Acute pancreatitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me synthesize a complete clinical overview of acute pancreatitis.
Acute Pancreatitis
Definition & Epidemiology
Acute pancreatitis (AP) is a sudden inflammatory disease of the pancreas that ranges from mild, self-limited illness to a life-threatening emergency. Hospital admissions in the USA appear to be increasing. The clinical diagnosis requires two of three criteria:
- Abdominal pain strongly suggestive of AP
- Serum amylase and/or lipase ≥ 3× the upper limit of normal
- Characteristic imaging findings
— Grainger & Allison's Diagnostic Radiology
Etiology (Mnemonic: GET SMASHED)
| Category | Examples |
|---|---|
| Gallstones | Most common cause in adults (~40%) |
| Ethanol | Second most common (~30%) |
| Trauma | Blunt abdominal trauma |
| Steroids | Corticosteroids, azathioprine |
| Mumps / infections | EBV, CMV, Coxsackievirus, Mycoplasma |
| Autoimmune | IgG4-related disease |
| Scorpion venom / Spider bite | Rare |
| Hyperlipidaemia / Hypercalcaemia | Metabolic causes |
| ERCP | Post-procedural pancreatitis |
| Drugs | Valproate, L-asparaginase, 6-mercaptopurine, furosemide, tetracyclines |
Additional causes: pancreas divisum, genetic mutations (SPINK1, CFTR, PRSS1), malignancy, vasculitis (SLE, Kawasaki disease). ~5% remain idiopathic.
Pathogenesis
The final common pathway is premature intracellular activation of trypsinogen to trypsin within acinar cells, triggering auto-digestion. This releases inflammatory mediators (IL-1, IL-6, TNF-α), leading to a local inflammatory cascade that, in severe cases, progresses to systemic inflammatory response syndrome (SIRS) and multi-organ dysfunction.
Clinical Features
- Pain: Sudden-onset, severe, constant epigastric pain radiating to the back or left scapular region; patients are more comfortable leaning forward
- Nausea, vomiting, anorexia, fever
- Examination: Tachycardia, tachypnoea, epigastric tenderness, hypoactive bowel sounds, abdominal rigidity (variable)
- Rare signs of haemorrhagic pancreatitis:
- Grey-Turner sign: flank ecchymosis
- Cullen sign: periumbilical ecchymosis
- Extremities may be cool and cyanotic from underperfusion
— Sleisenger and Fordtran's GI and Liver Disease
Laboratory Findings
| Test | Findings |
|---|---|
| Serum amylase | Elevated within hours; non-specific (also elevated in other abdominal conditions) |
| Serum lipase | More sensitive and specific; stays elevated longer |
| WBC | 12,000–20,000/mm³ typical |
| CRP | Marker of severity (>150 mg/L at 48h suggests severe disease) |
| LFTs | Elevated ALT >3× normal suggests gallstone etiology |
| Serum calcium | Hypocalcaemia (saponification of fat) |
| Blood glucose | Hyperglycaemia (transient or persistent) |
| Triglycerides | Check if hypertriglyceridaemia is suspected cause |
| ABG | Hypoxaemia in severe cases |
Severity Classification — Revised Atlanta 2012
| Category | Definition |
|---|---|
| Mild | No organ failure; no local/systemic complications |
| Moderately severe | Transient organ failure (<48 h) or local complications without persistent organ failure |
| Severe | Persistent organ failure (>48 h), single or multi-organ |
Morphological types (Revised Atlanta):
- Interstitial oedematous pancreatitis — pancreatic parenchyma enhances normally on contrast CT; peripancreatic oedema present
- Necrotising pancreatitis — non-enhancing areas indicating parenchymal necrosis; may involve peripancreatic tissue
Severity Scoring Systems
Ranson Criteria (1974)
At admission (5 criteria): Age >55, WBC >16,000, glucose >200 mg/dL, LDH >350 IU/L, AST >250 IU/L
At 48 hours (6 criteria): Haematocrit fall >10%, BUN rise >5 mg/dL, Ca²⁺ <8 mg/dL, PaO₂ <60 mmHg, base deficit >4 mEq/L, fluid sequestration >6 L
Score ≥3 = severe disease.
BISAP Score
Each criterion = 1 point:
- BUN > 25 mg/dL
- Impaired mental status
- SIRS present
- Age > 60 years
- Pleural effusion
Score ≥3 correlates with increased mortality.
