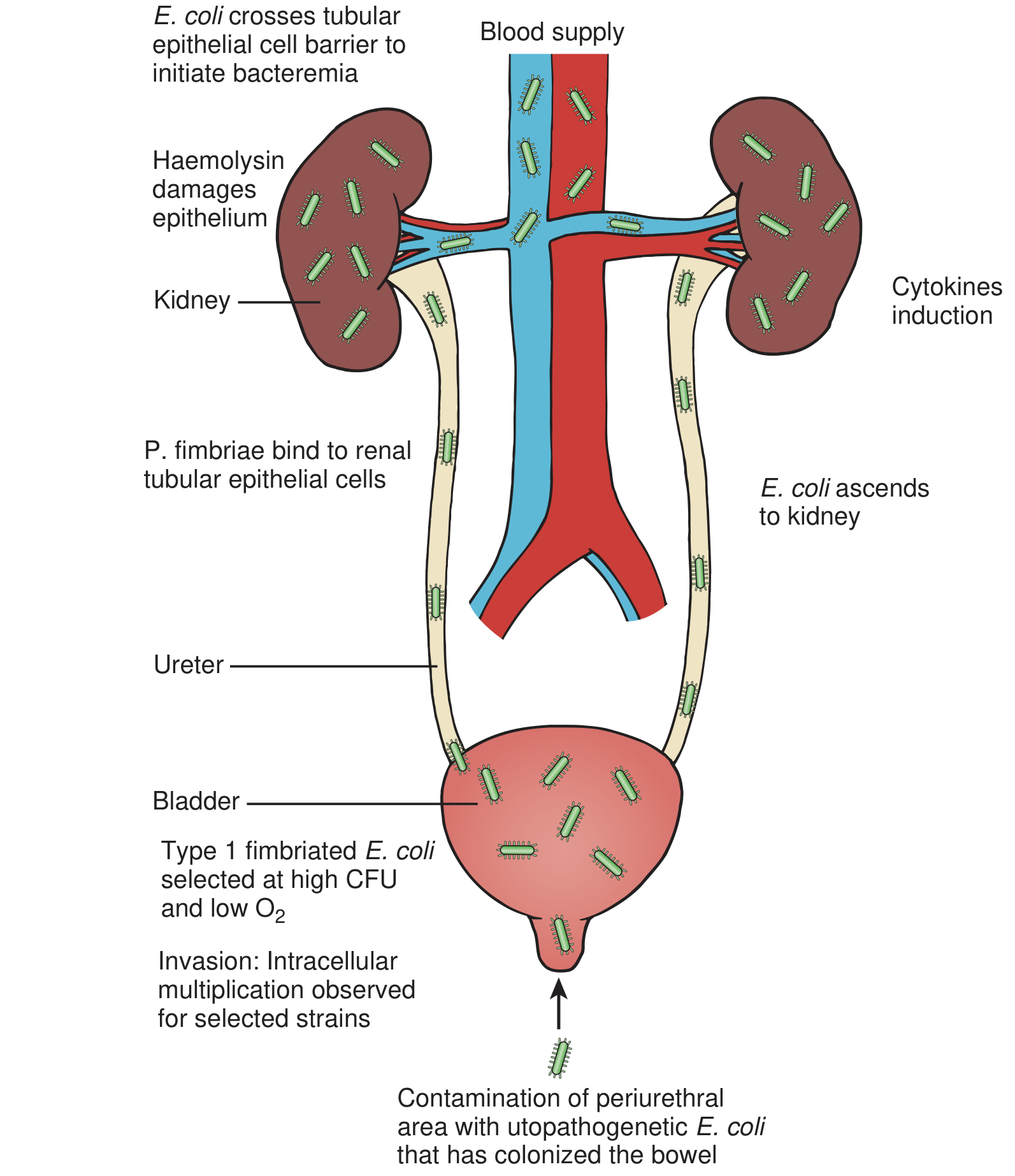
- Colonization of periurethral/vaginal flora — enteric gram-negative bacilli (principally E. coli) from bowel flora colonize the perineum and periurethral area
- Urethral ascent — bacteria enter the bladder via the urethra (short female urethra = critical risk factor)
- Bladder colonization — bacteria adhere to urothelium via adhesins (fimbriae)
- Ureteric ascent to kidney — bacteria ascend to the renal pelvis; reflux is not required but edema from cystitis can transiently impair the ureterovesical junction, promoting reflux
- Renal parenchymal invasion — bacteria enter collecting ducts at papillary tips, ascending within collecting tubules
"Most bacteria enter the urinary tract from the bowel and skin reservoir via ascent through the urethra into the bladder... Most episodes of pyelonephritis are caused by retrograde ascent of bacteria from the bladder through the ureter to the renal pelvis and parenchyma." — Campbell Walsh Wein Urology
Gram-negative bacterial endotoxins and pregnancy exert an anti-peristaltic effect on ureteral smooth muscle, facilitating ascending infection.
