chest pain. definition, epidemiology,etiology, pathogenesis, histopathology, clinical features, diagnosis, management,prognosis, complications,and differential diagnosis (table). along with images
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks plus key images. Let me compile the full, detailed response.
Chest Pain: A Comprehensive Clinical Review
1. Definition
Chest pain is a symptom defined as any discomfort, pressure, tightness, heaviness, burning, or frank pain perceived anywhere between the jaw and the epigastrium, arising from structures within or adjacent to the thorax. It is one of the most common and diagnostically challenging presentations in clinical medicine, ranging from benign musculoskeletal strain to immediately life-threatening cardiovascular emergencies.
The cardinal manifestation of myocardial ischemia is chest discomfort or pain resulting from coronary artery disease or any condition creating an imbalance between myocardial oxygen supply and demand. However, many non-cardiac structures - lungs, pleura, esophagus, chest wall, and diaphragm - can generate identical or indistinguishable pain.
Goldman-Cecil Medicine: "Chest discomfort or pain is the cardinal manifestation of myocardial ischemia resulting from coronary artery disease or any condition that causes myocardial ischemia by an imbalance of myocardial oxygen demand compared with myocardial oxygen supply."
2. Epidemiology
- Approximately 7.5 million patients visit emergency departments (EDs) in the United States each year with chest pain, constituting ~5% of all ED visits - making it the second most common ED complaint.
- Chest pain is a daily presentation in virtually every ED, large or small, academic or community.
- The epidemiology of critical diagnoses causing chest pain varies widely:
- Acute Coronary Syndrome (ACS) accounts for 15-25% of ED chest pain presentations
- Pulmonary embolism causes 2-4%
- Aortic dissection is rare but devastating (<1%)
- Musculoskeletal causes account for 20-40% (most common overall)
- Gastrointestinal causes (GERD, esophageal spasm): 10-20%
- Psychogenic/anxiety: 5-10%
- Women and older individuals may present with atypical symptoms and are more likely to have advanced coronary disease despite fewer classic complaints.
- In children, the most common causes are musculoskeletal (chest wall), asthma, pneumonia, pleurisy, GERD, and precordial catch syndrome. Cardiac causes are rare but must be excluded with exertional pain or a family history of sudden unexplained death.
Rosen's Emergency Medicine: "Approximately 7.5 million patients visit the emergency department each year with complaints of chest pain, constituting 5% of all patients seen in EDs in the United States."
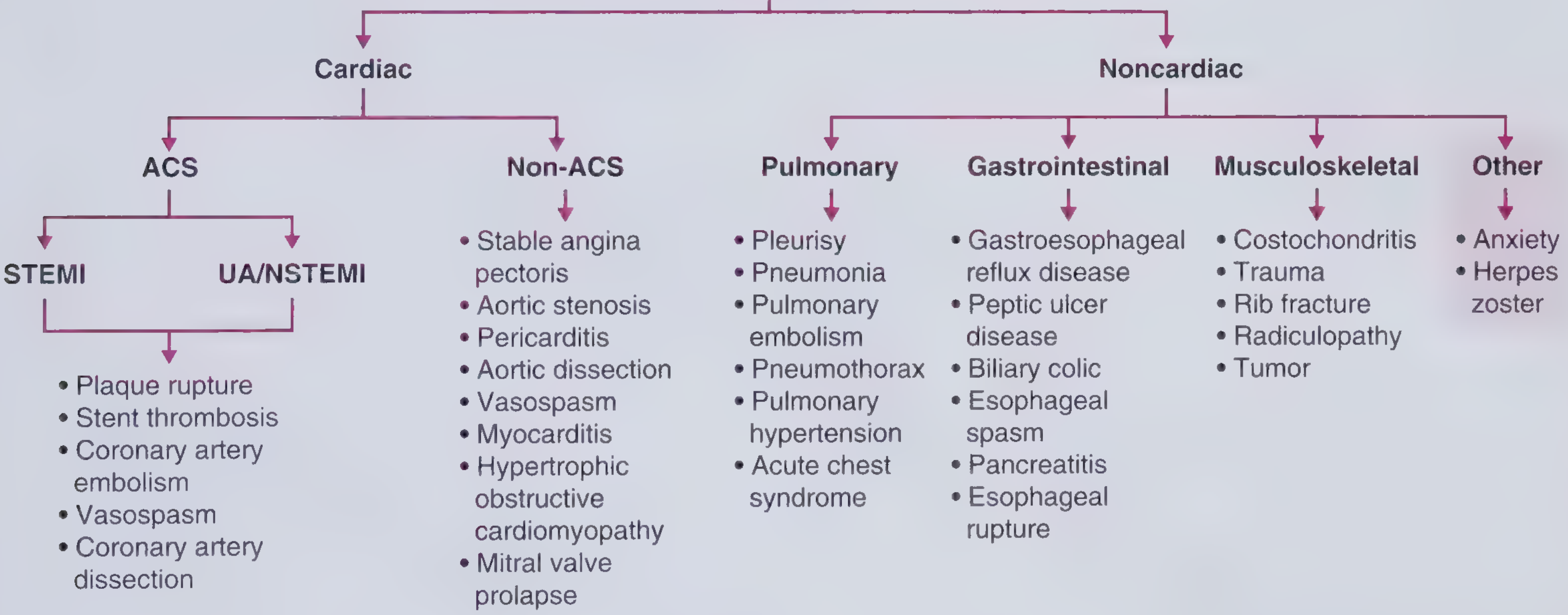
3. Etiology
Chest pain has a broad differential diagnosis spanning multiple organ systems:
