Biomechanics of hip
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer:
Biomechanics of the Hip Joint
1. Joint Architecture
The hip is a spheroidal (ball-and-socket) joint — one of the most stable in the body. Its deep-seated design provides intrinsic stability while allowing multiplanar motion. Key architectural features include:
- Sourcil: a condensation of subchondral bone beneath the superomedial acetabulum, where the joint reaction force (R) is maximal
- Gothic arch: remodeled trabecular bone supporting the acetabular roof, with the sourcil at its base
- Neck-shaft angle (normal ~125–135°): critically influences load distribution
— General Anatomy and Musculoskeletal System, THIEME Atlas
2. Axes of Motion & Degrees of Freedom
The hip has three principal axes of motion, all passing through the center of the femoral head (the rotational center), giving it three degrees of freedom:
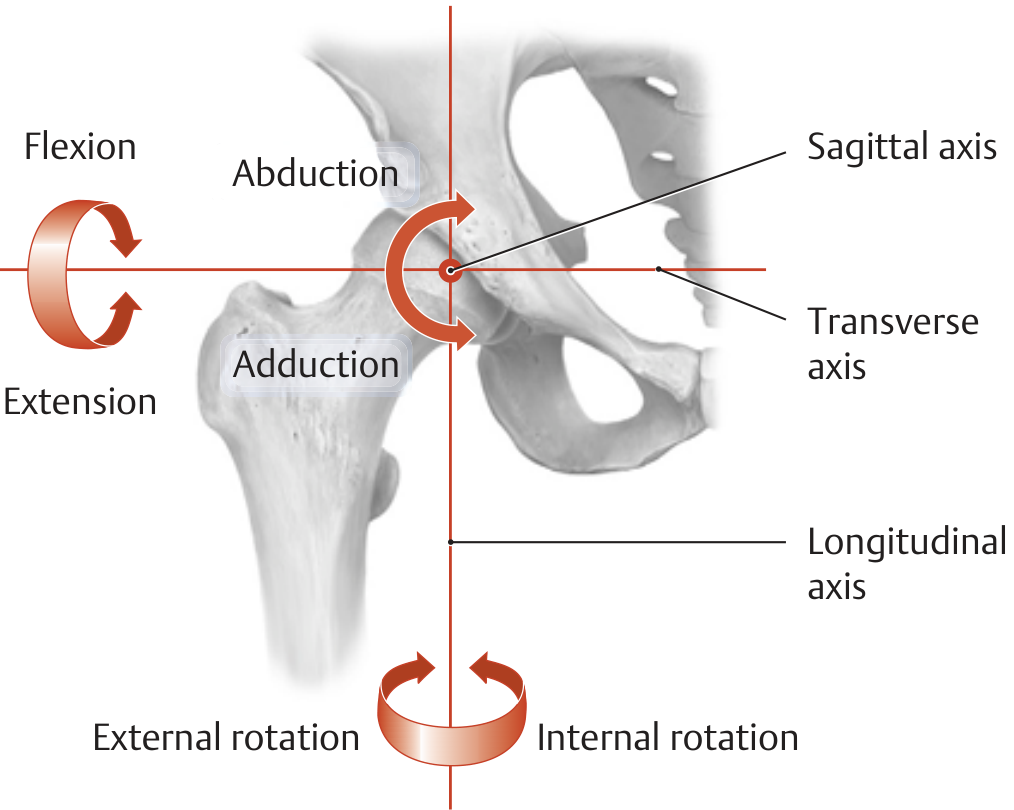
| Axis | Movement |
|---|---|
| Transverse axis | Flexion and extension |
| Sagittal axis | Abduction and adduction |
| Longitudinal axis | Internal and external rotation |
— THIEME Atlas of Anatomy, General Anatomy and Musculoskeletal System
3. Range of Motion
| Motion | Average Range | Functional Range |
|---|---|---|
| Flexion | 115° | 90° (120° to squat) |
| Extension | 30° | — |
| Abduction | 50° | 20° |
| Adduction | 30° | — |
| Internal rotation | 45° | 0° |
| External rotation | 45° | 20° |
Because the hip is a ball-and-socket joint, simultaneous triplanar motion makes instant center analysis essentially impossible.
— Miller's Review of Orthopaedics, 9th Ed.