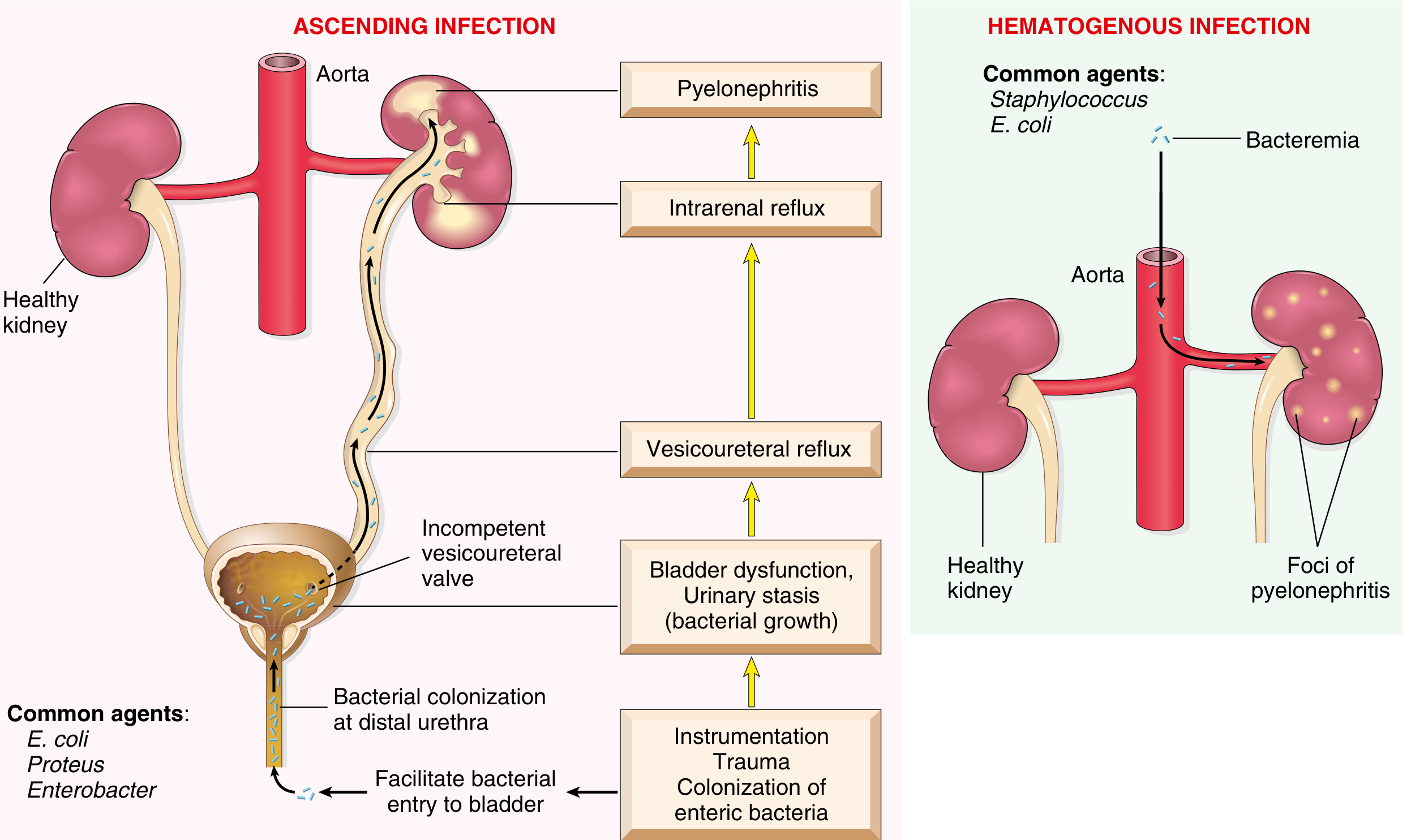
B. Hematogenous Route (Uncommon)
- Kidneys may be seeded via bacteremia — most commonly from S. aureus bacteremia (from skin/oral sources) or Candida fungemia
- Infection via this route is enhanced by urinary tract obstruction — Campbell Walsh Wein Urology
C. Lymphatic Route (Rare)
- Direct extension via lymphatics from adjacent organs (severe bowel infection, retroperitoneal abscess)
- Plays no significant role in the majority of UTIs
4.2 Bacterial Virulence Factors
E. coli possesses multiple virulence mechanisms that enable it to overcome host defenses:
| Virulence Factor | Function |
|---|---|
| Type 1 fimbriae (fim H) | Bind mannose-containing glycoproteins on urothelial cells (uroplakins); mediate cystitis |
| P-fimbriae (pap) | Bind globoside receptors on renal tubular/urothelial cells; critical for pyelonephritis |
| S-fimbriae | Bind sialic acid residues |
| Flagella | Aid motility and ascending spread |
| α-hemolysin (hlyA) | Pore-forming toxin; lysing epithelial cells and immune cells |
| Cytotoxic necrotizing factor-1 (CNF-1) | Disrupts actin cytoskeleton; promotes bacterial invasion |
| Iron acquisition (siderophores — aerobactin, enterobactin) | Scavenge iron for bacterial growth in iron-limited urine |
| Capsular polysaccharide (K antigen) | Resists complement-mediated killing and phagocytosis |
| LPS (O antigen / endotoxin) | Triggers inflammatory cascade; anti-peristaltic effect on ureter |
"The significance of epithelial cell receptivity in the pathogenesis of ascending UTI has been studied initially by examining adherence of E. coli to vaginal epithelial cells and uroepithelial cells." — Campbell Walsh Wein Urology
4.3 Host Defense Mechanisms
Normal host defenses that prevent UTI:
| Defense | Mechanism |
|---|---|
| Urine flow (washout) | Mechanical flushing; bacteria expelled during voiding |
| Urine properties | High osmolality, low pH, high urea, organic acids — bacteriostatic |
| Tamm-Horsfall protein (uromodulin) | Binds type 1 fimbriae of E. coli, trapping bacteria for excretion |
| Bladder mucosa | Antimicrobial properties; urothelium internalizes and eliminates bacteria |
| Secretory IgA | Inhibits bacterial adherence to mucosa |
| Normal vaginal flora (lactobacilli) | Acidic environment; produce H₂O₂; inhibit uropathogens |
| Ureteral peristalsis | Prevents reflux; propels urine downward |
| Ureterovesical junction (UVJ) | Functional anti-reflux valve |
| Prostatic secretions | Zinc-containing antibacterial compounds in males |
"In females, normal vaginal and periurethral flora contain microorganisms like lactobacillus that help prevent uropathogenic colonization. Unobstructed urinary flow with the subsequent washout of ascending bacteria is one of the most important defense mechanisms." — Smith and Tanagho's General Urology, 19th Edition
