
1000321367.jpg
Answer accordingly to the marks if possible provide with the images n flowcharts give answer of questions 1-2 for 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
I now have all the information needed to write comprehensive, exam-quality answers. Let me compose the full answers.
MICROBIOLOGY - PAPER I (RS-4 & RS-5)
Long Essay Answers (10 Marks Each)
QUESTION 1 — Visceral Leishmaniasis (Kala-azar)
Clinical Diagnosis: The bone marrow aspirate showing amastigotes filled within a macrophage on Giemsa stain is pathognomonic. This is Visceral Leishmaniasis (Kala-azar).
a) Etiological Agent and Clinical Diagnosis
| Feature | Details |
|---|---|
| Etiological Agent | Leishmania donovani |
| Clinical Diagnosis | Visceral Leishmaniasis (Kala-azar / "Dum-dum fever" / "Black fever") |
| Vector | Female Phlebotomus sandfly |
| Reservoir | Rodents, dogs, wild canids (humans also act as reservoir in India) |
Morphological forms:
- Amastigote (Leishman-Donovan body / LD body): Oval, 2-3 μm, intracellular form found inside macrophages; has a nucleus and a rod-like kinetoplast appearing as a "dot and dash" on Giemsa stain
- Promastigote: Elongated, flagellated, found in sandfly gut and culture media
Histopathology image - L. donovani amastigotes (arrows) from a liver biopsy:
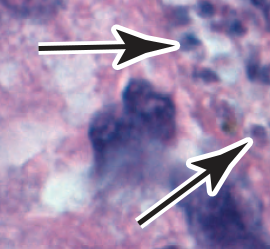
(Arrows point to amastigotes [LD bodies] within macrophage cytoplasm - Medical Microbiology, Jawetz 28e)
b) Life Cycle and Pathogenesis of Leishmania donovani
Life Cycle Flowchart:
SANDFLY (Phlebotomus) — Female sandfly bites infected host
│
▼
Ingests amastigotes from blood/macrophages
│
▼
SANDFLY MIDGUT: Amastigotes transform into → PROMASTIGOTES (flagellated)
│
▼
Promastigotes multiply by binary fission, migrate to proboscis
│
▼
Sandfly bites new host — injects PROMASTIGOTES into skin
│
▼
HUMAN HOST: Promastigotes phagocytosed by neutrophils/macrophages
│
▼
Inside phagolysosome: Promastigotes → transform to AMASTIGOTES
│
▼
Amastigotes multiply within macrophages (resist lysosomal killing)
│
▼
Infected macrophages burst → amastigotes released
│
▼
Taken up by other macrophages → spread via lymphatics/bloodstream
│
▼
Reticuloendothelial system (RES): Spleen, Liver (Kupffer cells),
Bone marrow, Lymph nodes → massive colonization
│
▼
KALA-AZAR: Hepatosplenomegaly, Pancytopenia, Fever, Weight loss
Pathogenesis:
- Entry: Promastigotes injected by sandfly are phagocytosed by skin macrophages
- Intracellular survival: L. donovani inhibits phagolysosome fusion and resists oxidative killing - the parasite lives and multiplies as amastigotes in macrophage cytoplasm
- Dissemination: Infected macrophages carry the parasite via lymphatics to the liver, spleen, bone marrow, and lymph nodes (RES organs)
- Hyperplasia of spleen: Marked splenomegaly due to RES proliferation
- Bone marrow suppression: Amastigotes fill bone marrow macrophages → pancytopenia (anaemia, leukopenia, thrombocytopenia)
- Immune dysregulation: Defective cell-mediated immunity (CMI), polyclonal B-cell activation → hypergammaglobulinemia
- Fever: Irregular, hectic fever due to cytokine release (IL-1, TNF)
- Post-kala-azar dermal leishmaniasis (PKDL): Occurs 1-2 years after treatment in Indian kala-azar - cutaneous vesicles with abundant parasites
Clinical Features Summary:
- Prolonged irregular fever (>2 weeks)
- Progressive weight loss and cachexia
