Hoe to manage a 80 year old lady with complaint of spinning of head and dizziness
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive, evidence-based approach to managing an 80-year-old woman presenting with spinning and dizziness.
Managing Dizziness & Vertigo in an 80-Year-Old Woman
Why Age Matters
Dizziness prevalence increases with age due to:
- Decreased visual acuity
- Reduced proprioception
- Declining vestibular input
- Accumulation of free-floating otoconia (predisposing to BPPV)
- Polypharmacy (many medications cause dizziness)
— Tintinalli's Emergency Medicine
Step 1: Clarify the Type of Dizziness
"Dizziness" is imprecise. First categorize what she actually means:
| Type | Description | Common Causes |
|---|---|---|
| Vertigo | Spinning sensation (self or environment) | BPPV, vestibular neuritis, Ménière's, central |
| Presyncope | Light-headedness, faintness | Orthostatic hypotension, arrhythmia, medications |
| Disequilibrium | Imbalance without spinning | Sensory neuropathy, Parkinson's, cerebellar |
| Non-specific | Vague floating feeling | Anxiety, hyperventilation, medications |
Step 2: History — Key Questions
Timing & Triggers:
- Seconds — triggered by head movement or getting in/out of bed → think BPPV
- Hours — with hearing loss/tinnitus → Ménière's disease
- Hours — without hearing symptoms → vestibular migraine
- Minutes — with neurological symptoms → TIA (posterior circulation)
- Constant for days — with or without viral prodrome → vestibular neuritis
- On standing up → orthostatic hypotension
Associated symptoms to ask about:
- Unilateral hearing loss, ear fullness, tinnitus → peripheral cause
- Double vision, facial numbness, dysarthria, limb ataxia, headache → central cause / stroke (emergency)
- Neck pain → vertebral artery dissection
- Palpitations → cardiac arrhythmia
Medications review (crucial in elderly):
- Antihypertensives, diuretics, sedatives, antiepileptics, aminoglycosides, loop diuretics
Step 3: Examination
Vitals: Blood pressure lying and standing (orthostatic drop >20 mmHg systolic = orthostatic hypotension)
Ocular motility:
- Nystagmus — direction, persistence, fixation suppression
- Peripheral nystagmus: unidirectional, suppressed by fixation
- Central nystagmus: direction-changing with gaze, NOT suppressed by fixation; vertical nystagmus is a red flag
Head Impulse Test (HIT): Rapid small-amplitude head rotation while patient fixates on target. A "catch-up saccade" = peripheral vestibular lesion.
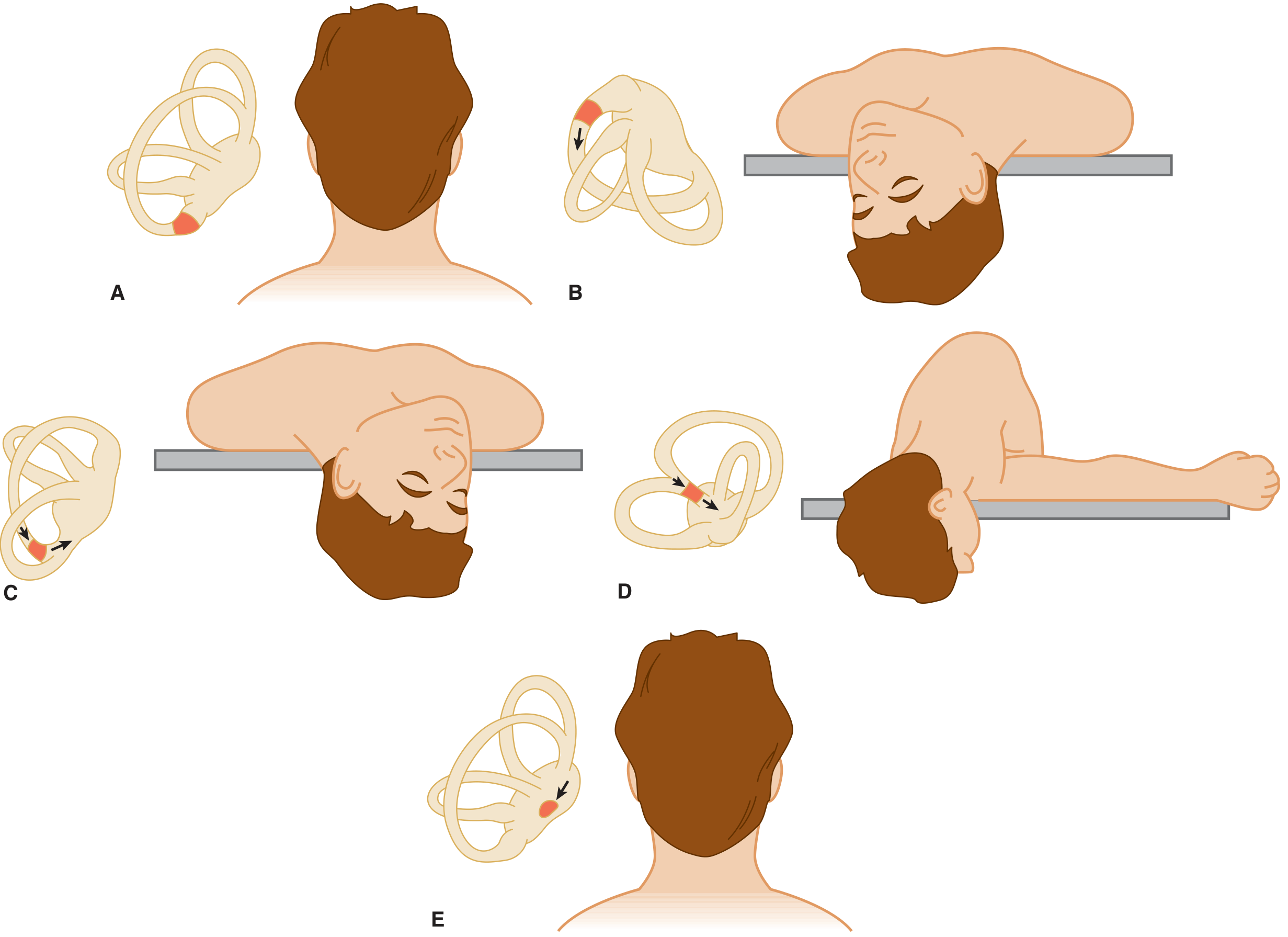
