Dialysis tpe filter
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the dialysis filter (dialyzer) — the core component of hemodialysis:
The Dialysis Filter (Dialyzer)
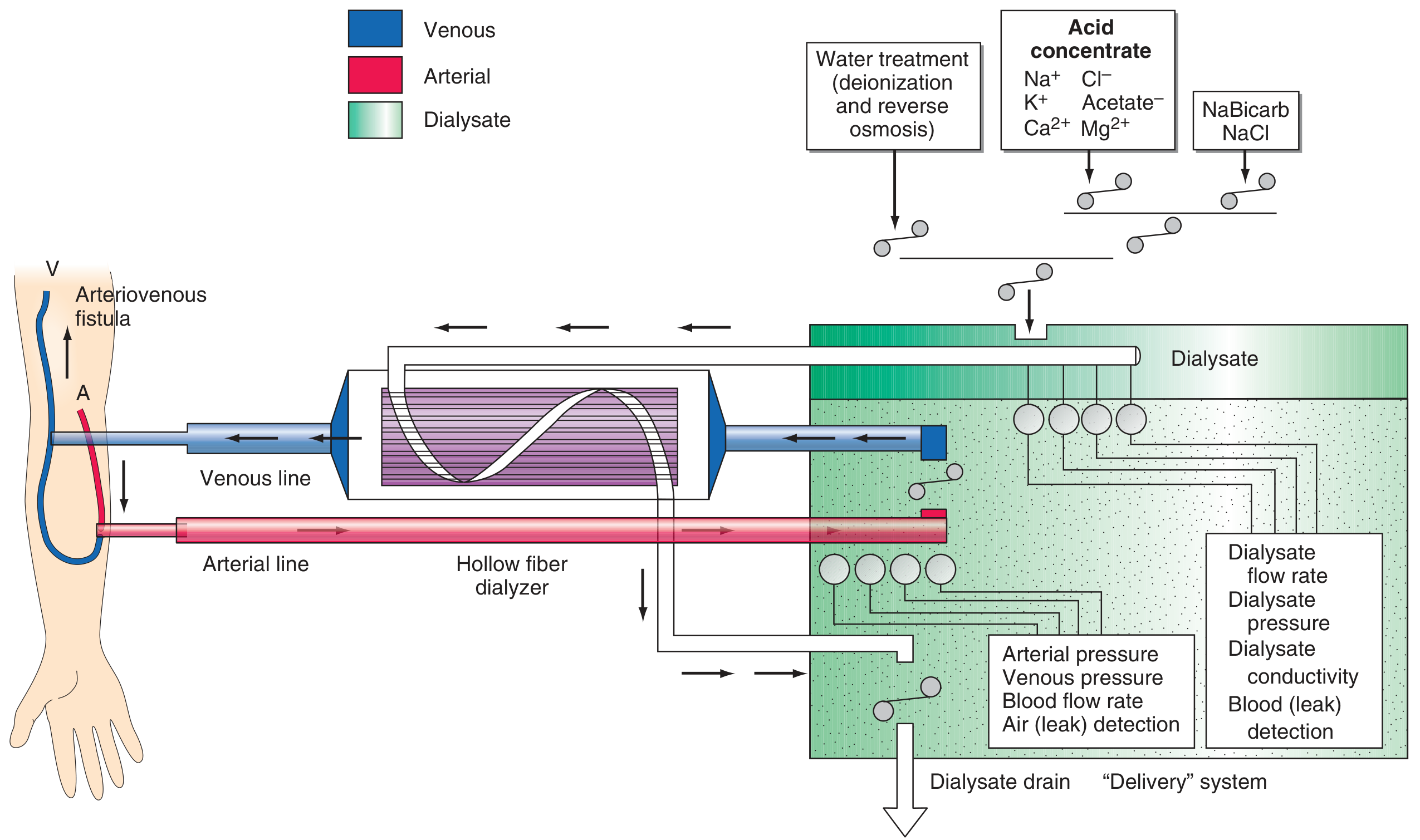
Schema for hemodialysis — Harrison's Principles of Internal Medicine 22E
What It Is
The dialyzer is the artificial kidney — a plastic chamber that simultaneously perfuses blood and dialysate compartments at high flow rates. The most common type used today is the hollow-fiber dialyzer, made up of bundles of capillary tubes through which blood flows while dialysate circulates on the outside in a countercurrent direction (maximizing the concentration gradient).
