Esophageal atersia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer. Let me synthesize it.
Esophageal Atresia (EA)
Esophageal atresia is a loss of continuity between the upper and lower esophagus, most commonly associated with a tracheoesophageal fistula (TEF). It is the most common developmental anomaly of the esophagus.
Incidence & Embryology
- Incidence: 1 in 3,000–4,500 neonates; ~⅓ of affected infants are premature
- EA results from deviation of the tracheoesophageal septum posteriorly and incomplete separation of the esophagus from the laryngotracheal tube
- Isolated atresia (no fistula) results from failure of esophageal recanalization during the 8th week of development
- TEF results from failure of the lung bud to separate completely from the foregut
- Key signaling pathway: Sonic Hedgehog (SHH) — disruption impairs separation of respiratory and digestive tracts
- Associated gene mutations: N-MYC (MYCN), SOX2, CHD7
— The Developing Human: Clinically Oriented Embryology; Sleisenger and Fordtran's GI and Liver Disease, p. 708–709
Classification (5 Types)
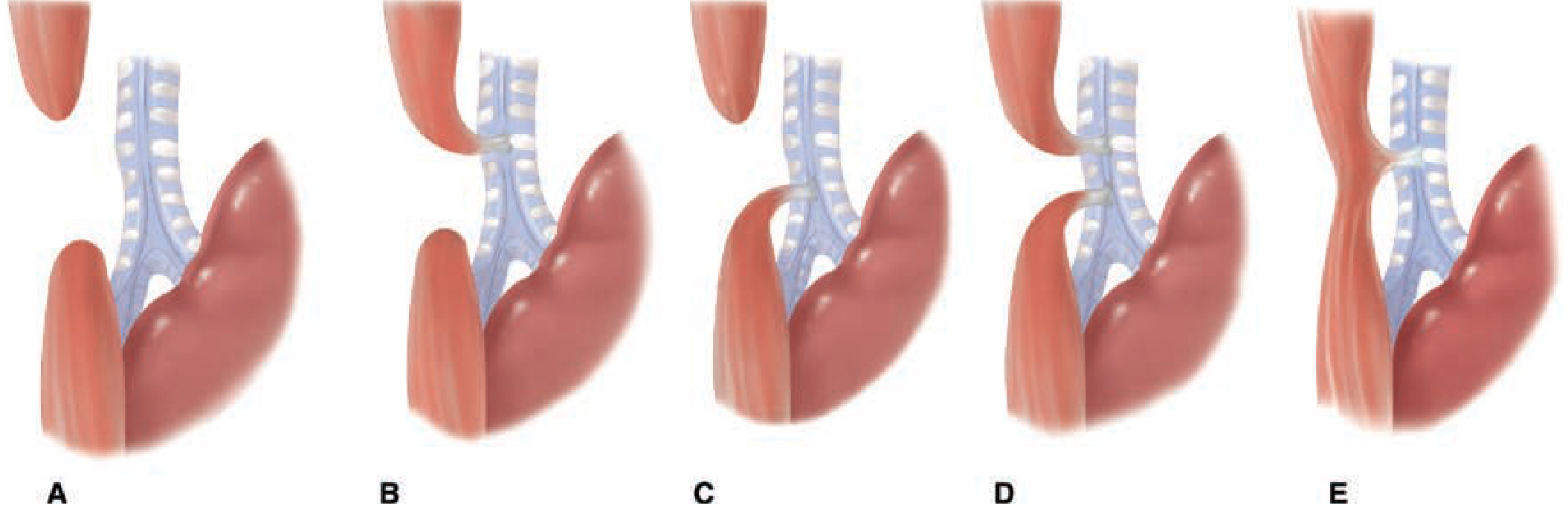
Figure: The five varieties of EA and TEF. — Schwartz's Principles of Surgery, 11th ed.
| Type | Description | Frequency |
|---|---|---|
| A | Pure esophageal atresia (no fistula) | 8–10% |
| B | EA with TEF between proximal esophagus and trachea | ~1% |
| C | EA with TEF between distal esophagus and trachea (most common) | ~85% |
| D | EA with TEF at both proximal and distal ends | ~2% |
| E | TEF without EA ("H-type fistula") | ~8% |
— Schwartz's Principles of Surgery, 11th ed.
Associated Anomalies
Up to 80% of EA cases have associated anomalies, particularly in the VACTERL association:
- Vertebral anomalies (absent or hemi-vertebrae)
- Anal/anorectal defects (imperforate anus) — 8%
- Cardiac malformations — 38% (most important predictor of survival)
- TracheoEsophageal fistula
- Renal anomalies — 15%
- Limb defects — 19% skeletal
Other associated syndromes include CHARGE (CHD7), Feingold syndrome (MYCN), Fanconi anemia, and Anophthalmia-esophageal-genital syndrome (SOX2).
Clinical Features
Prenatal clues:
- Polyhydramnios (fetus cannot swallow amniotic fluid → fluid accumulates) — present in ~⅔ of cases
- Failure to visualize the stomach on ultrasound
Postnatal presentation:
- Excessive drooling/salivation shortly after birth
- Immediate regurgitation and coughing upon first feed
- Choking and cyanosis with feeding
- Air transmitted through fistula → abdominal distension as infant cries/coughs
- In type C/D: gastric juice refluxes through fistula → chemical pneumonitis
The H-type fistula (type E) often presents later in infancy/childhood with recurrent chest infections and coughing during feeds.
— Schwartz's Principles of Surgery; The Developing Human
Diagnosis
- Inability to pass an orogastric/nasogastric tube into the stomach — strongly suggestive
- Chest X-ray: tube coiled in the upper esophageal pouch; air in the GI tract confirms distal TEF
- Contrast esophagram: confirms diagnosis; occasionally demonstrates fistula
A soft feeding tube will coil in the upper pouch, providing diagnostic certainty. An esophageal perforation (false passage at the piriform sinus) must be excluded if the tube fails to pass.
— Schwartz's Principles of Surgery
Initial Management
- Place neonate in infant warmer with head elevated ≥30°
- Sump catheter in upper pouch on continuous suction (prevents aspiration)
- Echocardiography — assess cardiac anatomy and aortic arch side (influences surgical approach)
- Plain radiographs for vertebral anomalies; renal ultrasound; check for patent anus
- Surgery is rarely a surgical emergency — can be deferred 1–2 days to stabilize
Special concern in premature/ventilated infants: Elevated airway pressures force air through the fistula into the stomach → progressive abdominal distension → impaired lung expansion → cardiopulmonary deterioration.
Surgical Repair
- Historical milestone: First successful primary anastomosis by Dr. Cameron Haight (University of Michigan, 1943)
- Standard approach: Ligation of the TEF + primary esophageal anastomosis (thoracoscopic or open)
- Right-sided or left-sided thoracotomy depending on aortic arch position
Prognosis:
- In infants >2 kg without significant cardiac anomalies: survival approaches 100%
- As birth weight decreases and cardiac defects become more severe, survival may fall to as low as 1%
— Schwartz's Principles of Surgery, 11th ed.; The Developing Human
This is a shared conversation. Sign in to Orris to start your own chat.