Top 10 heart disease and there ecg report and ecg images
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram myocardial infarction ST elevation
Finding Sources
Searching Images
atrial fibrillation ECG irregular rhythm no P waves
Searching Images
heart failure cardiomyopathy ECG left ventricular hypertrophy
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
complete heart block third degree AV block ECG bradycardia
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy voltage
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave pre-excitation
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
Searching Images
pericarditis ECG saddle shaped ST elevation diffuse
Here is a comprehensive guide to the Top 10 Heart Diseases with their ECG findings and representative ECG images.
Top 10 Heart Diseases — ECG Findings & Images
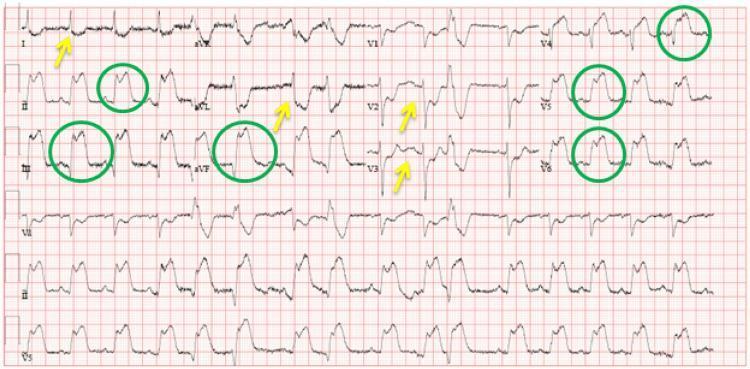
1. 🔴 ST-Elevation Myocardial Infarction (STEMI)
ECG Findings:
| Feature | Description |
|---|---|
| Rhythm | Sinus (may develop VT/VF) |
| ST Segments | Convex (tombstone) ST elevation ≥1 mm in ≥2 contiguous leads |
| Reciprocal Changes | ST depression in opposing leads |
| Hyperacute T-waves | Tall, peaked T-waves (earliest sign) |
| Q Waves | Pathological Q waves develop later (necrosis) |
| Territory | Anterior (V1–V6, LAD), Inferior (II, III, aVF, RCA), Lateral (I, aVL, V5–V6) |
Key teaching point: ST elevation in V2–V4 = LAD occlusion; II, III, aVF = RCA occlusion. Reciprocal depression confirms STEMI.

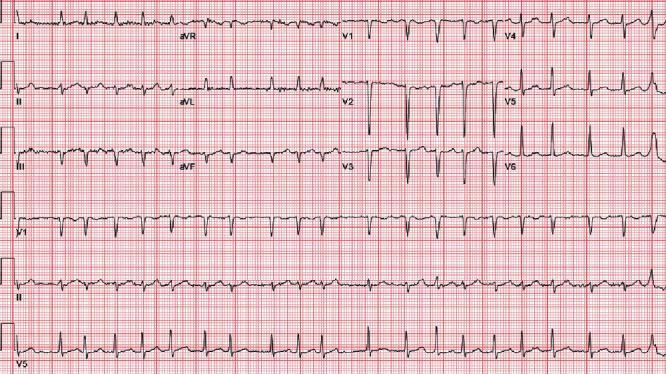
2. 💜 Atrial Fibrillation (AF)
ECG Findings:
| Feature | Description |
|---|---|
| Rhythm | Irregularly irregular — no two R-R intervals equal |
| P Waves | Absent; replaced by chaotic fibrillatory (f) waves |
| QRS | Narrow (unless aberrant conduction/WPW) |
| Rate | Ventricular rate varies; may be slow, normal, or fast |
| Baseline | Fine or coarse f-waves, best seen in V1 and II |
Key teaching point: "Irregularly irregular + no P waves = AF." Rate control target is 60–100 bpm at rest.
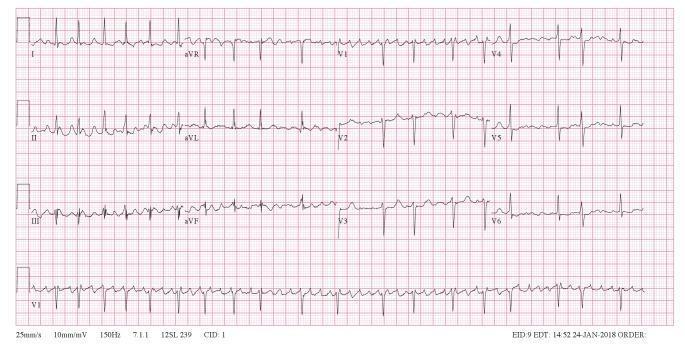
3. 💛 Ventricular Tachycardia (VT)
ECG Findings:
| Feature | Description |
|---|---|
| Rhythm | Regular (monomorphic) or irregular (polymorphic/torsades) |
| Rate | 100–250 bpm |
| QRS | Wide (>120 ms), bizarre morphology |
| P Waves | AV dissociation — P waves independent of QRS |
| Fusion/Capture Beats | Pathognomonic of VT |
| Axis | Often extreme left (northwest) axis |
Key teaching point: Wide complex tachycardia is VT until proven otherwise. Brugada criteria help differentiate VT from SVT with aberrancy.

