Tuberculer Meningitis
Reading File
Finding Sources
Searching PubMed
"tuberculous meningitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have comprehensive information from multiple authoritative sources. Let me compile a thorough answer.
Tuberculous Meningitis (TBM)
Overview
Tuberculous meningitis (TBM) is the most severe form of extrapulmonary tuberculosis, caused primarily by Mycobacterium tuberculosis. It carries death rates of 18-40% and leaves disabling neurologic deficits in 10-30% of survivors even with prompt treatment. - Murray & Nadel's Respiratory Medicine
Atypical mycobacteria (M. bovis, M. avium, M. kansasii, M. fortuitum) can also cause TBM, particularly in HIV-infected patients. The frequency of TBM parallels systemic tuberculosis rates, making it especially prevalent in sub-Saharan Africa, South Asia, and among immunocompromised patients.
Pathogenesis
TBM arises in two stages:
- Bacterial seeding of the meninges and subpial regions, forming discrete tubercles (part of miliary dissemination)
- Rupture of one or more tubercles, discharging bacilli into the subarachnoid space
Once in the subarachnoid space, the infection triggers an intense inflammatory cascade that leads to the characteristic complications of the disease.
- Adams & Victor's Principles of Neurology, 12th Ed.
Pathological Findings
-
Basal meningitis: Thick gelatinous exudate accumulates in the pontine and interpeduncular cisterns, extending to the optic chiasm, floor of the third ventricle, undersurfaces of the temporal lobes, and around the medulla
-
Tubercles: Small white discrete lesions scattered over the base of the cerebral hemispheres; microscopically show central caseation surrounded by epithelioid cells, Langhans giant cells, lymphocytes, and plasma cells
-
Vasculitis: Arterial inflammation and occlusion can cause cerebral infarction
-
Hydrocephalus: Blockage of basal cisterns (communicating) or aqueductal obstruction (obstructive)
-
Cranial nerve involvement: The inflammatory exudate engulfs cranial nerves far more often than typical bacterial meningitis
-
The process is truly a meningoencephalitis - the pia and ependyma are penetrated, and the choroid plexus is studded with minute tubercles
-
Adams & Victor's Principles of Neurology, 12th Ed.
MRI in TBM
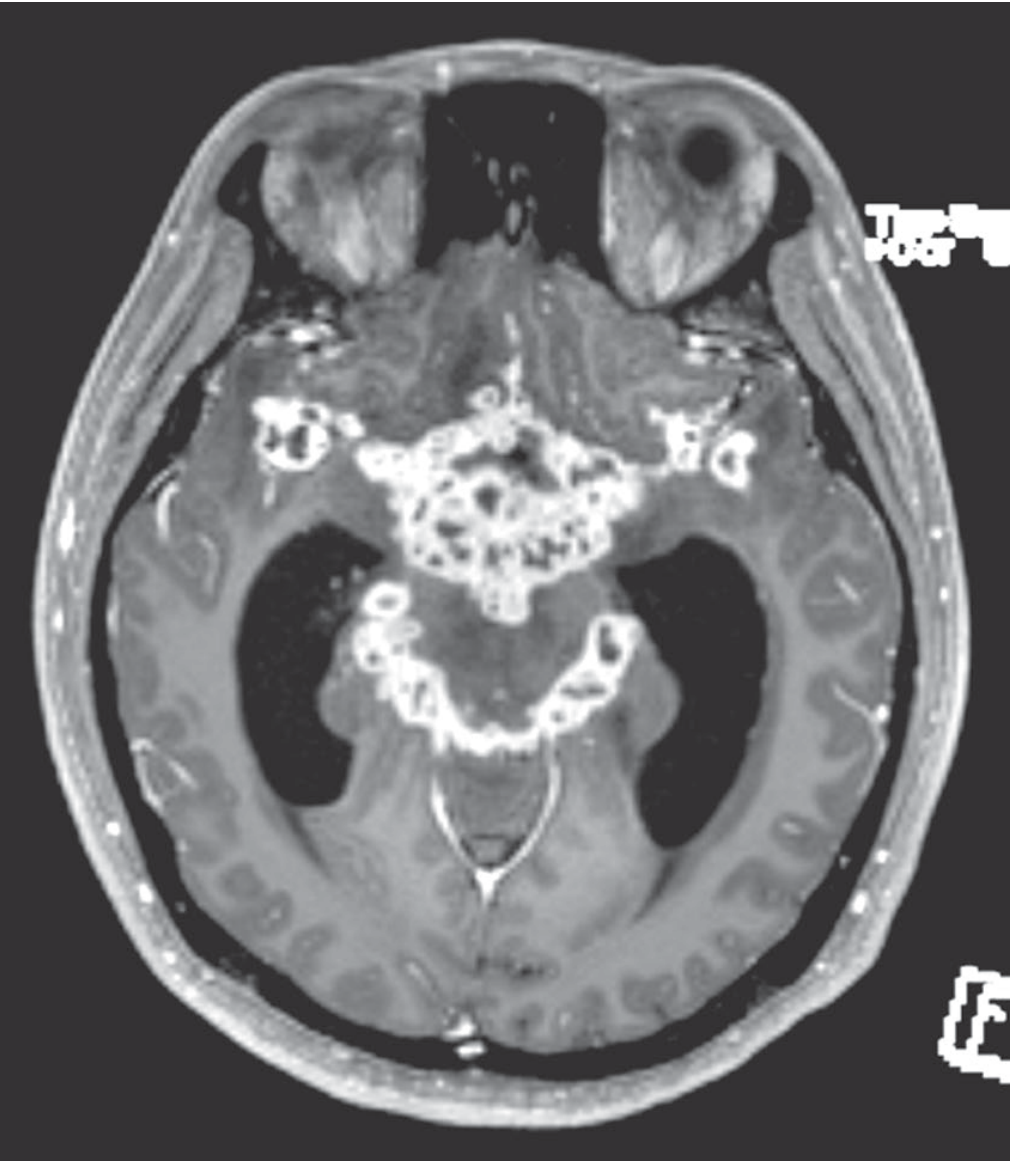
Gadolinium-enhanced MRI in TBM showing intense enhancement of the basal meninges reflecting multiple abscesses, with accompanying hydrocephalus and cranial nerve palsies. - Adams & Victor's Principles of Neurology
Clinical Features
TBM occurs at all ages but is more common in children; adults with HIV or immunocompromise are also at high risk.
Presentation
- Subacute onset over 1-2 weeks (occasionally longer) - in contrast to bacterial meningitis
- Early symptoms: Low-grade fever, malaise, headache (>50% of cases), lethargy, confusion, stiff neck (~75%)
- Kernig and Brudzinski signs present