Cardiac (Ischemic and Non-Ischemic)
| Category | Conditions |
|---|---|
| ACS (Ischemic) | STEMI, NSTEMI, Unstable angina |
| Stable angina | Exertional ischemia from fixed atherosclerotic lesion |
| Vasospasm | Prinzmetal (variant) angina, cocaine-induced |
| Structural cardiac | Aortic stenosis, hypertrophic obstructive cardiomyopathy, mitral valve prolapse |
| Pericarditis/myocarditis | Viral, autoimmune, post-MI (Dressler syndrome) |
| Aortic dissection | Type A (ascending), Type B (descending) |
| Cardiac tamponade | Pericardial effusion with hemodynamic compromise |
Pulmonary
- Pulmonary embolism, tension pneumothorax, spontaneous pneumothorax
- Pneumonia, pleuritis, mediastinitis, pulmonary hypertension
- Acute chest syndrome (sickle cell disease)
Gastrointestinal
- Esophageal rupture (Boerhaave syndrome) - catastrophic
- Esophageal spasm, GERD, Mallory-Weiss tear
- Peptic ulcer disease, cholecystitis, pancreatitis
Musculoskeletal
- Costochondritis, rib fracture, muscle strain
- Thoracic disc herniation, arthritis
Neurologic
- Herpes zoster (before rash appears), postherpetic neuralgia
- Spinal root compression, thoracic outlet syndrome
Psychogenic/Other
- Panic disorder, anxiety, hyperventilation syndrome
- Malingering, somatization disorder
4. Pathogenesis / Pathophysiology
The mechanism of chest pain is rooted in visceral pain neuroscience:
-
Shared afferent pathways: Afferent fibers from the heart, lungs, great vessels, and esophagus enter the same thoracic dorsal ganglia (T1-T5). This convergence means each organ produces the same indistinct quality and location of pain - the brain cannot distinguish the source.
-
Dermatomal overlap: Because dorsal segments overlap three levels above and below, disease of thoracic origin can produce pain anywhere from the jaw to the epigastrium.
-
Referred pain: Radiation to the arm, shoulder, neck, and jaw is caused by somatic afferent fibers synapsing in the same dorsal root ganglia as the thoracic viscera, confusing the CNS into misperceiving the origin.
-
Ischemic mechanism: Myocardial ischemia activates chemosensitive and mechanosensitive receptors in the myocardium, releasing adenosine, bradykinin, and other mediators that stimulate cardiac sympathetic afferents.
-
Visceral hypersensitivity: In noncardiac chest pain (especially esophageal), central sensitization and visceral hypersensitivity amplify pain signals from minor stimuli (low esophageal pressure, minor acid reflux).
Rosen's Emergency Medicine: "Afferent fibers from the heart, lungs, great vessels, and esophagus enter the same thoracic dorsal ganglia. Through these visceral fibers, each organ produces the same indistinct quality and location of pain... Because dorsal segments overlap three segments above and below a level, disease of a thoracic origin can produce pain anywhere from the jaw to the epigastrium."