Membrane Materials
| Type | Examples | Notes |
|---|---|---|
| Synthetic (modern standard) | Polysulfone, polyacrylonitrile, polycarbonate, polyamide, polymethylmethacrylate | Biocompatible; do not activate complement |
| Cellulose-based (older) | Cellulose acetate | Bioincompatible — activates complement cascade; largely phased out |
Virtually all dialyzers now manufactured in the US use synthetic membranes. — Harrison's Principles of Internal Medicine 22E
How Transport Works
Two mechanisms move solutes across the membrane:
- Diffusion (concentration gradient) — drives clearance of small solutes like urea, potassium, creatinine
- Convection (hydrostatic pressure gradient) — drives ultrafiltration (fluid removal); also clears mid-size molecules
- Only the free fraction of protein-bound solutes crosses the membrane (unless albumin-leaky membranes are used)
- Solute flux is also affected by charge and blood-side protein concentration (Gibbs-Donnan effect)
Key Performance Parameters
| Parameter | Definition | Clinical Significance |
|---|---|---|
| Surface area | Usually 0.8–2.1 m² | Larger area = more efficient clearance |
| KoA (mass transfer area coefficient) | Theoretical max urea clearance (mL/min) | Low <500, Moderate 500–700, High >700 mL/min |
| Ultrafiltration coefficient (Kuf) | mL of fluid removed/h/mmHg | High-flux dialyzers: Kuf up to 80 mL/h/mmHg |
| Flux classification | Low-flux vs. high-flux vs. medium cut-off | High-flux/MCO membranes can remove β₂-microglobulin (11,800 Da), TNF-α (17 kDa), and larger uremic toxins |
Dialyzer Choice Criteria
When selecting a dialyzer, three factors are most critical:
- Solute clearance capacity — urea is the standard reference solute; in vivo clearance may be lower than manufacturer in vitro values due to protein binding, membrane adsorption, and Gibbs-Donnan effects
- Fluid removal (UF) capacity — the UF coefficient; in vivo values may vary ±10–20% from in vitro
- Biocompatibility — synthetic membranes are most inert; bioincompatible membranes activate coagulation, complement, and platelets
Additional considerations:
- Thrombogenicity: activated thrombin adsorbs to the membrane; heparin-bonded dialyzers may reduce thrombosis in anticoagulation-free HD
- Reuse: bleach (used for reprocessing) can enlarge pores of synthetic membranes → protein loss; heat disinfection can crack dialyzer headers
— Brenner and Rector's The Kidney, Comprehensive Clinical Nephrology 7th Ed.
Safety Monitors Integrated with the Filter Circuit
- Prepump (arterial) pressure: overly negative → arterial inflow problem
- Postpump pressure: elevated → dialyzer clotting
- Venous pressure: elevated → venous obstruction; normal venous pressure does NOT exclude venous needle dislodgement
- Air detector: clamps venous line and stops pump if air is detected
- Blood leak detector: placed in dialysate outflow to detect membrane rupture
Blood and Dialysate Flow
- Blood flow: 250–450 mL/min
- Dialysate flow: typically 500–800 mL/min, configured countercurrent to blood flow
- Countercurrent configuration maximizes diffusion gradient throughout the dialyzer length; co-current flow reduces small solute clearance by ~10%
— Comprehensive Clinical Nephrology 7th Ed., Harrison's 22E, Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.