- Children/infants: Apathy, hyperirritability, vomiting, seizures; neck stiffness may be absent
- Advanced/chronic signs (present at diagnosis in ~20%): Cranial nerve palsies (especially ocular palsies, facial palsy, deafness), papilledema, hypothermia, hyponatremia
- Focal deficits: Can occur from hemorrhagic infarction (due to vasculitis)
- ~2/3 of patients have evidence of active TB elsewhere (lungs, bowel, bone, kidney, ear)
British Medical Research Council Grading
| Grade | Features |
|---|---|
| I | Conscious, no focal deficit |
| II | Confused, or minor focal deficit |
| III | Stuporous, or dense focal deficit |
- Adams & Victor's Principles of Neurology, 12th Ed.; Tintinalli's Emergency Medicine
CSF Findings
| Parameter | Typical TBM Finding |
|---|---|
| Opening pressure | Elevated |
| WBC | 1-500 cells/mm³, predominantly lymphocytes/monocytes |
| Protein | Elevated (often >100 mg/dL) |
| Glucose | Decreased (CSF:serum ratio <0.5); rarely below 20 mg/dL |
| Acid-fast smear | Positive in minority (10-50%+ depending on technique/volume) |
| Culture | May be negative; takes weeks if positive |
- Large volumes of CSF from multiple lumbar punctures with concentration techniques improve sensitivity of both AFB smear and culture
- Plum & Posner's Diagnosis and Treatment of Stupor and Coma; Henry's Clinical Diagnosis
Diagnosis
Key Diagnostic Tests
- AFB smear: Sensitivity 10-50%; low sensitivity but rapid
- Culture (gold standard): Most specific but takes 2-6 weeks; may be negative
- PCR (NAAT): Rapid and specific; sensitivity 25-80% with single primer; multiplex PCR (targeting multiple TB genes) has significantly higher sensitivity
- Adenosine deaminase (ADA): Elevated levels in TBM compared to other meningitides - useful adjunct
- Dot-ELISA for TB antigens/antibodies in CSF: 86% positivity in suspected TBM; only 5% false positives from pyogenic meningitis
Neuroimaging
- CT/MRI: May be normal in ~30% of mild cases
- Classic findings: Basal meningeal enhancement on gadolinium MRI, hydrocephalus, cerebral infarctions, tuberculomas
- Chest CT/X-ray: Evidence of pulmonary TB in ~50% of cases (miliary pattern in some)
Differential Diagnosis
The low/absent CSF pleocytosis may mimic aseptic meningitis - important differentials include:
-
Sarcoidosis
-
Leptomeningeal metastases
-
Neurosyphilis
-
Wegener's granulomatosis (GPA)
-
Behcet's disease
-
Cryptococcal meningitis (especially in HIV)
-
Plum & Posner's; Henry's Clinical Diagnosis
Treatment
Antitubercular Therapy (ATT)
The standard regimen follows a 2-phase approach:
Intensive phase (2 months):
| Drug | Adult Dose |
|---|---|
| Isoniazid (INH) | 300 mg/day |
| Rifampicin (RIF) | 10 mg/kg/day (max 600 mg) |
| Pyrazinamide (PZA) | 30 mg/kg/day in divided doses |
| Ethambutol (EMB) | 15-25 mg/kg/day |
| Pyridoxine (B6) | 50 mg/day (prevents INH neuropathy) |
Continuation phase: INH + RIF for 6-12 months (total therapy 9-12 months)
- If clinical/CSF response is good, PZA can be stopped at 8 weeks; EMB stopped when sensitivity confirmed