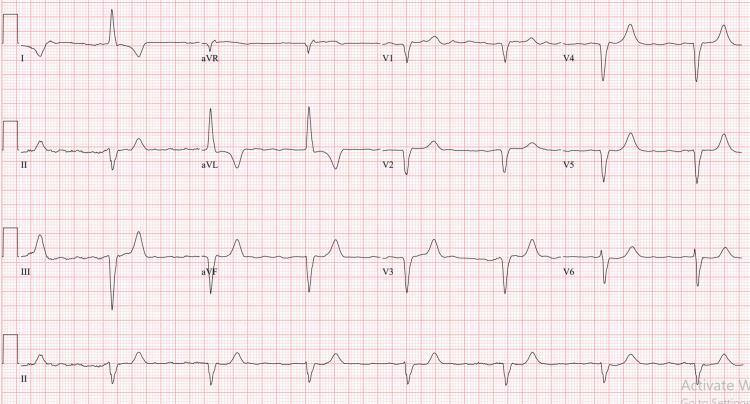
4. 💚 Complete (Third-Degree) Heart Block
ECG Findings:
| Feature | Description |
|---|---|
| Rhythm | P waves regular; QRS independent (AV dissociation) |
| Rate | Atrial rate > ventricular rate |
| PR Interval | No fixed PR interval |
| QRS | Wide if infranodal escape (junctional escape = narrow) |
| Ventricular Rate | 20–40 bpm (ventricular escape) |
Key teaching point: Complete AV dissociation with ventricular rate < atrial rate = third-degree block. Pacemaker required.