4.4 Risk Factors & Predisposing Conditions
Female anatomy is the dominant risk factor:
- Short urethra (4 cm vs 20 cm in males) — easy ascent
- Proximity of urethral meatus to rectum
| Risk Factor | Mechanism |
|---|---|
| Sexual intercourse | Mechanical inoculation of bacteria into bladder |
| Spermicide use | Disrupts Lactobacillus-dominated vaginal flora |
| Post-menopause | Loss of estrogen → loss of Lactobacillus; colonization by Enterobacteriaceae |
| Pregnancy | Ureteral smooth muscle relaxation (progesterone), vesical compression → stasis; up to 30% risk of pyelonephritis from ASB |
| Urinary obstruction (BPH, stricture, tumor) | Urinary stasis; bacteria multiply undisturbed |
| Vesicoureteral reflux (VUR) | Allows bladder bacteria access to upper tracts |
| Neurogenic bladder | Incomplete emptying; residual urine |
| Indwelling urinary catheter | Bypasses urethral defenses; forms biofilm |
| Diabetes mellitus | Immunosuppression; glycosuria (nutrient source); autonomic neuropathy → incomplete emptying |
| Immunocompromise | Reduced neutrophil and lymphocyte function |
| Renal transplant | Immunosuppression + surgical anastomosis |
| Spinal cord injury | Neurogenic bladder; catheter dependence |
"UTI is particularly frequent among patients with urinary tract obstruction, as may occur with benign prostatic hyperplasia and uterine prolapse." — Robbins & Kumar Basic Pathology
4.5 Inflammatory Response & Tissue Damage
Once bacteria colonize the bladder/kidney:
- Bacterial LPS activates Toll-like receptors (TLR4) on urothelial cells → NF-κB activation → IL-6, IL-8, TNF-α release
- IL-8 (CXCL8) recruits neutrophils into bladder tissue and urine (pyuria)
- Neutrophils phagocytose bacteria; degranulation causes local tissue damage
- In pyelonephritis: neutrophilic infiltration extends into tubular lumina → tubular destruction → focal areas of suppuration (microabscesses)
- Severe cases: cortical abscesses, papillary necrosis (especially in diabetes), perinephric abscess
- Chronic/recurrent pyelonephritis → fibrosis, cortical scarring, calyceal clubbing → reflux nephropathy / chronic pyelonephritis
5. CLINICAL FEATURES
Lower UTI (Cystitis)
- Dysuria (burning/painful micturition)
- Urinary frequency and urgency
- Suprapubic pain/tenderness
- Hematuria (gross or microscopic)
- Cloudy, malodorous urine
- No fever / systemic features in uncomplicated cystitis
Upper UTI (Acute Pyelonephritis)
- Fever (>38°C), rigors
- Flank/costovertebral angle tenderness
- Nausea, vomiting
- Malaise, myalgia
- Lower urinary tract symptoms may or may not be present