Ischemic chest pain specifically:
- An imbalance between myocardial O₂ demand (increased by HR, contractility, wall stress) and supply (decreased by stenosis, spasm, or thrombosis) triggers anaerobic metabolism
- Metabolic byproducts (H⁺, lactate, adenosine) stimulate nociceptors
- In ACS: plaque rupture triggers thrombosis → sudden coronary occlusion → ischemia/infarction
- In stable angina: fixed atherosclerotic stenosis limits flow during increased demand
5. Histopathology
Histopathology is specific to the underlying etiology:
Myocardial Infarction
- 0-6 hours: Coagulative necrosis begins; wavy myofiber change; contraction bands
- 12-24 hours: Neutrophilic infiltrate; pallor and early necrosis visible
- 1-5 days: Prominent neutrophil infiltration; myocytes ghost outlines
- 5-10 days: Macrophage infiltration; granulation tissue; capillary in-growth
- 2-8 weeks: Fibrosis and scar formation (collagen replacement)
Pericarditis
- Fibrinous exudate on epicardial surface
- Lymphocytic and plasma cell infiltration
- In chronic/constrictive: dense fibrous pericardial thickening
Aortic Dissection
- Cystic medial necrosis: fragmentation and loss of elastic fibers in the media
- Smooth muscle cell death; mucoid pooling
- Intimal tear allows blood to dissect between intima and adventitia
Pulmonary Embolism
- Vascular thrombus (predominantly fibrin and platelets)
- Pulmonary infarction (hemorrhagic, wedge-shaped, pleura-based)
- Organizing thrombus in chronic PE: fibrous recanalization
Esophageal Causes (GERD)
- Barrett's esophagus: columnar metaplasia replacing squamous epithelium
- Esophageal spasm: smooth muscle hypertrophy
6. Clinical Features
Character of Pain
The Diamond-Forrester classification categorizes chest pain into:
| Type | Criteria Met | Pre-test Probability |
|---|---|---|
| Typical angina | All 3 criteria | High |
| Atypical angina | 2 criteria | Intermediate |
| Noncardiac | ≤1 criterion | Low |
Three criteria:
- Substernal pressure-like discomfort
- Precipitated by exertion or emotional stress
- Relieved by rest or nitroglycerin within <30 minutes
Fuster & Hurst's The Heart: "It is important to remember that there are many patients who will not use the term 'pain' when describing their angina. Instead, they may describe their symptoms in other terms such as 'pressure, ache, discomfort, uneasy feelings.' These sensations may not always be substernal but often are felt in the neck, lower jaw, shoulder, and arm down to the wrist."
