Now I have comprehensive data from ENT authoritative textbooks. Let me compile the full detailed answer.
Clinical Anatomy & Physiology of the Pharynx — Acute Pharyngeal Disease — Peritonsillar Abscess
I. CLINICAL ANATOMY OF THE PHARYNX
Definition and Overview
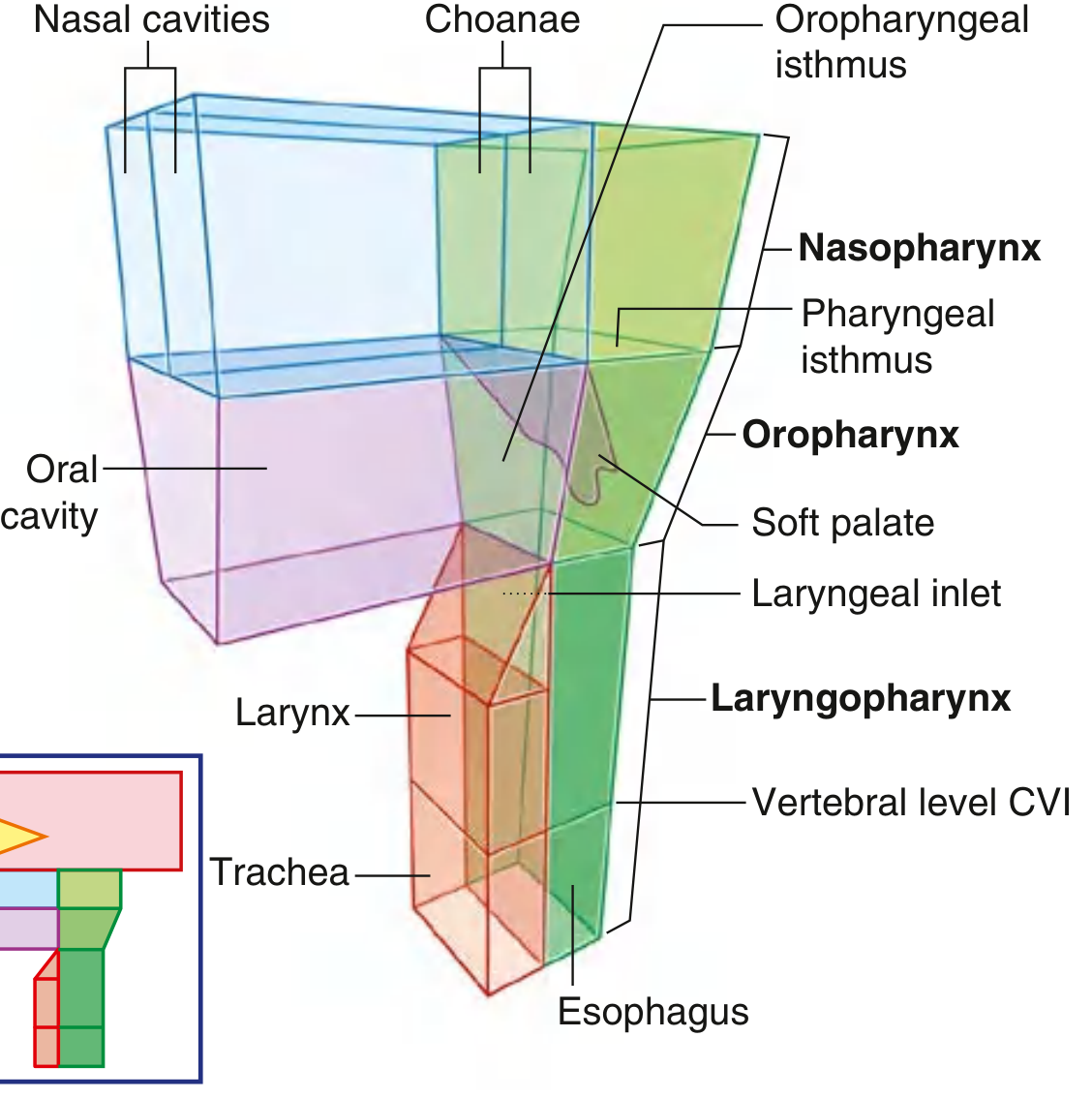
The pharynx is a musculofascial half-cylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck. Its cavity serves as a common pathway for air and food. It is attached superiorly to the base of the skull and is continuous inferiorly at approximately the level of vertebra C6 with the top of the esophagus.