- Right side predominance in pregnancy (due to mechanical forces on right ureter)
Complicated/Severe UTI
- Sepsis (urosepsis) — tachycardia, hypotension, altered consciousness
- Complications: renal abscess, emphysematous pyelonephritis (gas-forming organisms in diabetics), papillary necrosis
"Acute pyelonephritis carries considerable morbidity in pregnancy, including maternal sepsis, permanent renal injury, and premature labor." — Rosen's Emergency Medicine
6. DIAGNOSIS
Urinalysis
| Finding | Significance |
|---|---|
| Pyuria (>5 WBC/hpf or >10 WBC/mm³) | Inflammation; hallmark of UTI |
| Bacteriuria | Significant infection |
| Nitrites (Griess test) | Gram-negative organism (converts nitrate to nitrite) |
| Leukocyte esterase | Proxy for pyuria (enzyme from neutrophils) |
| Hematuria | Bladder mucosal irritation |
| WBC casts | Pyelonephritis (pathognomonic) |
| Struvite crystals | Urease-producing organisms (Proteus) |
"Bacteria and leukocytes are the hallmarks of UTI... In patients with pyelonephritis, RTECs [renal tubular epithelial cells] and leukocyte casts can also be found. When the infection is caused by urease-producing bacteria such as Proteus spp., Ureaplasma urealyticum, and Corynebacterium urealyticum, triple phosphate (struvite) crystals are often present." — Comprehensive Clinical Nephrology, 7th Edition
"The finding of bacteria and leukocytes, together with a high number of squamous epithelial cells, suggests urine contamination from genital secretion rather than UTI." — Comprehensive Clinical Nephrology, 7th Edition
Urine Culture (Gold Standard)
- ≥10⁵ CFU/mL of a single uropathogen = significant bacteriuria (classic threshold)
- Lower thresholds valid: ≥10² CFU/mL in symptomatic women; ≥10³ CFU/mL in catheterized samples
- Essential for identifying organism + antibiotic sensitivities in complicated/recurrent UTI
Imaging
- Ultrasound: detect hydronephrosis, abscesses, structural abnormalities; first-line in pregnancy
- CT abdomen/pelvis (non-contrast): investigation of choice for suspected obstruction, pyelonephritis complications
- VCUG (voiding cystourethrogram): assess for VUR (children with febrile UTI)
- DMSA renal scan: gold standard for detecting renal cortical scars
7. MANAGEMENT
Uncomplicated Cystitis (Women)
| Antibiotic | Regimen | Notes |
|---|---|---|
| Nitrofurantoin | 100 mg BD × 5 days | First-line; avoid if CrCl <30 mL/min |
| Trimethoprim-sulfamethoxazole | 160/800 mg BD × 3 days | Use if local resistance <20% |
| Fosfomycin | 3 g single dose | Excellent for ESBL strains |
| Pivmecillinam | 400 mg TID × 3–5 days | Europe; good Gram-negative coverage |
| Fluoroquinolones | 3 days | Reserve for complicated infections |
Acute Uncomplicated Pyelonephritis