- Massive splenomegaly (most prominent sign) + hepatomegaly
- Pancytopenia → anaemia, bleeding tendency, susceptibility to infections
- Hyperpigmentation of skin (hence "Kala-azar" = black fever in Hindi)
- Hypoalbuminemia and hypergammaglobulinemia
c) Laboratory Diagnosis of Visceral Leishmaniasis
Flowchart - Laboratory Diagnosis:
SUSPECTED KALA-AZAR
│
┌────┴────────────────────────────────────┐
│ │
PARASITOLOGICAL SEROLOGICAL /
METHODS IMMUNOLOGICAL
│ │
├─ Bone Marrow Aspirate (GOLD ├─ rK39 ICT strip test
│ STANDARD): Giemsa stain │ (Rapid, field diagnosis)
│ → LD bodies in macrophages │
│ ├─ DAT (Direct Agglutination Test)
├─ Splenic Aspirate: │
│ Most sensitive (>95%) ├─ ELISA (anti-Leishmania Ab)
│ but risk of bleeding │
│ ├─ CFT (Complement Fixation Test)
├─ Liver Biopsy: │ - Chopra's aldehyde test
│ Less sensitive than spleen │ (turbidity in hypergammaglobu-
│ │ linaemia - non-specific)
├─ Lymph node aspirate │
│ └─ Leishmanin (Montenegro)
├─ Peripheral blood smear (buffy coat) skin test: NEGATIVE in
│ - less sensitive active disease (CMI depressed)
│
├─ NNN CULTURE MEDIUM: Promastigotes
│ visible in 1-4 weeks
│
└─ PCR: Sensitive and specific,
detects Leishmania DNA in blood/
tissue. Used for species ID
│
MOLECULAR
METHODS
│
└─ PCR on blood, bone marrow, or
splenic aspirate
Supporting Hematological Findings:
| Parameter | Finding |
|---|---|
| Hemoglobin | Low (normocytic normochromic anaemia) |
| WBC | Leukopenia |
| Platelets | Thrombocytopenia |
| ESR | Elevated |
| Serum proteins | Low albumin; High globulin (IgG) |
| Formol-gel (Napier's) test | Positive (due to hyperglobulinaemia - white precipitate with formalin) |
Sources: Medical Microbiology 9e (Murray); Jawetz Melnick & Adelberg's Medical Microbiology 28e
QUESTION 2 — Bacillary Dysentery (Shigellosis)
Clinical Diagnosis: A 25-year-old with fever, tenesmus, blood/mucus in stools, pus cells on microscopy, no ova/cysts, and non-lactose fermenting colonies on stool culture = Bacillary Dysentery caused by Shigella spp.
a) Etiological Agent
| Feature | Details |
|---|---|
| Organism | Shigella species |
| Common species | S. flexneri (developing countries - most common), S. sonnei (developed countries), S. dysenteriae (most severe), S. boydii |
| Morphology | Gram-negative, non-motile, non-capsulated rod; facultative anaerobe |
| Biochemistry | Non-lactose fermenter (key clue in case!), oxidase-negative |
| Antigens | O (somatic) antigen used for serogroup classification |
| Minimum infective dose | As few as 10-100 organisms (very low infectious dose) |
b) Pathogenesis and Complications
Pathogenesis Flowchart:
INGESTION of ≥10-100 Shigella organisms (fecal-oral route)
│
▼
Reach SMALL INTESTINE → Initial colonization
│
▼
Produce ENTEROTOXIN → early WATERY DIARRHEA
(first 12-24 hours)
│
▼
Bacteria reach COLON (large intestine)
│
▼
Invade M-cells (Microfold cells) overlying Peyer's patches
via TYPE III SECRETION SYSTEM (T3SS)
│
▼
T3SS injects IpaA, IpaB, IpaC, IpaD proteins into epithelial cells
│
▼
Membrane RUFFLING → Macropinocytosis → Bacterial engulfment
│
▼
Shigella LYSE the phagosome → escape into CYTOPLASM
(unlike Salmonella which stays in vacuole)
│
▼
ACTIN POLYMERIZATION propels bacteria cell-to-cell
(protected from immune clearance)
│
▼
Induce APOPTOSIS of macrophages → release IL-1β
│
▼
IL-1β attracts NEUTROPHILS (PMNs) → mucosal inflammation
(pus cells in stool!)