Fig. Pharynx — showing relationships of nasal and oral cavities, pharynx, larynx, and trachea. (Gray's Anatomy for Students)
Subdivisions of the Pharynx
The pharynx is divided into three regions based on anterior relationships:
| Region | Anterior Opening | Level |
|---|
| Nasopharynx | Posterior choanae of nasal cavities | Skull base → soft palate |
| Oropharynx | Oropharyngeal isthmus (posterior oral cavity opening) | Soft palate → hyoid |
| Laryngopharynx (Hypopharynx) | Laryngeal inlet (superior aperture of larynx) | Hyoid → C6/esophagus |
Additional relationships:
- The pharyngotympanic (Eustachian) tubes open into the lateral walls of the nasopharynx
- The pharynx is separated from the vertebral column by the thin retropharyngeal space containing loose connective tissue
- The soft palate acts as a "flutter valve": elevates to seal the nasopharynx from oropharynx; depresses to seal the oral cavity from the oropharynx
— Gray's Anatomy for Students, p. 1180
Skeletal Framework
The superior and anterior margins of the pharyngeal wall attach to bone and cartilage. The two walls are united posteriorly in the midline by the pharyngeal raphe — a cord-like ligament descending from the pharyngeal tubercle on the base of the skull to C6, where it blends with the esophageal wall.
The line of skull attachment is C-shaped, beginning at the posterior margin of the medial pterygoid plate, crossing inferior to the pharyngotympanic tube, running onto the petrous temporal bone, and meeting at the midline pharyngeal tubercle.
Anterior Vertical Line of Attachment (Three Parts):
- First part: Medial pterygoid plate → pterygoid hamulus → pterygomandibular raphe → mandible
- Second part: Stylohyoid ligament → lesser horn of hyoid → body of hyoid → greater horn of hyoid
- Third part: Posterior aspect of thyroid cartilage and cricoid cartilage
— Gray's Anatomy for Students, p. 1181
Muscles of the Pharynx
Constrictors (outer circular layer):
- Superior constrictor — attaches to pterygomandibular raphe; overlaps the middle constrictor; most relevant clinically — the peritonsillar space lies between the tonsil capsule and this muscle
- Middle constrictor — from hyoid bone; fans out posteriorly
- Inferior constrictor — from thyroid and cricoid cartilages; its lowest fibers (cricopharyngeus) form the upper esophageal sphincter
Elevators (inner longitudinal layer):
- Stylopharyngeus — CN IX (glossopharyngeal)
- Salpingopharyngeus
- Palatopharyngeus
The constrictor muscles overlap like stacked cups — superior overlapped by middle, middle overlapped by inferior.