4. Kinematics
- Hip flexion is greatest when the knee is flexed (hamstrings not limiting); ~140° active flexion from neutral is achievable
- Extension averages ~20° (measured by the Thomas maneuver, which eliminates compensatory lumbar lordosis and anterior pelvic tilt)
- Abduction averages 40–50° in the weight-bearing limb; adduction ~20–30° across the midline
- Rotation: internal 40°, external 50°, measured with the hip in both 0° and 90° of flexion (values differ due to capsular tension)
- Combined motions (e.g., flexion + abduction + external rotation = "FABER") involve circumduction
The hip exhibits rolling and gliding contact between the femoral head and acetabulum, with synovial fluid providing the primary lubrication. The coefficient of friction for human joints is approximately 0.002–0.04 — far superior to even the best synthetic arthroplasty bearings (metal-on-polyethylene: 0.05–0.15).
— THIEME Atlas; Miller's Review of Orthopaedics
5. Kinetics — Joint Reaction Force
The joint reaction force (R) at the hip during activities:
| Activity | Approx. Joint Reaction Force |
|---|---|
| Standing (bilateral) | ~1/3 body weight per hip |
| Single-leg stance / walking | 3–6× body weight |
| Stair climbing | Up to 7–8× body weight |
The high force is generated primarily by contraction of the muscles crossing the hip (especially the abductors) rather than body weight alone.
Using a cane in the contralateral hand significantly reduces R by offloading the abductor force requirement.
— Miller's Review of Orthopaedics, 9th Ed.
6. Neck-Shaft Angle and Its Effects
The normal neck-shaft angle is ~125–135°. Deviations have important biomechanical consequences:
| Neck-Shaft Angle | Effect |
|---|---|
| Coxa vara (varus, <120°) | ↓ joint reaction force R; ↑ shear across femoral neck; shortens limb; reduces abductor resting length → Trendelenburg gait |
| Coxa valga (valgus, >140°) | ↑ joint reaction force R; ↓ shear across neck; improves abductor moment arm |
For total hip arthroplasty (THA), neutral or valgus angulation is preferred. PMMA (bone cement) resists shear poorly, making varus positioning particularly problematic.
— Miller's Review of Orthopaedics, 9th Ed.
7. Muscle Biomechanics & Stability
- The iliopsoas and rectus femoris are primary hip flexors; tightness produces anterior pelvic tilt and compensatory lumbar hyperlordosis (demonstrated clinically by the Thomas test)
- The gluteus medius and minimus are primary abductors; their moment arm is the perpendicular distance from the femoral head center to the line of pull — critical for efficient single-leg stance
- The gluteus maximus is the primary extensor, most active on stair climbing and rising from a chair
- The piriformis and deep external rotators (obturators, gemelli, quadratus femoris) contribute to rotational stability
- The labrum deepens the acetabular socket, increases contact area, creates a fluid seal, and contributes to negative intra-articular pressure — all enhancing stability without sacrificing mobility
8. Hip Arthrodesis — Biomechanical Position
When arthrodesis is required, the optimal position is:
- 25–30° of flexion
- 0–5° of adduction
- 5–10° of external rotation
Fusion in abduction causes the patient to lurch over the fused limb with excessive trunk shift → low back pain. Fusion reduces gait efficiency to approximately 50% of normal and increases oxygen consumption.
— Miller's Review of Orthopaedics, 9th Ed.
9. Pelvic–Lumbar–Hip Coupling
The hip does not act in isolation. Restricted hip extension is compensated by:
- Anterior pelvic tilt
- Increased lumbar lordosis
This pelvis-lumbar coupling explains why hip flexor contracture is a common source of low back pain. Tight hip flexors place hip extensors (gluteus maximus, hamstrings) at a mechanical disadvantage, further perpetuating dysfunction.
— THIEME Atlas; Textbook of Family Medicine, 9th Ed.
Summary: The hip is a highly congruent, intrinsically stable ball-and-socket joint capable of 3° of freedom. Joint reaction forces routinely reach 3–6× body weight during gait, driven mainly by abductor muscle activity. Neck-shaft angle, abductor moment arm, and pelvic alignment are the key determinants of hip biomechanical efficiency. Clinical tools like the Thomas test and cane use translate directly from these principles.
This is a shared conversation. Sign in to Orris to start your own chat.