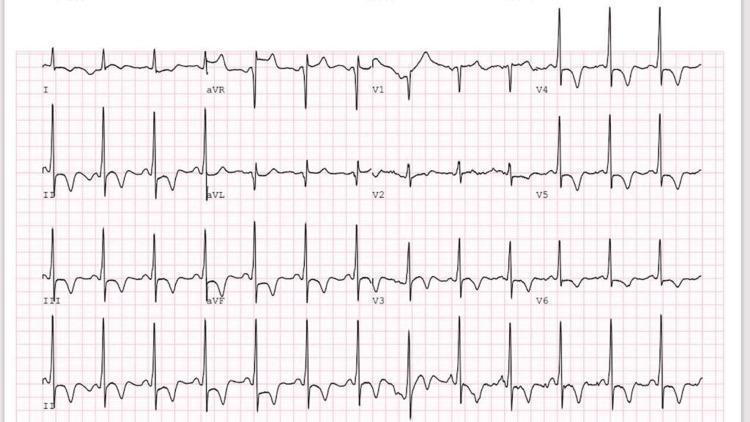
5. 🟠 Hypertrophic Cardiomyopathy (HCM)
ECG Findings:
| Feature | Description |
|---|---|
| LVH Voltage | High-amplitude QRS (Sokolow: SV1 + RV5/6 ≥ 35 mm) |
| T-Wave Inversions | Deep, symmetric ("giant") T-wave inversions V2–V6 (apical HCM/Yamaguchi) |
| Septal Q Waves | Deep, narrow Q waves in I, aVL, V5–V6 (septal hypertrophy) |
| ST Depression | Horizontal/downsloping in lateral leads |
| Rhythm | Sinus; AF common; risk of VT/VF |
Key teaching point: Giant negative T waves ≥10 mm in precordial leads in apical HCM (Yamaguchi syndrome) is a classic ECG signature.
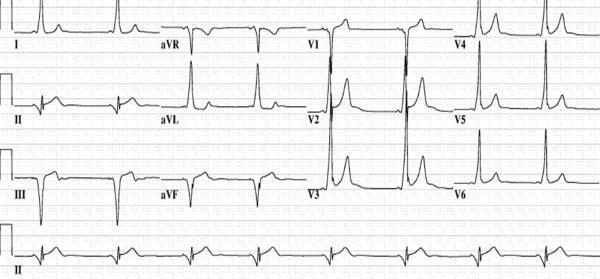
6. 🔵 Wolff-Parkinson-White Syndrome (WPW)
ECG Findings:
| Feature | Description |
|---|---|
| PR Interval | Short (<120 ms) — accessory pathway bypasses AV node |
| Delta Wave | Slurred upstroke at onset of QRS (pre-excitation) |
| QRS Duration | Wide (>120 ms) due to fusion beat |
| ST/T Changes | Secondary repolarization abnormalities (discordant) |
| Pseudo-infarct | Negative delta waves in inferior leads mimic Q waves |
| Risk | AF with rapid conduction → ventricular fibrillation (avoid AV nodal blockers) |
Key teaching point: Short PR + delta wave + wide QRS = WPW. Posteroseptal pathway = negative delta in II, III, aVF.

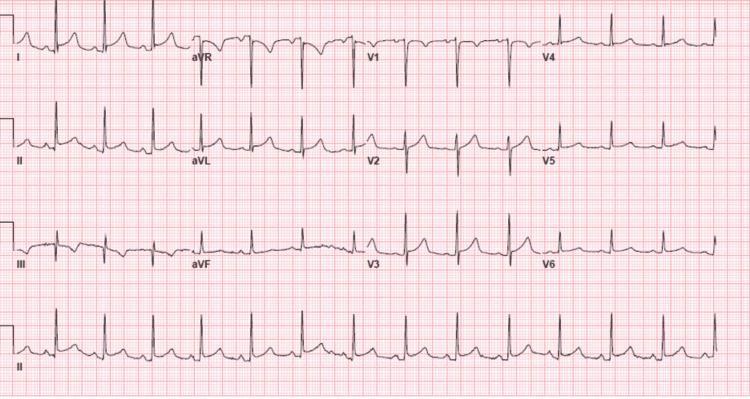
7. 🟡 Acute Pulmonary Embolism (PE)
ECG Findings:
| Feature | Description |
|---|---|
| Most Common | Sinus tachycardia (most sensitive but non-specific) |
| S1Q3T3 | S wave in I + Q wave in III + T-wave inversion in III (classic) |
| RBBB | New incomplete or complete right bundle branch block |
| Right Axis Deviation | Shift from baseline axis |
| T-wave Inversions | V1–V4 (right ventricular strain) |
| P Pulmonale | Tall peaked P waves in II (right atrial strain) |
Key teaching point: S1Q3T3 is specific (but insensitive ~20%). The most useful ECG finding is new sinus tachycardia with right-sided changes in a dyspneic patient.


8. 🟣 Acute Pericarditis
ECG Findings:
| Feature | Description |
|---|---|
| Stage 1 | Diffuse saddle-shaped (concave) ST elevation in all leads except aVR and V1; PR depression |
| Stage 2 | ST normalizes; T-wave inversions develop |
| Stage 3 | Deep T-wave inversions |
| Stage 4 | Normalization |
| Key Distinguisher | Diffuse ST elevation (no culprit vessel territory) + PR depression in II; PR elevation in aVR |
| Spodick's Sign | Downsloping TP segment |
Key teaching point: PR depression in lead II with diffuse concave ST elevation distinguishes pericarditis from STEMI. No reciprocal changes (except aVR).

