Acute pancreatitis for 10 mark’s question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to write a comprehensive 10-mark answer. Here it is:
Acute Pancreatitis — 10-Mark Answer
Definition
Acute pancreatitis (AP) is a sudden inflammatory disease of the pancreas characterized by autodigestion of the gland by its own enzymes. Diagnosis requires at least two of the following three criteria:
- Abdominal pain consistent with the disease
- Serum amylase or lipase >3× the upper limit of normal
- Characteristic findings on abdominal imaging
— Textbook of Family Medicine 9e
Etiology (Causes) — "GET SMASHED"
| Category | Notes |
|---|---|
| Gallstones | Most common cause (>50% of cases); biliary sludge and microlithiasis included |
| Ethanol (Alcohol) | Second most common (~30%); may be a toxin or exacerbating factor |
| Hypertriglyceridemia | When triglycerides >1000 mg/dL with no gallstones/alcohol |
| Trauma | Blunt abdominal trauma; pancreas protected retroperitoneally |
| ERCP | Post-procedure pancreatitis; significant cause |
| Medications | Valproate, L-asparaginase, prednisone, 6-mercaptopurine, azathioprine, thiazides |
| Infections | Mumps, Coxsackievirus, EBV, Mycoplasma, ascariasis |
| Neoplasm | Consider in anyone >40 years with unexplained AP |
| Idiopathic | ~15% of cases |
| Metabolic | Hypercalcemia, renal failure |
| Structural | Pancreas divisum, bile/pancreatic duct anomalies |
Pathophysiology
The key initiating event is premature intracellular activation of pancreatic enzymes (especially trypsinogen → trypsin) within acinar cells, rather than in the duodenum. Activated trypsin triggers a cascade:
- Autodigestion of pancreatic parenchyma and peripancreatic fat
- Release of pro-inflammatory cytokines (IL-1, IL-6, TNF-α) → systemic inflammatory response
- In severe cases: parenchymal necrosis, fat necrosis, hemorrhage, and multisystem organ failure
Clinical Features
Symptoms:
- Severe, sudden-onset epigastric pain radiating to the back ("boring" pain)
- Pain worsens in supine position; relieved by leaning forward
- Nausea, vomiting, anorexia
- Fever
Signs:
- Epigastric tenderness, guarding, rigidity
- Cullen's sign — periumbilical ecchymosis (haemorrhagic pancreatitis)
- Grey-Turner's sign — flank ecchymosis
- Paralytic ileus, abdominal distension
- Jaundice (if biliary obstruction)
Investigations
Serum Enzymes
- Serum lipase — preferred marker; rises and falls more slowly than amylase; more specific
- Serum amylase — rises within 6–12 hours, returns to normal in 3–5 days; can be elevated in other conditions (e.g., salivary gland disease, perforated PUD)
- >3× ULN of either confirms diagnosis
Imaging
- Ultrasound abdomen — first-line; detects gallstones, biliary dilation, peripancreatic fluid
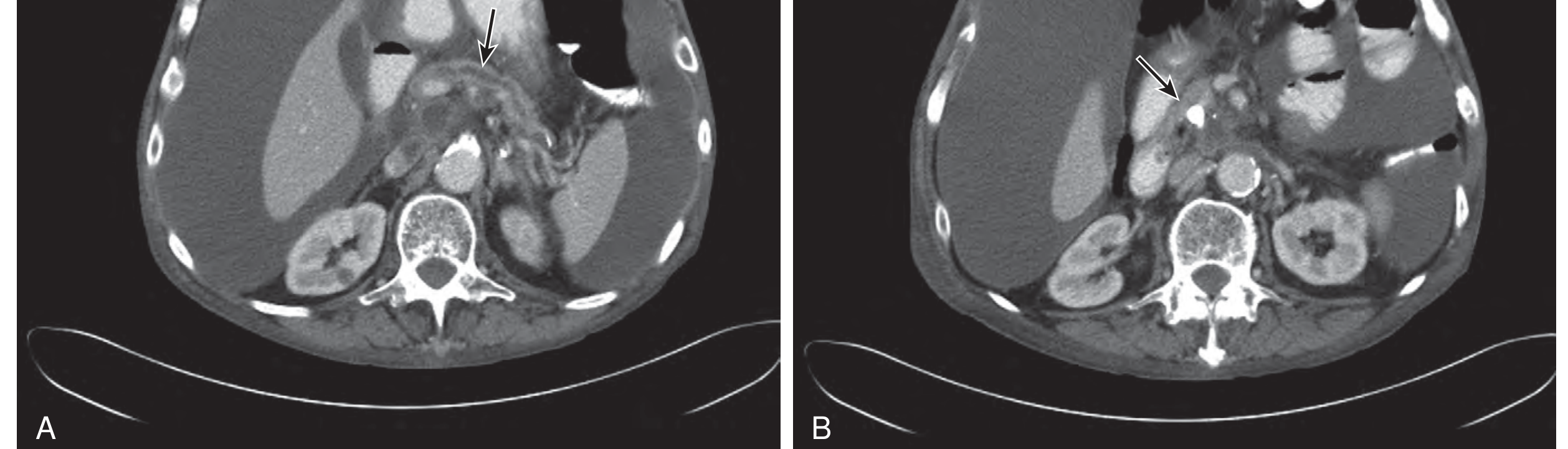
- CT abdomen with contrast — gold standard for severity assessment; detects necrosis, abscesses, pseudocysts
Other Tests
- LFTs (ALT >3× ULN suggests gallstone etiology)
- Serum triglycerides, calcium
- CBC, CRP, BUN, creatinine
- Blood glucose
- Chest X-ray (pleural effusion, ARDS)
- MRCP — for bile duct anatomy without radiation
Severity Assessment
Ranson's Criteria
At Admission (0 hours):
| Parameter | Threshold |
|---|---|
| Age | >55 years |
| WBC | >16,000/mm³ |
| Blood glucose | >200 mg/dL |
| LDH | >350 IU/L |
| AST | >250 IU/L |
At 48 hours:
| Parameter | Threshold |
|---|---|
| Hematocrit fall | >10% |
| BUN rise | >5 mg/dL |
| Serum calcium | <8 mg/dL |
| PaO₂ | <60 mmHg |
| Base deficit | >4 mEq/L |