Nasopharynx
The roof and posterior wall form a continuous surface attached to the base of the skull and the anterior arch of C1–C2. Key structures:
- Pharyngeal tonsil (adenoids) — lymphoid tissue on the roof/posterior wall
- Torus tubarius — cartilaginous elevation marking the Eustachian tube opening
- Fossa of Rosenmüller — lateral recess posterior to the torus; most common site of nasopharyngeal carcinoma
- Salpingopharyngeal fold — runs inferiorly from torus
- Pharyngeal isthmus — junction with oropharynx, closed by soft palate elevation
Oropharynx
Extends from the soft palate to the upper border of the epiglottis. Contains:
- Palatine tonsils — large ovoid lymphoid masses on each lateral wall, between the palatoglossal arch (anterior pillar) and the palatopharyngeal arch (posterior pillar)
- Posterior one-third of the tongue (base of tongue / lingual tonsils)
- Valleculae — recesses between the base of tongue and epiglottis
Laryngopharynx (Hypopharynx)
Extends from the epiglottis to C6/cricoid cartilage. Contains:
- Piriform fossae — paired lateral recesses that channel food around the laryngeal inlet into the esophagus; common site of foreign body impaction and carcinoma
- Postcricoid region — posterior to the larynx; connects to the esophagus
- Cricopharyngeus muscle — the "upper esophageal sphincter" at C6
Waldeyer's Tonsillar Ring
A ring of lymphoid tissue surrounding the pharyngeal inlet:
- Pharyngeal tonsil (adenoid) — roof of nasopharynx (midline)
- Tubal tonsils — near Eustachian tube opening
- Palatine tonsils — lateral oropharynx (the clinically most prominent)
- Lingual tonsils — posterior tongue
— Gray's Anatomy for Students, p. 1188
Blood Supply
Arterial:
- Upper pharynx: ascending pharyngeal artery, ascending palatine and tonsillar branches of the facial artery, branches of maxillary and lingual arteries (all from external carotid)
- Lower pharynx: pharyngeal branches of inferior thyroid artery (from thyrocervical trunk)
Venous:
- Pharyngeal venous plexus → internal jugular vein
Nerve Supply
- Motor (all constrictors + most elevators): pharyngeal branch of vagus (CN X) via pharyngeal plexus
- Sensory: CN IX (glossopharyngeal) for oropharynx; CN X for laryngopharynx; CN V2 for nasopharynx
- Stylopharyngeus: CN IX alone
Lymphatic Drainage
- Nasopharynx and posterior pharynx → retropharyngeal nodes → deep cervical chain
- Tonsils and oropharynx → jugulodigastric (tonsillar) node — the sentinel node for tonsillar infection/malignancy
II. PHYSIOLOGY OF THE PHARYNX
Functions
- Respiratory conduit — transmits air between nasal/oral cavities and larynx
- Alimentary conduit — directs food/liquid from oral cavity to esophagus
- Phonation — acts as a resonating chamber
- Eustachian tube equalization — nasopharynx communicates pressure to middle ear
- Immune defense — Waldeyer's ring provides first-line mucosal immune surveillance
Swallowing (Deglutition)
Swallowing occurs in three phases:
1. Oral phase (voluntary): food bolus formed, tongue propels it posteriorly into oropharynx
2. Pharyngeal phase (involuntary, CN IX/X/XII coordinated):
- Soft palate elevates → closes pharyngeal isthmus → prevents nasal regurgitation
- Hyoid bone and larynx elevate anterosuperiorly
- Laryngeal inlet closes (epiglottis folds, arytenoids approximate, true cords adduct) → airway protected
- Pharyngeal constrictors contract in peristaltic wave superiorly → inferiorly
- Upper esophageal sphincter (cricopharyngeus) relaxes
A person cannot breathe and swallow simultaneously because the airway is closed at two sites: the pharyngeal isthmus and the larynx. — Gray's Anatomy for Students, p. 1188
3. Esophageal phase: bolus enters esophagus; peristalsis continues to stomach
III. PHARYNGEAL SPACES
The pharynx is surrounded by fascial spaces that are clinically critical because infection can spread rapidly through them. Understanding their boundaries guides surgical drainage.