- Outpatient (mild-moderate): Oral ciprofloxacin 500 mg BD × 7 days; or TMP-SMX × 14 days
- Inpatient (severe / urosepsis): IV ciprofloxacin or ceftriaxone; step-down to oral when clinically improving
- Duration: 7–14 days
Complicated UTI
- Prolonged therapy (10–14 days); guided by culture and sensitivity
- Address underlying cause (relieve obstruction, remove catheter if possible)
- Urology referral for structural abnormalities
UTI in Pregnancy
- Treat all ASB (≥10⁵ CFU/mL) — prevents pyelonephritis in 30% of untreated cases
- Safe antibiotics: nitrofurantoin (avoid at term), amoxicillin-clavulanate, cefalexin
- Avoid fluoroquinolones (cartilage), tetracyclines (teeth/bones), TMP (folate antagonist in 1st trimester)
- Screen at 12–16 weeks or first prenatal visit (USPSTF Grade A recommendation)
"Because up to 30% of women who have asymptomatic bacteriuria will have pyelonephritis if they are untreated, the treatment of bacteriuria is cost-effective and important. Antibiotic treatment may also reduce the risk of preterm delivery and low birth weight." — Rosen's Emergency Medicine
Catheter-Associated UTI (CAUTI)
- Remove/replace catheter if possible
- Treat if symptomatic
- P. aeruginosa and Acinetobacter: urinary catheters/stents/stones should be removed; treat with ciprofloxacin or anti-pseudomonal β-lactam — Goldman-Cecil Medicine
8. RECURRENT UTI
- Reinfection (71–73%): new organism from external reservoir after eradication
- Relapse (27–29%): same organism, suggests inadequately treated source (e.g., renal calculus, prostate, abscess)
- Prevention strategies:
- Post-coital antibiotic prophylaxis
- Low-dose continuous prophylaxis (nitrofurantoin, TMP)
- Self-start therapy
- Behavioral: adequate hydration, post-coital voiding, avoidance of spermicides
- Vaginal estrogen therapy in post-menopausal women
- Cranberry products (modest benefit — inhibit type 1 fimbriae adhesion)
9. COMPLICATIONS
| Complication | Key Points |
|---|---|
| Urosepsis | Gram-negative bacteremia; endotoxin-mediated shock |
| Renal abscess | Failure to respond to antibiotics; drainage required |
| Perinephric abscess | Extension through renal capsule; CT-guided drainage |
| Emphysematous pyelonephritis | Gas-forming infection (E. coli, Klebsiella) in diabetics; emergency nephrectomy may be needed |
| Renal papillary necrosis | Especially in diabetics; ischemic necrosis of papillae; calyceal filling defects on imaging |
| Chronic pyelonephritis | Cortical scarring, calyceal clubbing, hypertension, CKD |
| Reflux nephropathy | VUR + UTI → cortical scars → progressive renal insufficiency |
| Preterm labor | Pyelonephritis in pregnancy; aggressive treatment essential |
