Type 1 and type 2 mi
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is a detailed breakdown:
Type 1 vs Type 2 Myocardial Infarction
These are distinct categories within the Fourth Universal Definition of MI (Thygesen et al., JACC 2018), which classifies MI into five types based on underlying mechanism.
Type 1 MI — Spontaneous (Atherothrombotic)
Mechanism: Caused by atherosclerotic plaque rupture, ulceration, fissuring, erosion, or dissection with resulting intraluminal thrombosis in one or more coronary arteries, leading to decreased myocardial blood flow or distal platelet emboli with myocyte necrosis. The patient may have underlying severe CAD but on occasion nonobstructive or no CAD.
Key features:
- The "classic" heart attack
- Thrombotic occlusion of a coronary artery at the site of plaque disruption
- Encompasses STEMI and NSTEMI presentations
- Treatment is directed at restoring coronary patency: primary PCI, thrombolytics, antiplatelet/anticoagulation therapy
- In COVID-19, viral PAMPs entering the systemic circulation can activate immune receptors on atherosclerotic plaques, predisposing to plaque rupture and Type 1 MI — associated with higher thrombus burden and worse outcomes
Troponin pattern: Rises sharply from near-zero, crossing the 99th percentile URL within 6–12 hours, reaching very high peak values (~150× URL), then gradually falling — a classic rise-and-fall pattern with a strongly positive delta.
Type 2 MI — Ischemic Imbalance (Supply-Demand Mismatch)
Mechanism: Myocardial injury with necrosis in which a condition other than CAD contributes to an imbalance between myocardial oxygen supply and/or demand.
Causes include:
- Coronary endothelial dysfunction
- Coronary artery spasm
- Coronary embolism
- Tachyarrhythmia or bradyarrhythmia
- Anemia
- Respiratory failure / hypoxemia
- Hypotension or severe hypertension (with or without LV hypertrophy)
Key features:
- No primary thrombotic event — the infarction is the consequence of another underlying process