Fascial Layers of the Neck
Superficial layer (investing fascia): envelopes SCM, trapezius, submandibular gland, parotid
Deep cervical fascia:
- Middle layer (visceral/pretracheal): envelopes pharynx, larynx, trachea, esophagus, thyroid
- Deep layer: two sublayers:
- Alar layer: base of skull → mediastinum; covers sympathetic trunk
- Prevertebral layer: base of skull → coccyx; covers vertebral bodies, paraspinous muscles
- ⚠️ Danger space = space between alar and prevertebral layers → extends from base of skull to mediastinum → rapid infection spread
Key Pharyngeal Spaces
1. Peritonsillar Space
- Medial: palatine tonsil (capsule)
- Lateral: superior constrictor muscle
- Contents: loose areolar tissue, tonsillar branches of lingual/facial/ascending pharyngeal vessels
- Clinical significance: site of peritonsillar abscess — the most common deep space infection of the head and neck
2. Parapharyngeal Space (Lateral Pharyngeal Space)
- Superior: base of skull (middle cranial fossa)
- Inferior: hyoid bone
- Anterior: pterygomandibular raphe
- Posterior: prevertebral fascia
- Medial: pharyngobasilar fascia / superior constrictor
- Lateral: deep lobe of parotid, mandible, medial pterygoid
- Divided by styloid process into:
- Prestyloid (muscular) compartment: fat, lymph nodes, internal maxillary artery, inferior alveolar/lingual/auriculotemporal nerves, pterygoid muscles, deep parotid lobe
- Poststyloid (neurovascular) compartment: internal carotid artery, internal jugular vein, CN IX, X, XI, XII, cervical sympathetic chain
- Clinical significance: Peritonsillar abscess can rupture through superior constrictor into this space; spread here causes Horner syndrome (sympathetic chain), cranial nerve palsies
3. Retropharyngeal Space (Retrovisceral Space)
- Superior: base of skull
- Inferior: posterior mediastinum (T1–T2)
- Anterior: posterior pharyngeal wall (constrictor muscles)
- Posterior: alar layer of deep cervical fascia
- Contents: retropharyngeal lymph nodes (most prominent in children < 5 years), loose areolar tissue
- Clinical significance: retropharyngeal abscess — most common in children; on lateral neck X-ray: >5 mm prevertebral soft tissue at C2 (child) or >7 mm (adult); can spread to mediastinum
4. Danger Space
- Between alar and prevertebral layers of deep cervical fascia
- Extends from skull base to diaphragm (T12)
- Has no natural barriers → direct conduit for mediastinitis
5. Prevertebral Space
- Behind prevertebral fascia
- Contains paraspinous and scalene muscles, vertebral bodies, phrenic nerve, brachial plexus
- Extends to coccyx
6. Submandibular (Submaxillary) Space
- Bounded by floor of mouth mucosa (superior), digastric muscle (inferior), skin/platysma/mandible (lateral)
- Divided by mylohyoid into sublingual (supramylohyoid) and submaxillary (inframylohyoid) compartments
- Ludwig's angina = bilateral cellulitis of this space; floor-of-mouth edema, tongue swelling, airway emergency
7. Visceral (Pretracheal) Space
- Superior: hyoid bone
- Inferior: T4 (arch of aorta)
- Contains: pharynx, esophagus, larynx, trachea, thyroid
8. Carotid Sheath Space
- Envelopes carotid artery, internal jugular vein, vagus nerve
- Called "The Lincoln Highway of the Neck" — a potential avenue for rapid spread of infection from skull base to thorax
— K.J. Lee's Essential Otolaryngology, pp. 699–704
IV. ACUTE DISEASES OF THE PHARYNX
A. Acute Pharyngitis — Primary Angina
Definition: Acute inflammation of the pharyngeal mucosa and submucosal tissues, most commonly infectious. "Primary angina" refers to pharyngitis/tonsillitis where the pharynx itself is the primary site of infection (not secondary to systemic disease).