"Renal papillary necrosis... Multiple predisposing conditions have been associated with development of RPN, particularly diabetes, analgesic abuse, sickle cell hemoglobinopathy, and obstruction." — Campbell Walsh Wein Urology
10. SPECIAL POPULATIONS
UTI in Children
- Febrile UTI in children suggests pyelonephritis; must be investigated for VUR
- Incidence of UTI in children with prenatal hydronephrosis: 4–40% depending on grade of dilation
- Risk factors: uncircumcised male, VUR, neurogenic bladder, anatomical anomalies
UTI in Spinal Cord Injury
- Occurs in virtually 100% of patients with SCI over long-term follow-up
- Risk factors: male sex, cervical-level injury, indwelling catheter (worst outcomes vs. CIC or spontaneous voiding)
- 34% develop pyelonephritis; 25% develop renal stones; 32% experience upper tract deterioration
UTI in Diabetes
- Higher incidence in women; upper tract involved in ~80%
- More severe infections: emphysematous pyelonephritis, papillary necrosis
- Contributory: incomplete bladder emptying, impaired immunity, antibiotic-driven resistant organisms — Campbell Walsh Wein Urology
11. KEY PATHOLOGICAL FINDINGS (Histology)
Acute Cystitis: Mucosal hyperemia, edema, neutrophilic infiltration of lamina propria; epithelial ulceration in severe cases
Acute Pyelonephritis (Robbins):
- Gross: Pale, raised abscesses on cortical surface; suppurative destruction of renal parenchyma
- Micro: Neutrophilic infiltration of tubular lumina (intra-tubular neutrophils = pathognomonic); microabscesses; glomeruli relatively spared early
- Leukocyte casts in collecting tubules — appear in urine
Chronic Pyelonephritis:
- Asymmetric corticomedullary scarring
- Calyceal clubbing (blunting of calyces underlying scars)
- Tubular atrophy, interstitial fibrosis
- "Thyroidization" of tubules (colloid-like casts resembling thyroid follicles)
- Periglomerular fibrosis
SUMMARY
UTI represents a spectrum from uncomplicated cystitis to life-threatening urosepsis. The cornerstone of pathophysiology is ascending infection — colonization by enteric uropathogens (chiefly E. coli) that overcome host defenses via adhesins, toxins, and immune-evasion mechanisms. Host factors (female anatomy, obstruction, vesicoureteral reflux, pregnancy, diabetes, catheterization) tip the balance in favor of infection. Management is guided by site, complexity, patient population, and local resistance patterns.
Key References:
- Campbell Walsh Wein Urology, 3-Volume Set (Wein et al.)
- Robbins & Kumar Basic Pathology (Kumar et al.)
- Comprehensive Clinical Nephrology, 7th Edition
- Smith and Tanagho's General Urology, 19th Edition
- Rosen's Emergency Medicine — Concepts and Clinical Practice
- Goldman-Cecil Medicine International Edition
This is a shared conversation. Sign in to Orris to start your own chat.