- Ethambutol has variable CNS penetration and is questionably adequate for TBM - in children, ethionamide or an aminoglycoside is often substituted (per AAP guidelines)
Pediatric note (AAP): Initial 4-drug regimen with INH, RIF, PZA, and ethionamide or aminoglycoside for 2 months, followed by 7-10 months of INH + RIF.
- Harrison's Principles of Internal Medicine 22E; Murray & Nadel's; Rosen's Emergency Medicine
Adjunctive Corticosteroids
Dexamethasone is strongly recommended for HIV-negative patients - high-quality evidence shows a mortality benefit:
| Population | Dosage |
|---|---|
| Adults (>14 years) | Dexamethasone 0.4 mg/kg/24h with tapering over 6 weeks (Harrison's: 12-16 mg/day x 3 weeks, then taper over 3 weeks) |
| Children (<14 years) | Prednisolone 4 mg/kg/24h (or dexamethasone 0.6 mg/kg/24h) for 4 weeks, then taper over 2-4 weeks |
- Murray & Nadel's; Harrison's 22E
Neurosurgical Interventions
- Ventriculoperitoneal (VP) shunt required in ~25% of patients for hydrocephalus
- Indications: Obstructive hydrocephalus, tuberculous cerebral abscess, paraparesis
- Up to 25% may require some form of neurosurgical procedure in advanced disease
Complications
| Complication | Mechanism |
|---|---|
| Hydrocephalus | Basal cistern obliteration (communicating) or aqueductal block |
| Cerebral infarction/stroke | Vasculitis of penetrating arteries |
| Cranial nerve palsies | Inflammatory exudate around CN III, IV, VI, VII, VIII |
| Paraparesis/spinal syndrome | Exudate around spinal cord, radiculopathy |
| SIADH/hyponatremia | Hypothalamic involvement |
| Seizures | Cortical irritation, infarction |
| Paradoxical reaction | Enlarging tuberculomas during treatment (IRIS) |
| Bladder dysfunction | In ~33% of TBM patients (voiding/storage dysfunction on urodynamics) |
Prognosis
-
Untreated: Death within a few weeks
-
Treated: Mortality 18-40%; neurologic disability in 10-30% of survivors
-
Prognosis depends on: age, comorbidities (HIV), time to diagnosis, disease stage at presentation
-
The severity of illness should always prompt TBM consideration, as early treatment is the critical determinant of outcome
-
Murray & Nadel's; Rosen's Emergency Medicine; Plum & Posner's
Key Sources: Adams & Victor's Principles of Neurology 12th Ed. | Harrison's Principles of Internal Medicine 22E | Murray & Nadel's Textbook of Respiratory Medicine | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Henry's Clinical Diagnosis and Management by Laboratory Methods | Plum & Posner's Diagnosis and Treatment of Stupor and Coma
K/c/o SHTN, DM, CKD 5 on HD , tuberculer Meningitis,military tb, sepsis what treatment should be given antibiotics and further management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching the Web
ATT anti-tuberculosis drug dose adjustment hemodialysis CKD 5 isoniazid ethambutol pyrazinamide rifampicin
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile the full clinical management answer.