CT Severity Index (CTSI / Modified Balthazar)
A radiological scoring system (max 10 points):
| Parameter | Points |
|---|---|
| Normal pancreas | 0 |
| Intrinsic pancreatic abnormality ± peripancreatic fat changes | 2 |
| Pancreatic/peripancreatic fluid collection or fat necrosis | 4 |
| Necrosis ≤30% | +2 |
| Necrosis >30% | +4 |
| Extrapancreatic complications (pleural effusion, ascites, vascular/GI involvement) | +2 |
Mild: 0–2 | Moderate: 4–6 | Severe: 8–10
— Grainger & Allison's Diagnostic Radiology
Imaging
CT (Investigation of Choice for Severity)
Contrast-enhanced CT (CECT) is the gold standard for:
- Confirming diagnosis when uncertain
- Assessing extent of pancreatic necrosis
- Identifying fluid collections and complications
Important timing caveat: CT performed within 12–24 hours may underestimate the degree of necrosis, which takes 2–3 days to fully develop. CECT is best performed after 72 hours if clinical deterioration warrants it.
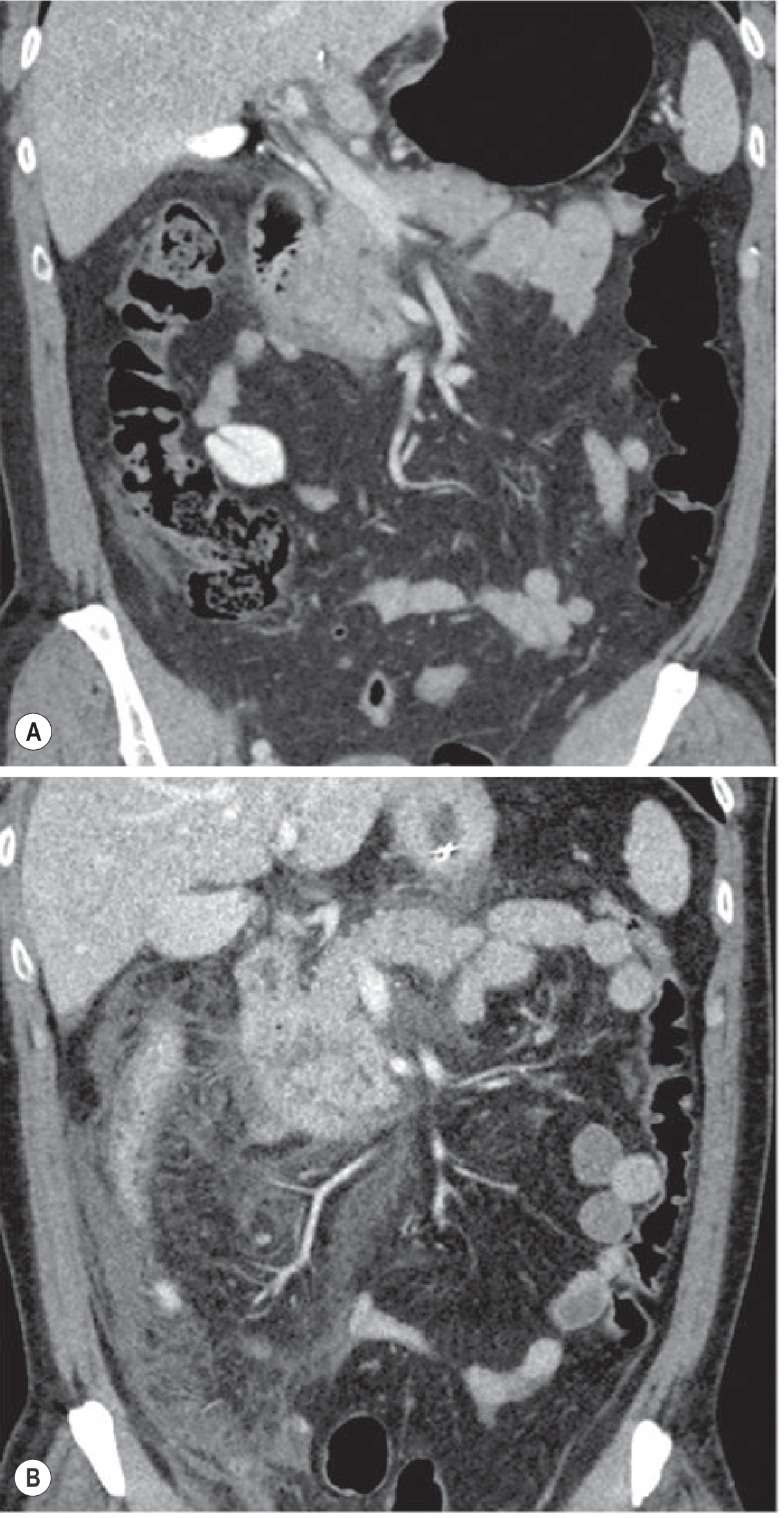
Fig. Appropriate timing of CT in acute pancreatitis: (A) CT at 12 hours shows only minimal signs; (B) follow-up CT on day 3 demonstrates much more severe inflammation. — Grainger & Allison's Diagnostic Radiology
A single venous-phase CT (70s delay; ~1.5–2 mL/kg contrast at 4 mL/s) is sufficient to stage AP. Arterial phase is not routinely needed.