Pain Characteristics by Etiology
| Condition | Character | Location | Radiation | Duration | Aggravating | Relieving |
|---|---|---|---|---|---|---|
| Stable angina | Pressure, squeezing, heaviness | Substernal | Arm, neck, jaw | <5 min | Exertion, cold, meals | Rest, GTN |
| ACS/STEMI | Pressure, crushing, severe | Substernal | Left arm, jaw | >20-30 min | None (occurs at rest) | Morphine (not GTN) |
| Aortic dissection | Tearing, ripping | Anterior chest/back | Back, abdomen | Sudden onset, sustained | Hypertension | None |
| Pericarditis | Sharp, pleuritic | Anterior/retrosternal | Shoulder/trapezius | Hours to days | Supine, inspiration | Leaning forward |
| Pulmonary embolism | Pleuritic, sharp | Lateral, pleuritic | None | Sudden onset | Inspiration | None |
| Pneumothorax | Sharp | Lateral chest | Ipsilateral shoulder | Sudden | Inspiration | None |
| GERD | Burning, pressure | Substernal | Throat | Minutes-hours | Meals, supine | Antacids |
| Esophageal spasm | Severe, squeezing | Substernal | Back | Minutes | Swallowing cold | GTN, CCB |
| Costochondritis | Sharp | Costal cartilage | None | Persistent | Palpation, movement | NSAIDs |
| Herpes zoster | Burning, dermatomal | Unilateral | Dermatomal | Days | Touch | Antivirals |
Associated Symptoms
- Diaphoresis, nausea, vomiting: Strongly suggest ACS (autonomic activation)
- Dyspnea: Pulmonary embolism, tension pneumothorax, heart failure
- Syncope: Massive PE, aortic dissection, HOCM, aortic stenosis
- Hemoptysis: Pulmonary embolism, pulmonary infarction
- Fever: Pericarditis, myocarditis, pneumonia
- Neurological deficits: Aortic dissection involving great vessels
7. Diagnosis
Initial Assessment Algorithm
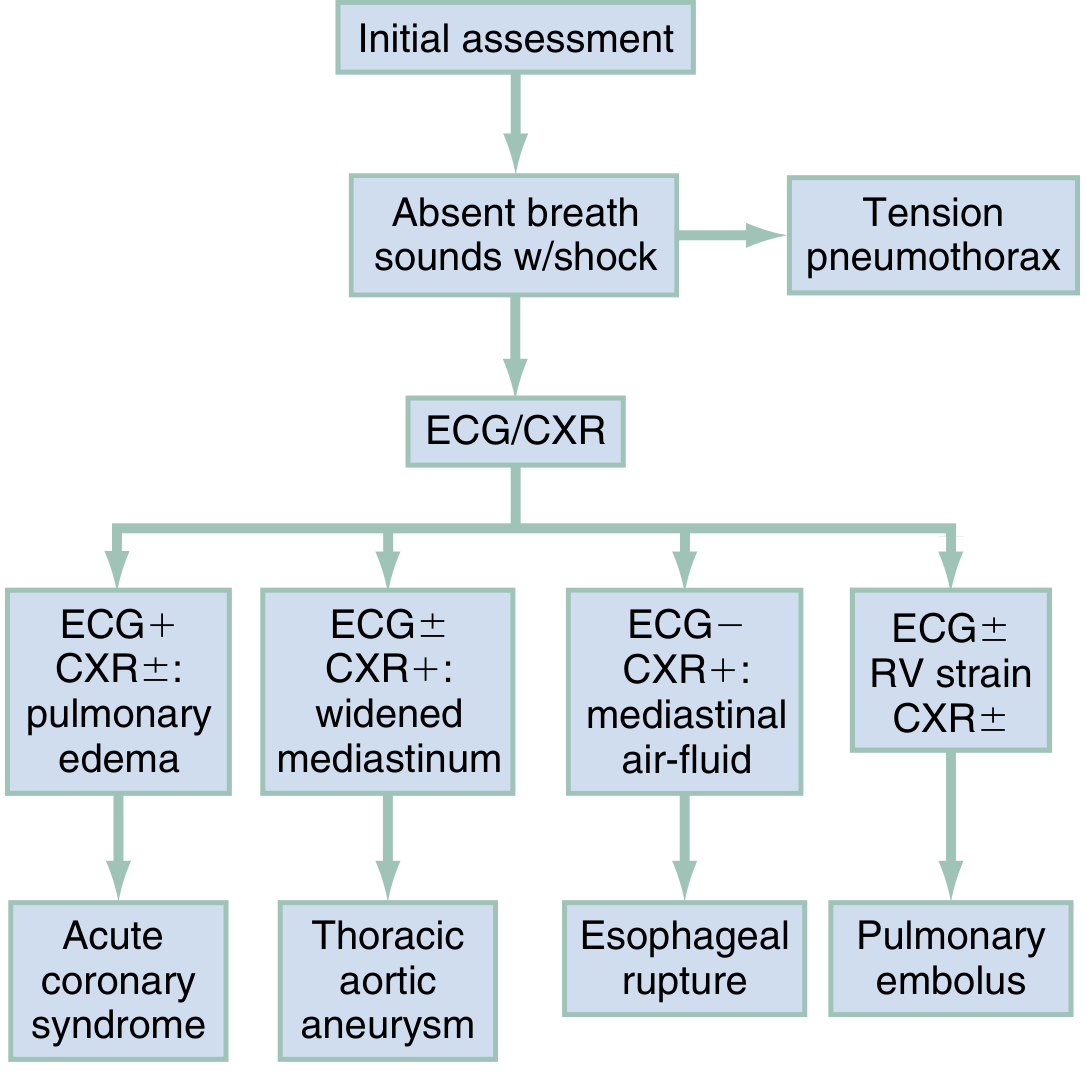
Step-by-Step Diagnostic Approach
1. History (80-90% of diagnosis)
- Onset, character, severity (1-10), location, radiation
- Duration, temporal pattern
- Aggravating/relieving factors
- Associated symptoms
- Cardiac risk factors: hypertension, diabetes, hyperlipidemia, smoking, family history
- Prior cardiac history
2. Physical Examination
- Vital signs: BP (both arms for dissection), HR, SpO₂
- General appearance: diaphoresis, pallor, cyanosis, distress
- Neck: JVP, carotid bruits
- Chest: breath sounds (absent = pneumothorax), rubs (pericarditis/pleuritis), crackles (pulmonary edema)
- Heart: murmurs (AS, HOCM, MVP), S3/S4, rubs
- Abdomen: tenderness (pancreatitis, cholecystitis)
- Extremities: pulse discrepancy (dissection), DVT signs (PE)