Management: TBM + Miliary TB + Sepsis in CKD 5 on Hemodialysis with HTN & DM
This is a high-complexity, multi-problem patient requiring simultaneous management of three overlapping critical conditions. Priorities: stabilize sepsis first → treat TB aggressively → manage comorbidities carefully.
IMMEDIATE PRIORITIES (First Hour - "Sepsis Bundle")
Per Surviving Sepsis Campaign guidelines (SSC):
| Time | Action |
|---|---|
| Within 1 hour | Blood cultures x2 (before antibiotics) |
| Serum lactate | |
| CBC, CMP, LFTs, coagulation | |
| Broad-spectrum IV antibiotics (see below) | |
| IV crystalloid 30 mL/kg if hypotensive or lactate ≥4 mmol/L | |
| Target MAP | ≥65 mmHg |
| Within 6 hours | Vasopressors if MAP not achieved with fluids |
| Reassess volume status, lactate, ScvO2 |
CAUTION IN CKD5/HD: Fluid resuscitation - give 30 mL/kg as per SSC protocol even in dialysis patients (do not withhold), but reassess early with ECHO or passive leg raise. Arrange urgent HD if fluid overload develops post-resuscitation.
- Mulholland's Surgery; Bailey & Love's Surgery
SEPSIS: EMPIRICAL ANTIBIOTICS
The source of sepsis in this patient may be TB bacteremia (miliary TB itself), line infection (dialysis access), secondary bacterial infection, or pneumonia. Cover broadly while cultures are pending.
Empirical Antibiotic Regimen
| Drug | Dose in CKD5/HD | Notes |
|---|---|---|
| Meropenem | 500 mg IV q12h (after HD on HD days) | Preferred carbapenem over imipenem in CNS disease - imipenem is neurotoxic (seizures, myoclonus) especially with underlying CNS disease; dose-reduce in CKD |
| Vancomycin | 1 g IV post-HD session (q3-5 days, guided by levels) | For MRSA/Gram-positive coverage, dialysis access infection; monitor trough - target 15-20 mcg/mL; high-flux HD removes more vancomycin |
- Comprehensive Clinical Nephrology, 7th Ed. (antibiotic dosing in dialysis)
De-escalate as soon as culture sensitivities available. Duration 7-10 days for sepsis (SSC guideline).
Note on CNS penetration: Meropenem has good CSF penetration. Avoid imipenem in TBM patients as it lowers seizure threshold.
ANTI-TUBERCULAR THERAPY (ATT) - DOSE-ADJUSTED FOR HD
Start ATT immediately without waiting for culture confirmation when TBM + miliary TB is clinically suspected.
Standard 4-Drug Regimen Modified for CKD5/HD
| Drug | Normal Dose | Dose in CKD5/HD (eGFR <10, on HD) | Timing relative to HD |
|---|---|---|---|
| Isoniazid (H) | 5 mg/kg/day (max 300 mg) | No dose adjustment - 300 mg daily | Can give anytime; not significantly dialyzable |
| Rifampicin (R) | 10 mg/kg/day (max 600 mg) | No dose adjustment - 600 mg daily | Hepatobiliary excretion; not significantly dialyzable |
| Pyrazinamide (Z) | 25-35 mg/kg/day | 25-30 mg/kg THREE TIMES WEEKLY (give after HD on dialysis days) | Give AFTER HD - significantly removed by HD |
| Ethambutol (E) | 15-25 mg/kg/day | 15-25 mg/kg THREE TIMES WEEKLY (give after HD) | Give AFTER HD - extensively renally cleared; accumulates in CKD |
| Pyridoxine (B6) | 10-25 mg/day | 25-50 mg daily (MANDATORY in CKD+HD) | Any time |
Key rules:
- INH and RIF: full daily doses unchanged - both primarily hepatobiliary; rifampicin is highly protein-bound, lipophilic, and not significantly dialyzed
- EMB: MUST dose-reduce - renally excreted; accumulates → visual toxicity (optic neuritis) if given daily in CKD5. Change to 3x/week and give after HD. Monitor visual acuity and color vision monthly.