Viral Causes (Most Common Overall)
| Virus | Clinical Feature |
|---|
| Rhinovirus | Most common cause of common cold |
| Coronavirus | Common cold |
| Parainfluenza | Common cold, croup |
| Influenza A & B | Widespread outbreaks, systemic illness |
| Adenovirus | Pharyngoconjunctival fever (pharyngitis + conjunctivitis) |
| Coxsackie A | Herpangina (vesicular eruption on soft palate/anterior pillar + fever); hand-foot-mouth disease |
| Epstein-Barr virus (EBV) | Infectious mononucleosis — exudative tonsillitis + lymphadenopathy + splenomegaly + atypical lymphocytosis |
| Cytomegalovirus (CMV) | CMV mononucleosis |
| HSV types 1 & 2 | Pharyngitis, gingivostomatitis |
| HIV | Acute retroviral syndrome (primary HIV infection) — consider in sexually active patients |
Bacterial Causes
| Organism | Clinical Syndrome |
|---|
| Group A β-hemolytic Streptococcus (GABHS) S. pyogenes | Most important bacterial cause; pharyngitis, tonsillitis, scarlet fever |
| Non-group A β-hemolytic Streptococcus (B, C, G) | Pharyngitis, tonsillitis |
| Neisseria gonorrhoeae | STI-related pharyngitis |
| Corynebacterium diphtheriae | Diphtheria — gray pseudomembrane, bull-neck, myocarditis, neuropathy |
| Arcanobacterium haemolyticum | Pharyngitis + scarlatiniform rash in adolescents |
| Mixed anaerobes + spirochetes | Vincent's angina (acute necrotizing ulcerative pharyngitis) — fusospirochetal infection |
| Francisella tularensis | Ulceroglandular tularemia |
— K.J. Lee's Essential Otolaryngology, pp. 684–686
GABHS Pharyngitis — Clinical Features and Diagnosis
Centor Criteria (used to estimate probability of GABHS):
- Tonsillar exudate
- Tender anterior cervical lymphadenopathy
- Fever (>38°C / 100.4°F)
- Absence of cough
Score 3–4: empiric treatment OR confirm with rapid strep test/culture
Score 0–1: viral etiology likely; no antibiotic needed
Complications of untreated GABHS:
- Non-suppurative: Acute rheumatic fever (ARF), post-streptococcal glomerulonephritis, PANDAS
- Suppurative: peritonsillar abscess, parapharyngeal abscess, otitis media, sinusitis, mastoiditis
Treatment: Penicillin V (first-line) × 10 days; amoxicillin; clindamycin or macrolide if penicillin-allergic
B. Secondary Angina (Pharyngitis as Manifestation of Systemic Disease)
"Secondary angina" refers to pharyngeal inflammation that is a manifestation of an underlying systemic process rather than a primary pharyngeal infection:
| Condition | Pharyngeal Findings |
|---|
| Infectious mononucleosis (EBV) | Severe exudative tonsillitis, palatal petechiae, uvular edema, posterior cervical adenopathy, hepatosplenomegaly |
| Agranulocytosis | Necrotizing tonsillopharyngitis in context of absent neutrophils (drug-induced, leukemia) |
| Leukemia / lymphoma | Tonsillar enlargement, ulceration, without purulent exudate |
| Diphtheria | Grayish pseudomembrane (bleeds on removal), bull-neck adenopathy; toxin → cardiac/neurologic complications |
| Syphilis | Secondary syphilis → mucous patches, painless pharyngeal lesions |
| Scarlet fever | GABHS toxin → strawberry tongue, sandpaper rash, pharyngitis |
| HIV acute retroviral syndrome | Mononucleosis-like pharyngitis, rash, generalized lymphadenopathy |
| GERD/LPR | Chronic posterior pharyngitis, cobblestoning |
C. Acute Tonsillitis
Acute inflammation of the palatine tonsils specifically.
Pathogens: GABHS (most important), adenovirus, EBV; other β-hemolytic streptococci
Clinical features:
- Severe sore throat, odynophagia, dysphagia, fever
- Tonsillar enlargement, erythema, white/yellow exudate (follicular or membranous)
- Jugulodigastric lymphadenopathy (tender "tonsillar node")
- Halitosis, trismus if extending
Grading of tonsillar hypertrophy (Friedman / Mallampati):
- Grade 1: tonsils within tonsillar fossa
- Grade 2: tonsils extending to pillars
- Grade 3: tonsils beyond pillars
- Grade 4: tonsils touching ("kissing tonsils")
Indications for tonsillectomy (Paradise criteria):
- ≥7 episodes in 1 year, OR
- ≥5 episodes/year for 2 consecutive years, OR
- ≥3 episodes/year for 3 consecutive years
-
2 weeks school/work missed in 1 year
- Upper airway obstruction / sleep-disordered breathing
- Peritonsillar abscess
- Suspicion of malignancy (unilateral tonsillar enlargement)
- Recurrent febrile seizures from tonsillitis
- Diphtheria carrier
— K.J. Lee's Essential Otolaryngology, p. 611–613
V. PERITONSILLAR ABSCESS
Definition
A peritonsillar abscess (PTA) — quinsy — is an accumulation of pus in the peritonsillar space: deep to the tonsil capsule, between the palatine tonsil and the superior constrictor muscle. It is the most common deep space infection of the head and neck.