- Skin: vesicular rash (herpes zoster), reproducible tenderness on palpation (costochondritis/musculoskeletal)
3. Electrocardiogram (ECG) - FIRST-LINE, within 10 minutes
- STEMI: ST elevation ≥1mm in ≥2 contiguous leads; new LBBB
- NSTEMI/UA: ST depression, T-wave inversions
- STEMI equivalents: Posterior MI (ST depression V1-V4), Wellens pattern
- Pericarditis: Diffuse saddle-shaped ST elevation, PR depression
- PE: S1Q3T3, sinus tachycardia, right heart strain, new RBBB
- LVH: Suggests longstanding hypertension or aortic stenosis
4. Laboratory Tests
| Test | Purpose |
|---|---|
| Troponin I/T (high-sensitivity) | Myocardial injury; serial at 0h and 1-3h |
| BNP / NT-proBNP | Heart failure, RV strain |
| D-dimer | Exclude PE (if pre-test probability low/intermediate) |
| CBC | Anemia, infection |
| CMP | Renal function, electrolytes |
| Lipase/amylase | Pancreatitis |
| ABG | Hypoxemia, acidosis |
| CRP/ESR | Pericarditis, myocarditis |
5. Imaging
| Modality | Key Findings |
|---|---|
| Chest X-ray | Widened mediastinum (dissection), cardiomegaly, pleural effusion, pneumothorax, infiltrates |
| CT Angiography (CTA) | Gold standard for aortic dissection; diagnosis of PE (CTPA); rule out other causes |
| Echocardiography (TTE/TEE) | Wall motion abnormalities (ischemia), pericardial effusion, valvular disease, RV dilation (PE), aortic root |
| Coronary angiography | Definitive for coronary artery disease |
| V/Q scan | PE in patients where CTPA contraindicated (CKD, contrast allergy) |
| Cardiac MRI | Myocarditis, pericarditis, cardiomyopathy workup |
6. Risk Stratification: The HEART Score
For suspected ACS in the ED, the HEART score is validated for risk stratification:
| Variable | 0 | 1 | 2 |
|---|---|---|---|
| History | Slightly suspicious | Moderately suspicious | Highly suspicious |
| ECG | Normal | Non-specific repolarization | Significant ST changes |
| Age | <45 | 45-65 | >65 |
| Risk factors | No known factors | 1-2 factors | ≥3 factors or atherosclerotic disease |
| Troponin | ≤Normal | 1-3× normal | >3× normal |
- Score 0-3: Low risk - MACE rate ~1.7% → safe for discharge
- Score 4-6: Intermediate - MACE ~12-17% → observation, serial troponins, cardiology
- Score 7-10: High risk - MACE ~50-65% → admission, likely coronary intervention
Rosen's Emergency Medicine: "Information pertinent to the differential diagnosis is obtained through the directed history, physical examination, and ECG in 80% to 90% of patients."