Dix-Hallpike Test (DHT): Gold standard for BPPV
- Positive = upbeat-torsional nystagmus with latency, fatigable → posterior canal BPPV
HINTS Exam (for acute continuous vertigo — to rule out stroke):
- Head Impulse (normal = central), INdirection-changing nystagmus (central), Test of Skew (vertical misalignment = central)
- A normal head impulse + direction-changing nystagmus + skew deviation = posterior circulation stroke (more sensitive than MRI in first 24–48 h)
Step 4: Differential Diagnosis & Management by Cause
A. BPPV (Most Common in Elderly)
- Brief episodes (<1–2 min), triggered by head/position change
- Dix-Hallpike test positive
- Treatment: Epley Maneuver (Canalith Repositioning) — first-line, highly effective
- Do NOT prescribe vestibular suppressants for classic BPPV (episodes too brief)
- Repeat maneuver if needed; instruct home exercises (Brand-Daroff)
B. Vestibular Neuritis
- Constant vertigo lasting days, worse with movement, no hearing loss
- Treatment: Symptomatic (vestibular suppressants short-term), corticosteroids (methylprednisolone) may improve recovery, vestibular rehabilitation exercises
- Avoid prolonged use of suppressants — they impair central compensation
C. Ménière's Disease
- Recurrent episodes (20 min–hours) + low-frequency hearing loss + tinnitus + ear fullness
- Treatment: Low-salt diet, diuretics (hydrochlorothiazide), betahistine; ENT referral
D. Orthostatic Hypotension
- Very common in elderly (medications, dehydration, autonomic dysfunction)
- Treatment: Review/reduce offending medications, adequate hydration, compression stockings, rise slowly, consider fludrocortisone or midodrine if severe
E. Central Vertigo / Posterior Circulation Stroke
- Red flag — must rule out emergently
- Persistent vertigo + any of: new headache, diplopia, dysarthria, ataxia, facial palsy, limb weakness
- Action: Urgent MRI brain (CT may miss posterior fossa infarct), neurological referral
F. Medication-Induced
- Antihypertensives, sedatives, antiepileptics — review and rationalize the medication list
Step 5: Investigations (Selective, Not Routine)
| Test | When to Order |
|---|---|
| BP lying/standing | Orthostatic hypotension suspected |
| ECG / Holter | Arrhythmia suspected |
| Blood tests (FBC, glucose, TFTs, electrolytes) | Non-specific/unexplained dizziness |
| MRI brain | Central signs, HINTS positive, progressive symptoms |
| Audiogram | Unilateral hearing loss, Ménière's suspected |
| Vestibular function tests | Persistent unexplained vertigo |