| Fluid sequestration | >6 L |
Scoring: 0–2 = mild; 3–4 = moderate; ≥5 = severe (mortality rises sharply)
BISAP Score (Bedside Index of Severity in AP)
- BUN >25 mg/dL
- Impaired mental status (Glasgow Coma Scale <15)
- SIRS (≥2 SIRS criteria)
- Age >60 years
- Pleural effusion
Score ≥3 = increased risk of mortality.
Atlanta Classification (Revised 2012)
- Mild AP — no organ failure, no local/systemic complications; resolves in 1 week
- Moderately Severe AP — transient organ failure (<48 h) or local complications
- Severe AP — persistent organ failure (>48 h), single or multi-organ
Complications
Local Complications
- Acute peripancreatic fluid collection (early, <4 weeks)
- Pancreatic pseudocyst (>4 weeks, non-epithelialized fluid collection)
- Acute necrotic collection (contains necrotic material, <4 weeks)
- Walled-off necrosis (WON) (organized necrosis, >4 weeks)
- Pancreatic abscess
- Pseudoaneurysm, splenic vein thrombosis
Systemic Complications
- ARDS (acute respiratory distress syndrome)
- Acute kidney injury
- Shock
- DIC (disseminated intravascular coagulation)
- Hypocalcemia (saponification of fat)
- Hyperglycemia
- GI bleeding
Management
General Principles (first 48–72 hours are critical)
-
IV Fluid Resuscitation — Most critical early intervention
- Aggressive isotonic fluid replacement (Ringer's lactate preferred over normal saline — reduces SIRS)
- Target urine output >0.5 mL/kg/hr
- Monitor for fluid overload
-
Analgesia
- IV opioids (morphine, hydromorphone, meperidine) — adequate pain control is essential
- NSAIDs/ketorolac for mild cases
-
NPO vs. Early Oral/Enteral Feeding
- Mild AP: resume clear liquids and advance diet when pain resolves and bowel sounds return
- Severe AP: early enteral nutrition via nasojejunal tube (preferred over TPN) — reduces bacterial translocation and infection
- TPN only if enteral route not tolerated
-
Antibiotics
- Not indicated prophylactically
- Used only when there is evidence of infected necrosis or sepsis
- Agents: imipenem, meropenem, or ciprofloxacin + metronidazole
-
Monitoring
- Frequent vitals, urine output, CBC, metabolic panel
- ICU admission for severe AP
Specific Interventions
- Gallstone pancreatitis: Early ERCP with sphincterotomy if cholangitis or persistent biliary obstruction; cholecystectomy during same admission for mild AP to prevent recurrence
- Hypertriglyceridemia: Plasmapheresis, insulin infusion (activates lipoprotein lipase)
- Infected necrosis: Endoscopic or surgical necrosectomy (step-up approach: drainage first, then necrosectomy)
Prognosis & Mortality
| Severity | Mortality |
|---|---|
| Mild (Ranson <3) | <1% |
| Moderate (Ranson 3–4) | 15–20% |
| Severe (Ranson ≥5) | 40–50%+ |
| With infected necrosis | Up to 80% historically |
Approximately 40% of acute cases are diagnosed only at autopsy, underlining the importance of early recognition.
Key Points Summary
- AP = autodigestion by premature enzyme activation
- Most common causes: gallstones > alcohol
- Diagnose with 2 of 3 criteria (pain + enzymes + imaging)
- Lipase is more sensitive and specific than amylase
- Severity: Ranson's, BISAP, Atlanta Classification
- Management: aggressive IV fluids, analgesia, early enteral feeding; antibiotics only for infected necrosis
- Gallstone AP → ERCP if obstruction → cholecystectomy before discharge
- Complications: pseudocyst, necrosis, ARDS, renal failure, hypocalcemia
Sources: Textbook of Family Medicine 9e; Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.