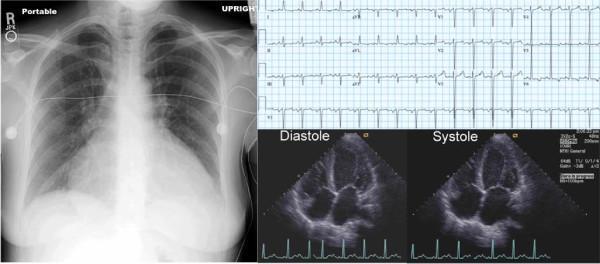
9. 🔶 Dilated Cardiomyopathy (DCM) / Congestive Heart Failure
ECG Findings:
| Feature | Description |
|---|---|
| LVH Voltage | High QRS voltage (may be low voltage in advanced/amyloid) |
| LBBB | Left bundle branch block very common (QRS >120 ms, broad notched R in I, V5–V6) |
| Q Waves | May simulate old MI (pseudo-infarct) |
| AF | Frequent comorbid arrhythmia |
| Sinus Tachycardia | Compensatory |
| Prolonged QRS | Poor prognosis; candidate for CRT (cardiac resynchronization therapy) |
Key teaching point: LBBB in a patient with reduced EF is an indication for CRT if QRS ≥150 ms. Low voltage in amyloid DCM contrasts with echocardiographic "sparkling" hypertrophy.
10. 🟤 Non-ST Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
ECG Findings:
| Feature | Description |
|---|---|
| ST Depression | Horizontal or downsloping ≥0.5–1 mm in ≥2 contiguous leads |
| T-wave Inversions | Symmetric, deep — especially in Wellens syndrome (V2–V3) |
| No ST Elevation | Key distinction from STEMI |
| Transient Changes | May normalize between episodes |
| Wellens Syndrome | Type A: biphasic T V2–V3; Type B: deep symmetric T inversion V2–V3 — proximal LAD lesion |
| Normal ECG possible | Up to 1–6% of NSTEMI have normal ECG |
Key teaching point: Wellens syndrome T-wave pattern without chest pain at the time of ECG = critical proximal LAD stenosis requiring urgent cath — do NOT stress test.

Quick Reference Summary Table
| # | Condition | Rhythm | Key ECG Feature | Emergency Action |
|---|---|---|---|---|
| 1 | STEMI | Sinus | Convex ST elevation ≥1 mm | PCI within 90 min |
| 2 | Atrial Fibrillation | Irregularly irregular | No P waves, f-waves | Rate/rhythm control, anticoagulation |
| 3 | Ventricular Tachycardia | Regular, fast | Wide QRS >120 ms, AV dissociation | Cardioversion/amiodarone |
| 4 | Complete Heart Block | Slow ventricular escape | AV dissociation, no PR relationship | Temporary pacing |
| 5 | Hypertrophic CM | Sinus | Giant T inversions, LVH voltage | Beta-blockers, ICD if high risk |
| 6 | WPW | Variable | Short PR, delta wave, wide QRS | Ablation; avoid AV nodal drugs in AF |
| 7 | Pulmonary Embolism | Sinus tachycardia | S1Q3T3, RBBB, RV strain | Anticoagulation ± thrombolysis |
| 8 | Pericarditis | Sinus | Diffuse concave ST elevation, PR depression | NSAIDs + colchicine |
| 9 | Dilated CM / HF | Sinus/AF | LBBB, LVH, Q waves | Guideline-directed medical therapy, CRT |
| 10 | NSTEMI / Unstable Angina | Sinus | ST depression, T inversions (Wellens) | Antiplatelet, anticoagulation, early cath |
Clinical pearl: Always compare the ECG with a prior baseline when available. Serial ECGs 15–30 minutes apart can reveal dynamic changes that confirm or exclude acute ischemia.
This is a shared conversation. Sign in to Orris to start your own chat.