If CECT is contraindicated (e.g. renal failure), contrast-enhanced ultrasound (CEUS) is an alternative to assess necrosis.
Ultrasound
- First-line initial investigation
- Limited pancreatic visualisation due to overlying bowel gas
- Excellent for identifying gallstones as the cause
- Useful for guiding drainage of fluid collections
MRI / MRCP
- Superior to CT for characterising fluid collections and ductal disruption
- MRCP useful to detect choledocholithiasis without ERCP risk
- Preferred in pregnancy and young patients requiring serial imaging
Fluid Collections (Revised Atlanta Terminology)
| Collection | Timing | Contents | Wall |
|---|---|---|---|
| Acute peripancreatic fluid collection (APFC) | <4 weeks, oedematous AP | Fluid | None |
| Pseudocyst | >4 weeks, oedematous AP | Fluid | Defined wall |
| Acute necrotic collection (ANC) | <4 weeks, necrotising AP | Fluid + necrosis | None |
| Walled-off necrosis (WON) | >4 weeks, necrotising AP | Fluid + necrosis | Defined wall |
Complications
Local:
- Pancreatic necrosis (sterile or infected)
- Pseudocyst formation
- Pancreatic duct disruption
- Splenic vein thrombosis, pseudoaneurysm
- Colonic infarction (middle colic or right colic artery thrombosis — presents with rapid haemodynamic collapse)
Systemic:
- Hypovolaemia and shock
- Acute kidney injury
- Acute respiratory distress syndrome (ARDS) / pleural effusion
- Hepatic failure
- Hypocalcaemia
- Hyperglycaemia/diabetes
Management
Initial Resuscitation
- IV fluid resuscitation is the cornerstone: aggressive early resuscitation with Lactated Ringer's solution is preferred over normal saline (lower incidence of acidosis/SIRS); rate typically 250–500 mL/h adjusted to urine output, BUN, and haematocrit
- Oxygen supplementation; intubation for ARDS if needed
- Urinary catheter to monitor hourly urine output (target >0.5 mL/kg/h)
- Analgesia: IV opioids (morphine, hydromorphone) — older concerns about morphine causing sphincter of Oddi spasm are not clinically significant; meperidine is no longer preferred due to toxic metabolite accumulation
Monitoring
- Serial vital signs, fluid balance
- Monitor BUN, creatinine, haematocrit, calcium every 6–12 hours initially
- APACHE II or SOFA scores to guide ICU transfer
Nutrition
- Mild AP: early oral feeding (soft, low-fat diet) as soon as tolerated — no need for NPO/bowel rest
- Severe AP: enteral nutrition (via nasojejunal tube) is preferred over total parenteral nutrition (TPN); reduces infectious complications and mortality
- TPN is reserved for patients who cannot tolerate enteral feeds
Specific Interventions
Gallstone AP (biliary pancreatitis):
- Early ERCP with sphincterotomy within 24–72 hours if concurrent cholangitis or persistent biliary obstruction
- Cholecystectomy should be performed during the same admission or early after recovery to prevent recurrence
Infected pancreatic necrosis:
- Suspected when clinical deterioration occurs after initial improvement or fever/rising WBC at >1 week
- CT-guided fine needle aspiration (FNA) with Gram stain and culture can confirm
- Step-up approach: antibiotics (imipenem, meropenem, or ciprofloxacin + metronidazole) → percutaneous catheter drainage → minimally invasive necrosectomy → open surgery as last resort
- Prophylactic antibiotics are not recommended routinely in sterile necrotising AP
Hypertriglyceridaemia-induced AP:
- Insulin infusion, plasmapheresis in severe cases; fibrates for long-term prevention
Medications to Avoid
- NSAIDs (worsen renal perfusion in hypovolaemia)
- Prophylactic antibiotics in uncomplicated AP
Prognosis
- ~80% of AP cases are mild and self-limiting, resolving in 3–5 days
- ~20% have severe disease with local or systemic complications
- Mortality: ~3–5% overall; up to 20–30% in severe necrotising pancreatitis with multiorgan failure
- Colonic infarction from colic artery thrombosis carries an extremely high mortality and requires emergent laparotomy
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Grainger & Allison's Diagnostic Radiology | Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.