8. Management
Management is etiology-directed. Below is the approach by condition:
Immediate Life-Threatening Conditions
STEMI (Acute MI with ST elevation):
- Aspirin 325 mg + P2Y12 inhibitor (clopidogrel/ticagrelor/prasugrel)
- Primary PCI within 90 minutes (door-to-balloon time) - preferred
- Fibrinolysis if PCI not available within 120 minutes
- Anticoagulation (heparin/bivalirudin), nitrates, oxygen if SpO₂ <90%
- Beta-blockers (if no contraindications), ACE inhibitors within 24h
NSTEMI/Unstable Angina:
- Aspirin + P2Y12 inhibitor, anticoagulation, nitrates, beta-blockers
- Risk stratify with HEART score, serial troponins
- High-risk: early invasive strategy (coronary angiography within 24h)
- Low-risk: conservative management with noninvasive testing
Aortic Dissection:
- Urgent IV beta-blockade (target HR <60 bpm) FIRST, then reduce BP to SBP 100-120 mmHg
- CT angiography for diagnosis
- Type A (ascending): Emergency surgical repair
- Type B (descending): Medical management (unless complications - TEVAR)
Pulmonary Embolism:
- Anticoagulation: heparin bridge to warfarin or direct oral anticoagulants (DOACs)
- Massive PE with hemodynamic instability: systemic thrombolysis (alteplase)
- Submassive PE: consider catheter-directed thrombolysis
- High suspicion + low risk of bleeding: anticoagulate empirically while awaiting imaging
Tension Pneumothorax:
- Immediate needle decompression (2nd intercostal space, midclavicular line) followed by chest tube
Cardiac Tamponade:
- Emergent pericardiocentesis (echocardiography-guided preferred)
Non-Immediately-Life-Threatening Conditions
| Condition | Management |
|---|---|
| Stable angina | Anti-anginals (beta-blockers, CCBs, nitrates), antiplatelet, statins, risk factor modification; revascularization if refractory |
| Pericarditis | NSAIDs (ibuprofen/aspirin) + colchicine for 3 months; avoid anticoagulation |
| GERD | PPI, lifestyle modification, H2 blockers |
| Esophageal spasm | CCBs, nitrates, PPIs; psychiatric/CBT if functional |
| Costochondritis | NSAIDs, local heat, rest |
| Anxiety/Panic | Benzodiazepines (acute), SSRIs (long-term), CBT |
| Pneumonia/Pleuritis | Antibiotics, NSAIDs for pleuritis |
9. Differential Diagnosis (Table)
| System | Critical/Emergent | Urgency | Key Distinguishing Feature |
|---|---|---|---|
| Cardiovascular | STEMI | Critical | ST elevation, crushing pain, diaphoresis |
| NSTEMI/UA | Critical | Troponin rise, ST depression | |
| Aortic dissection | Critical | Tearing pain radiating to back, BP asymmetry | |
| Cardiac tamponade | Critical | Beck's triad: hypotension, JVD, muffled heart sounds | |
| Unstable angina | Emergent | Rest pain, no troponin rise | |
| Prinzmetal angina | Emergent | ST elevation at rest, nocturnal, normal coronaries | |
| Pericarditis | Emergent | Pleuritic, positional, pericardial rub, diffuse ST elevation | |
| Myocarditis | Emergent | Troponin rise, fever, viral prodrome | |
| Aortic stenosis | Non-emergent | Systolic ejection murmur, exertional angina, syncope | |
| Mitral valve prolapse | Non-emergent | Mid-systolic click, young women | |
| Pulmonary | Tension pneumothorax | Critical | Absent breath sounds, tracheal deviation, shock |
| Pulmonary embolism | Critical | Pleuritic pain, dyspnea, tachycardia, risk factors | |
| Pneumothorax | Emergent | Sudden onset, pleuritic, ipsilateral absent breath sounds | |
| Mediastinitis | Emergent | High fever, post-procedure | |
| Pneumonia | Non-emergent | Fever, cough, productive sputum, consolidation | |
| Pleuritis | Non-emergent | Pleuritic pain, friction rub | |
| Pulmonary hypertension | Non-emergent | Exertional dyspnea, right heart signs | |
| Gastrointestinal | Esophageal rupture (Boerhaave) | Critical | Mackler's triad: emesis + chest pain + subcutaneous emphysema; widened mediastinum |
| Mallory-Weiss tear | Emergent | Hematemesis after vomiting | |
| Cholecystitis | Emergent | RUQ pain, Murphy's sign, fever | |
| Pancreatitis | Emergent | Epigastric pain, elevated lipase | |
| GERD | Non-emergent | Burning, postprandial, responds to antacids | |
| Esophageal spasm | Non-emergent | Severe substernal, can mimic angina, responds to GTN/CCB | |