│
▼
Disruption of INTESTINAL WALL INTEGRITY
│
▼
BLOODY DYSENTERY: Blood, mucus, pus in stool
Severe cramps + Tenesmus (painful urge to defecate)
│
▼
S. dysenteriae: SHIGA TOXIN (AB5 toxin)
B subunits → bind Gb3 receptor on endothelial cells
A subunit → cleaves 28S rRNA → BLOCKS PROTEIN SYNTHESIS
│
▼
Intestinal epithelial damage + (in small subset) Glomerular
endothelial damage → HEMOLYTIC UREMIC SYNDROME (HUS)
Shiga Toxin Mechanism:
- Structure: 1 A subunit + 5 B subunits (AB5 toxin)
- Receptor: B subunits bind glycolipid Gb3 on host cells
- Action: A subunit cleaves 28S rRNA of 60S ribosomal subunit → blocks aminoacyl-tRNA binding → inhibits protein synthesis → cell death
Complications:
| Complication | Details |
|---|---|
| HUS | Hemolytic uremic syndrome - S. dysenteriae Shiga toxin; triad: microangiopathic hemolytic anemia + thrombocytopenia + renal failure |
| Reactive arthritis (Reiter syndrome) | Weeks after infection; HLA-B27 association |
| Septicemia | Rare, mainly in malnourished children |
| Toxic megacolon | Especially S. dysenteriae |
| Pseudomembranous colitis | |
| Intestinal perforation | Severe cases |
| Seizures/Encephalopathy | Ekiri syndrome (especially in children) |
| Nutritional deficiency | Protein-losing enteropathy |
c) Laboratory Diagnosis
Flowchart - Laboratory Diagnosis of Shigellosis:
CLINICAL SUSPICION (fever + tenesmus + bloody-mucoid stools)
│
┌─────────┴────────────────────────┐
│ │
MICROSCOPY CULTURE
(Immediate) (Definitive)
│ │
├─ Stool wet mount: Collect FRESH stool
│ • Abundant pus cells (PMNs) │
│ • RBCs ├─ MacConkey agar:
│ • Mucus │ PALE/COLORLESS colonies
│ • NO cysts/ova │ (non-lactose fermenter)
│ (distinguishes from │
│ parasitic dysentery) ├─ XLD (Xylose Lysine
│ │ Deoxycholate) agar:
├─ Giemsa stain (PMNs, │ Pink/red colonies
│ intracellular bacteria │ (no H2S - no black center)
│ in severe cases) │
│ ├─ Hektoen Enteric (HE) agar:
│ │ Green colonies
│ │
│ ├─ Selenite F broth: enrichment
│ │
│ └─ BIOCHEMICAL ID:
│ • Glucose fermented (acid, no gas)
│ • Lactose: NOT fermented
│ • H2S: Negative
│ • Urease: Negative
│ • Motility: Non-motile
│
SEROLOGY MOLECULAR
│ │
├─ Widal-type slide └─ Multiplex PCR / NAATs
│ agglutination with (GOLD STANDARD - enteric
│ Shigella antisera multiplex panels)
│ (confirm O-antigen Detects virulence genes
│ group A/B/C/D) (ipaH, Shiga toxin genes)
│
└─ Not routinely done
(culture preferred)
Culture Characteristics on MacConkey Agar:
| Organism | MacConkey Agar |
|---|---|
| E. coli | Pink (lactose fermenter) |
| Shigella | Pale/Colorless (non-lactose fermenter) |
| Salmonella | Pale (non-lactose fermenter) |
| Klebsiella | Pink, mucoid |
Additional Identification Steps:
- Serotyping: Slide agglutination with polyvalent antisera (Groups A, B, C, D)
- Group A = S. dysenteriae (12 serotypes)
- Group B = S. flexneri (6 serotypes)
- Group C = S. boydii (18 serotypes)
- Group D = S. sonnei (1 serotype)
-
Antibiotic Sensitivity Testing: Required due to multidrug resistance; fluoroquinolones or azithromycin are standard empirical therapy
-
NAATs / Multiplex PCR: Now considered the gold standard for diagnosis - detects ipaH gene (invasion plasmid) and Shiga toxin genes
Sources: Medical Microbiology 9e (Murray/Rosenthal); Red Book 2021; Rosen's Emergency Medicine
Quick Summary Table:
| Feature | Q1: Kala-azar (L. donovani) | Q2: Shigellosis (Shigella spp.) |
|---|---|---|
| Organism | Leishmania donovani | Shigella flexneri/dysenteriae |
| Vector/Route | Female sandfly | Fecal-oral |
| Pathogenesis | Intracellular survival in macrophages (RES) | Colonic invasion + T3SS + apoptosis induction |
| Key toxin | - | Shiga toxin (AB5) - inhibits protein synthesis |
| Diagnosis gold standard | Bone marrow/splenic aspirate Giemsa stain; rK39 ICT | Stool culture on MacConkey/XLD; NAATs/PCR |
| Key lab finding | LD bodies (amastigotes) in macrophages | NLF colonies + PMNs in stool |
| Serious complication | PKDL, severe pancytopenia | HUS, Toxic megacolon |
| Treatment | Sodium stibogluconate / Miltefosine | Fluoroquinolones / Azithromycin |
Give answers little shorter and briefly
MICROBIOLOGY – Long Essay Answers (10 Marks Each)
Q1 – Visceral Leishmaniasis (Kala-azar)
a) Etiological Agent & Clinical Diagnosis
- Agent: Leishmania donovani