Routine MRI, audiogram, and vestibular tests are NOT recommended in unselected dizzy patients — they are no more likely to be abnormal than in age-matched controls. — Bradley and Daroff's Neurology in Clinical Practice
Step 6: Pharmacotherapy for Symptomatic Relief
| Drug Class | Example | Dose | Use | Caution in Elderly |
|---|---|---|---|---|
| Antihistamine | Meclizine | 25 mg PO 2–4×/day | Acute vertigo/nausea | Drowsiness, anticholinergic effects |
| Antihistamine | Dimenhydrinate | 50–100 mg PO/IM/IV q4h | Vertigo/nausea | Drowsiness |
| Antiemetic | Metoclopramide | 10 mg IV/PO TDS | Nausea/vomiting | Extrapyramidal effects |
| Antiemetic | Ondansetron | 4 mg IV; 8 mg PO BD | Nausea | Safer option |
| Benzodiazepine | Diazepam | 2–5 mg PO 2–4×/day | Central vertigo/anxiety | Dependency, impairs compensation — avoid if possible in elderly |
| Calcium antagonist | Cinnarizine | 25 mg PO BD | Peripheral vertigo | Lesser experience |
— Tintinalli's Emergency Medicine, Table 170-4
Important: Benzodiazepines and antihistamines with anticholinergic properties should be used with caution and only short-term in elderly patients due to fall risk, sedation, confusion, and urinary retention.
Step 7: Vestibular Rehabilitation
For any chronic or residual vestibular dysfunction:
- Cawthorne-Cooksey exercises or formal vestibular rehabilitation therapy (VRT)
- Proven to improve balance, reduce dizziness, and decrease fall risk
- Particularly important in elderly patients to prevent falls
Summary Algorithm
Dizziness in 80-year-old woman
↓
Characterize: Vertigo / Presyncope / Disequilibrium?
↓
If VERTIGO:
├── Central red flags? → Urgent MRI + Neurology
├── Positional (seconds, Dix-Hallpike +ve)? → Epley Maneuver (BPPV)
├── Constant (days, no hearing loss)? → Vestibular neuritis Rx
├── Episodic (hours + hearing sx)? → Ménière's workup
└── Episodic (minutes) + neuro sx? → TIA workup
↓
If PRESYNCOPE:
├── Orthostatic? → Medication review, hydration
└── Cardiac? → ECG, Holter
↓
Review ALL medications
Vestibular rehabilitation for all chronic cases
Fall risk assessment mandatory
Key take-home points for this patient:
- BPPV is the single most common cause of vertigo in the elderly — always test with Dix-Hallpike
- Never miss posterior circulation stroke — use the HINTS exam
- Orthostatic hypotension and medication side effects are extremely prevalent in this age group
- Avoid or minimize sedating vestibular suppressants in the elderly
- Vestibular rehabilitation reduces fall risk — critical in an 80-year-old
This is a shared conversation. Sign in to Orris to start your own chat.