- Management is directed at the underlying cause (e.g., treat the arrhythmia, correct anemia, treat sepsis), not at coronary reperfusion
- In COVID-19, relevant Type 2 mechanisms include fixed atherosclerosis limiting perfusion during physiological stress, coronary microvascular endothelial dysfunction, severe hypertension from elevated angiotensin II, and hypoxemia from ARDS or pulmonary vascular thrombosis
Troponin pattern: Rises to a lower peak (~45× URL) than Type 1, with a blunted rise-and-fall curve. The delta may be less dramatic.
Troponin Kinetics: Type 1 vs Type 2 vs Chronic Injury
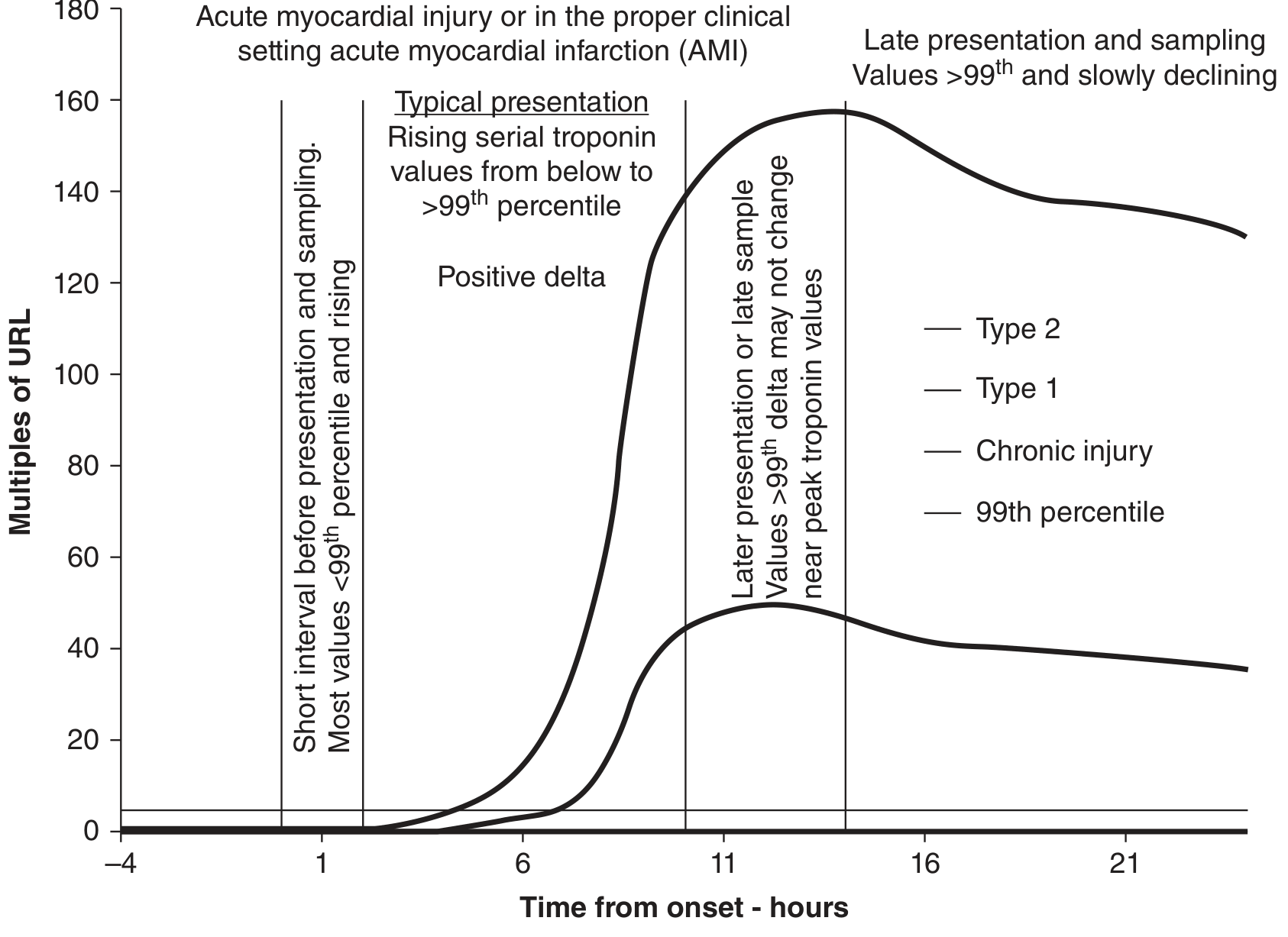
Rise and fall profile of cardiac troponin for Type 1 MI, Type 2 MI, and chronic myocardial injury. Type 1 reaches markedly higher peak values than Type 2. Chronic injury remains chronically elevated above the 99th percentile URL but without the acute rise-fall pattern. — Tietz Textbook of Laboratory Medicine, 7th Ed.
Summary Comparison
| Feature | Type 1 MI | Type 2 MI |
|---|---|---|
| Primary mechanism | Plaque rupture → thrombosis | Supply-demand imbalance |
| Coronary artery | Usually obstructed acutely | May be patent or mildly diseased |
| Underlying cause | Atherosclerosis | Arrhythmia, anemia, hypoxia, spasm, etc. |
| Troponin peak | Very high (e.g., ~150× URL) | Lower (e.g., ~45× URL) |
| ECG changes | STEMI or NSTEMI pattern | Variable |
| Treatment target | Coronary reperfusion (PCI/lysis) | Treat the precipitating cause |
| Antiplatelet/anticoagulation | Core therapy | Role is less well-defined |
The Other MI Types (for context)
- Type 3: MI causing sudden cardiac death before biomarkers can be drawn
- Type 4a/4b: PCI-related MI (cTn >5× URL) or stent thrombosis
- Type 5: CABG-related MI (cTn >10× URL)
— Tietz Textbook of Laboratory Medicine, 7th Ed.; Sabiston Textbook of Surgery; Fuster and Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.