| Peptic ulcer disease | Non-emergent | Epigastric, food-related | |
| Musculoskeletal | - | Non-emergent | - |
| Costochondritis | Non-emergent | Reproducible tenderness on palpation of costal cartilages | |
| Rib fracture | Non-emergent | Trauma history, point tenderness, X-ray | |
| Muscle strain | Non-emergent | History of exertion/trauma, positional | |
| Cervical/thoracic disc | Non-emergent | Dermatomal radiation, neurological signs | |
| Neurological | Herpes zoster | Emergent | Dermatomal burning, vesicular rash (may precede rash by 48-72h) |
| Thoracic outlet syndrome | Non-emergent | Upper limb neurological symptoms | |
| Psychogenic | Panic disorder | Non-emergent | Episodic, hyperventilation, multiple somatic complaints, young patient |
| Anxiety | Non-emergent | Situational triggers, associated symptoms |
10. Prognosis
Prognosis depends entirely on the underlying cause:
| Condition | Prognosis |
|---|---|
| STEMI with timely PCI | 30-day mortality ~5%; good long-term outcome with secondary prevention |
| Aortic dissection Type A | Untreated: ~1-2% mortality per hour in first 24h; surgical survival ~70-80% |
| Massive PE | Mortality 25-65% without treatment; ~8% with treatment |
| Tension pneumothorax | Near 100% mortality if untreated; excellent with needle decompression |
| Esophageal rupture | Mortality rises sharply with delay >24h (>40% vs <10% if early repair) |
| Stable angina | Annual mortality 1-3%; depends on extent of CAD and LV function |
| Pericarditis (viral) | Generally excellent; recurrence in 20-30% |
| GERD/musculoskeletal/functional | Benign, though functional chest pain diminishes quality of life; patients may require repeated cardiac evaluations |
Goldman-Cecil Medicine: "Functional chest pain has a benign prognosis, although many patients may request repeated cardiac evaluations if symptoms persist and diminish quality of life."
11. Complications
Complications arise from either the underlying condition or delayed/missed diagnosis:
Cardiovascular
- Myocardial infarction → cardiogenic shock, arrhythmias (VF, VT, complete heart block), papillary muscle rupture, ventricular septal defect, free wall rupture, Dressler syndrome (post-MI pericarditis), heart failure
- Aortic dissection → aortic regurgitation, coronary artery compromise, stroke, mesenteric ischemia, renal failure, limb ischemia
- Pericarditis → constrictive pericarditis, pericardial effusion, tamponade
Pulmonary
- Pulmonary embolism → right heart failure, chronic thromboembolic pulmonary hypertension (CTEPH)
- Pneumothorax → tension pneumothorax, respiratory failure
Gastrointestinal
- Esophageal rupture → mediastinitis, sepsis, multi-organ failure (high mortality)
- GERD → Barrett's esophagus, esophageal adenocarcinoma, peptic stricture
Diagnostic Errors (iatrogenic complications)
- Missed ACS in atypical presentations → preventable death
- Over-diagnosis → unnecessary angiography, anticoagulation, radiation exposure
- Repeated negative workups → patient anxiety, healthcare resource utilization
Summary Reference Table
| Parameter | Key Points |
|---|---|
| Definition | Discomfort/pain between jaw and epigastrium from any thoracic or referred source |
| Most common cause | Musculoskeletal (20-40%), then cardiac ischemia |
| Life-threatening causes | STEMI, aortic dissection, PE, tension pneumothorax, tamponade, esophageal rupture |
| Key mechanism | Shared T1-T5 dorsal root ganglia for cardiac, pulmonary, esophageal afferents |
| First-line test | 12-lead ECG (within 10 minutes) + high-sensitivity troponin |
| Risk stratification | HEART score (0-3 low, 4-6 intermediate, 7-10 high risk) |
| Most important distinction | Cardiac ischemic vs. non-ischemic vs. non-cardiac |
Sources:
- Rosen's Emergency Medicine, 9th Edition - Chapters 22, 64
- Goldman-Cecil Medicine, International Edition - Chapters 39, 45
- Fuster and Hurst's The Heart, 15th Edition - Chapter 2
- Frameworks for Internal Medicine
- Braunwald's Heart Disease - Textbook of Cardiovascular Medicine
This is a shared conversation. Sign in to Orris to start your own chat.