Pathogenesis
PTA develops as a complication of:
- Acute tonsillitis — spreading infection through the tonsil capsule
- Weber's glands (minor salivary glands in the superior peritonsillar space) — possibly a primary focus of infection
- Infection follows: tonsillitis → peritonsillar cellulitis → peritonsillar abscess
Microbiology: Typically polymicrobial:
- Aerobic: Streptococcus pyogenes (GABHS), Staphylococcus aureus (including MRSA)
- Anaerobic: Bacteroides spp., Fusobacterium spp.
The most common aerobic organisms are Streptococcus pyogenes (GABHS) and Staphylococcus aureus. The most common anaerobes are Bacteroides and Fusobacterium. — Pfenninger & Fowler's Procedures for Primary Care
Location: Most commonly superior pole of the tonsil (where Weber's glands are concentrated); occasionally middle or inferior pole.
Clinical Presentation
| Symptom/Sign | Mechanism |
|---|
| Severe unilateral sore throat | Peritonsillar space inflammation |
| Trismus (difficulty opening mouth) | Spasm of medial pterygoid muscle due to adjacent inflammation |
| Hot potato voice (muffled, "plummy") | Alteration of pharyngeal resonance by peritonsillar swelling |
| Dysphagia/odynophagia | Oropharyngeal swelling |
| Drooling (pooling of saliva) | Inability to swallow |
| Uvular deviation to contralateral side | Peritonsillar pus displaces soft palate and uvula across midline |
| Tonsil displaced medially and inferiorly | Pus in superior peritonsillar space pushes tonsil |
| Bulging of soft palate | Inferior extension of pus under soft palate |
| Fever, chills, malaise | Systemic infectious response |
| Neck stiffness / ipsilateral neck pain | Adjacent parapharyngeal involvement |
| Foetor oris | Anaerobic bacteria |
Key distinguishing sign: unilateral peritonsillar bulge with uvular deviation away from the affected side (contrast with parapharyngeal abscess, where the tonsil is displaced medially but the soft palate may be less affected).
Imaging
- CT neck with IV contrast: Gold standard for confirming abscess vs. cellulite (phlegmon), delineating extent, ruling out parapharyngeal extension
- CT can identify which neck spaces require drainage, though still misidentifies abscess vs. phlegmon in ~25% of explorations
- Intraoral ultrasound: Growing evidence for real-time guidance during aspiration
- Plain lateral neck X-ray: Limited for PTA specifically (more useful for retropharyngeal abscess)
Management
1. Drainage (Primary Treatment)
Three approaches:
a. Needle aspiration: First-line in adults and cooperative adolescents
- Insert 18-gauge needle at the point of maximal fluctuance (usually superior pole)
- Aspirate pus; send for culture
- Can repeat if re-accumulates
b. Incision and drainage (I&D): More thorough
- Local anesthesia; incision at superior pole through mucosa and capsule
- Blunt dissection with hemostat into abscess cavity
- CPT code: 42700
c. Quinsy tonsillectomy (tonsillectomy in the acute setting):
- Indications: recurrent PTA, patient already under general anesthesia, massive swelling limiting visualization, poor cooperation
- Disadvantage: higher hemorrhage risk in acute infection
Peritonsillar abscess (PTA) may spontaneously drain, progress to involve the deep neck space or sepsis, or even lead to airway obstruction. The most important part of treatment is drainage. — Textbook of Family Medicine, 9e
2. Antibiotics
- Empiric coverage for GABHS and oral anaerobes