- Diagnosis: Visceral Leishmaniasis (Kala-azar)
- Vector: Female Phlebotomus sandfly
- Key finding: Amastigotes (LD bodies) inside macrophages on Giemsa stain — oval, 2–3 µm, with nucleus + rod-like kinetoplast ("dot and dash")
b) Life Cycle & Pathogenesis
Sandfly bites → injects PROMASTIGOTES into skin
↓
Phagocytosed by macrophages
↓
Transform into AMASTIGOTES (LD bodies) inside phagosome
↓
Resist lysosomal killing → multiply → macrophage bursts
↓
Spread via lymphatics/blood to RES organs
(Spleen, Liver, Bone Marrow, Lymph nodes)
↓
Massive splenomegaly + hepatomegaly
Bone marrow infiltration → Pancytopenia
Irregular fever, weight loss, anaemia
↓
Untreated → FATAL
↓ (post-treatment in India)
PKDL (Post Kala-azar Dermal Leishmaniasis)
Key pathogenic events:
- Inhibits phagolysosome fusion → survives intracellularly
- Depresses cell-mediated immunity (CMI)
- Polyclonal B-cell activation → hypergammaglobulinaemia
- Leishmanin skin test negative in active disease
c) Laboratory Diagnosis
| Method | Details |
|---|---|
| Bone Marrow Aspirate | Gold standard – Giemsa stain shows LD bodies in macrophages |
| Splenic Aspirate | Most sensitive (>95%) but risk of bleeding |
| NNN Culture | Promastigotes grow in 1–4 weeks |
| rK39 ICT strip | Rapid, field-level diagnosis |
| DAT / ELISA | Serological confirmation |
| PCR | Most sensitive; species identification |
| Formol-gel (Napier's) test | Positive – due to hyperglobulinaemia (non-specific) |
Blood counts: Anaemia + Leukopenia + Thrombocytopenia + High ESR + Low albumin
Q2 – Bacillary Dysentery (Shigellosis)
a) Etiological Agent
- Organism: Shigella spp. (most likely S. flexneri in developing countries)
- Gram-negative, non-motile rod; non-lactose fermenter; oxidase-negative
- Infective dose: as low as 10–100 organisms
- 4 species: S. dysenteriae (most severe), S. flexneri, S. boydii, S. sonnei
b) Pathogenesis & Complications
Ingestion of Shigella (fecal-oral route)
↓
Small intestine → ENTEROTOXIN → watery diarrhea (early)
↓
Reach COLON → invade M-cells via Type III Secretion System (T3SS)
↓
T3SS injects Ipa proteins (IpaA/B/C/D) → membrane ruffling
↓
Bacteria engulfed → LYSE phagosome → replicate in cytoplasm
↓
Actin polymerization → spread cell-to-cell
(protected from immune clearance)
↓
Induce APOPTOSIS in macrophages → IL-1β release
↓
PMN infiltration → mucosal destruction
↓
BLOODY DYSENTERY: blood + mucus + pus in stool + tenesmus
↓ (S. dysenteriae only)
SHIGA TOXIN (AB5): B subunits bind Gb3 receptor
A subunit cleaves 28S rRNA → blocks protein synthesis
↓
Intestinal damage ± Glomerular endothelial damage → HUS
Complications:
| Complication | Notes |
|---|---|
| HUS | S. dysenteriae; triad: haemolytic anaemia + thrombocytopenia + renal failure |
| Reactive arthritis | Reiter syndrome; HLA-B27 linked |
| Toxic megacolon | Severe disease |
| Ekiri syndrome | Encephalopathy in children |
| Septicaemia | Rare; malnourished children |
c) Laboratory Diagnosis
Fresh stool specimen collected
↓
┌─────────────────────┬──────────────────────────────┐
│ MICROSCOPY │ CULTURE │
│ │ │
│ Wet mount: │ MacConkey agar: │
│ • Abundant pus cells│ PALE/COLORLESS colonies │
│ • RBCs + mucus │ (non-lactose fermenter) │
│ • NO ova/cysts │ │
│ │ XLD / Hektoen agar: │
│ │ confirm non-H2S colonies │
│ │ │
│ │ Selenite F broth: enrichment │
└─────────────────────┴──────────────────────────────┘
↓
Biochemical ID:
Lactose (-), H2S (-), Urease (-), Non-motile
↓
SEROTYPING:
Slide agglutination with antisera
Group A = S. dysenteriae
Group B = S. flexneri
Group C = S. boydii
Group D = S. sonnei
↓
PCR / NAATs (ipaH gene, Shiga toxin genes)
→ Gold standard, most sensitive
Treatment: Fluoroquinolones / Azithromycin (guided by sensitivity)
At-a-Glance Comparison
| Feature | Kala-azar | Shigellosis |
|---|---|---|
| Agent | L. donovani | Shigella spp. |
| Route | Sandfly bite | Fecal-oral |
| Key finding | LD bodies in macrophages | NLF colonies + PMNs in stool |
| Gold standard Dx | Bone marrow aspirate + rK39 | Stool culture / PCR |
| Dangerous complication | Pancytopenia, PKDL | HUS, toxic megacolon |
| Treatment | Miltefosine / Sodium stibogluconate | Fluoroquinolone / Azithromycin |
This is a shared conversation. Sign in to Orris to start your own chat.