- Penicillin G IV or Amoxicillin-clavulanate
- Clindamycin (good anaerobic coverage, especially if MRSA concern)
- Metronidazole can be added for anaerobic coverage
3. Supportive
- IV fluids (often dehydrated from odynophagia)
- Corticosteroids (dexamethasone) — reduce edema, symptom duration
- Analgesics
- Airway monitoring — if significant trismus and swelling, awake fiberoptic intubation or tracheostomy may be required
Complications
| Complication | Mechanism |
|---|
| Parapharyngeal abscess | Rupture of PTA through superior constrictor into lateral pharyngeal space |
| Airway obstruction | Massive edema or downward extension |
| Dehydration | Severe odynophagia preventing oral intake |
| Internal carotid artery erosion / pseudoaneurysm | Parapharyngeal extension → vascular involvement |
| Internal jugular vein thrombophlebitis (Lemierre's syndrome) | Bacteremia → septic thrombophlebitis of IJV; Fusobacterium necrophorum classically |
| Mediastinitis / descending necrotizing mediastinitis | Spread via danger space — life-threatening |
| Brain abscess | Hematogenous spread or direct extension |
| Aspiration pneumonia | Abscess rupture with aspiration |
| Post-streptococcal nephritis | Streptococcal antigen deposition |
| Endocarditis | Bacteremia |
| Sepsis | Systemic infection |
Complications include: dehydration, airway obstruction, parapharyngeal abscess (due to rupture through superior constrictor), venous involvement (thrombosis, phlebitis, bacteremia, endocarditis), arterial involvement (thrombosis, hemorrhage, pseudoaneurysms), mediastinitis, brain abscess, aspiration pneumonia. — K.J. Lee's Essential Otolaryngology
Differential Diagnosis of PTA
| Condition | Key Differentiating Feature |
|---|
| Peritonsillar cellulitis | No fluctuance; less trismus; no abscess on imaging |
| Parapharyngeal abscess | Tonsil displaced medially but no peritonsillar bulge; neck swelling; CN palsy |
| Retropharyngeal abscess | Posterior pharyngeal wall bulge; stiff neck; dysphagia; fever in child |
| Epiglottitis | Dysphagia, drooling, inspiratory stridor; "thumbprint sign" on lateral X-ray |
| Tonsillar malignancy | No fever, firm, non-fluctuant unilateral tonsillar mass; no response to antibiotics |
| Infectious mononucleosis | Bilateral tonsils, posterior cervical adenopathy, splenomegaly; Monospot positive |
VI. SUMMARY TABLE — DEEP PHARYNGEAL SPACE INFECTIONS
| Space | Common Source | Clinical Clues | Drainage Route |
|---|
| Peritonsillar | Tonsillitis | Uvular deviation, hot potato voice, trismus | Transoral needle/I&D |
| Parapharyngeal | PTA rupture, dental, parotid | Lateral neck swelling, trismus, CN palsies | Transoral or transcervical |
| Retropharyngeal | URI, adenitis (children) | Posterior pharyngeal bulge, stiff neck, dysphagia | Transoral or transcervical |
| Submandibular | Dental (2nd/3rd molar) | Floor of mouth induration, Ludwig's angina | Transcervical |
| Danger space | Extension from above | Mediastinitis, rapid deterioration | Mediastinal drainage |
Sources
- K.J. Lee's Essential Otolaryngology, 12th ed. — Chapters 36–37 (pharyngeal spaces, infections, PTA)
- Cummings Otolaryngology Head and Neck Surgery — Chapters 96, 100 (pharyngeal anatomy, radiology)
- Gray's Anatomy for Students — Chapter 8 (pharynx, p. 1180–1188)
- Pfenninger & Fowler's Procedures for Primary Care — Peritonsillar abscess drainage
- Textbook of Family Medicine, 9e — Peritonsillar abscess management