- PZA: HD removes pyrazinamide and its metabolite pyrazinoic acid accumulates in renal failure - give after HD, 3x/week
- Give all drugs 4-6 hours before HD or after HD completion to prevent dialytic removal before adequate tissue levels are achieved (applies mainly to EMB and PZA)
- Comprehensive Clinical Nephrology 7th Ed.; Katzung's Pharmacology 16th Ed.; BTS Guidelines (web); Queensland Health TB in Renal Disease Guidelines
Duration of Treatment for TBM
- Intensive phase: 2 months (HRZE)
- Continuation phase: INH + RIF for 7-10 additional months (total 9-12 months for TBM)
- Miliary TB: Treat same duration as TBM (most severe form)
ADJUNCTIVE DEXAMETHASONE
Strongly recommended for TBM (mortality benefit - high-quality RCT evidence).
| Population | Dose | Duration |
|---|---|---|
| Adults | Dexamethasone 0.4 mg/kg/24h IV | Weeks 1-3 (tapered), then reduce; total 6 weeks |
| Alternative (Harrison's) | 12-16 mg/day x 3 weeks, taper over 3 weeks | Total 6 weeks |
IMPORTANT - DM + Dexamethasone interaction:
- Dexamethasone will markedly worsen hyperglycemia in a known diabetic
- Intensify insulin regimen from day 1 of steroids
- Monitor capillary blood glucose every 4-6 hours
- Target glucose: 140-180 mg/dL (ICU range per ADA)
- Use sliding scale insulin + basal insulin (dose adjustment for CKD - insulin clearance also reduced)
- Dexamethasone does NOT require dose adjustment in renal failure
MANAGEMENT OF COMORBIDITIES IN THIS PATIENT
1. CKD 5 on Hemodialysis
- Continue regular HD schedule (typically 3x/week)
- Schedule HD to optimize ATT pharmacokinetics - administer EMB and PZA after each HD session
- Watch for: fluid overload post-sepsis resuscitation → may need extra HD session
- Avoid nephrotoxins strictly: aminoglycosides (streptomycin, kanamycin, amikacin) are CONTRAINDICATED as 4th drug substitute in this patient - will worsen/eliminate residual renal function
- Monitor: BUN, creatinine, potassium, bicarbonate, phosphate at each HD
2. Hypertension
- BP management complicated by:
- Vasopressors for septic shock (norepinephrine first-line)
- Rifampicin induces CYP3A4 - reduces levels of many antihypertensives (CCBs like amlodipine, nifedipine significantly affected)
- May need to increase CCB/ARB doses or switch to drugs with less interaction
- Avoid ACE inhibitors/ARBs in the acute sepsis phase (risk of hypotension and hyperkalemia in CKD5)
- Post-sepsis: amlodipine is less affected by rifampicin than most; dose adjustment may be needed
- Continue HD for fluid management as antihypertensive
3. Diabetes Mellitus
- Dexamethasone: aggressive glucose monitoring and insulin titration (see above)
- Rifampicin may reduce metformin levels (enzyme induction) - however, metformin is CONTRAINDICATED in CKD5 (lactic acidosis risk) - ensure it is stopped
- Insulin clearance is reduced in CKD - risk of hypoglycemia; reduce doses carefully
- Diabetic patients have higher TB risk and worse TBM outcomes - tight glucose control is important
4. Hyponatremia (commonly seen in TBM - SIADH from hypothalamic involvement)
- Check serum sodium urgently
- If SIADH present: fluid restrict to 800-1000 mL/day
- Correct cautiously - no faster than 8-10 mEq/L per 24 hours (risk of osmotic demyelination)
- HD can be used for sodium correction if severe
NEUROSURGICAL CONSIDERATIONS
| Complication | Threshold for Action |
|---|---|
| Hydrocephalus | LP opening pressure >25 cmH2O and progressive symptoms → urgent neurosurgery consult; VP shunt in 25% of TBM patients |
| Cerebral infarction | MRI/DWI to detect lacunar infarcts from vasculitis |
| Raised ICP | Head of bed 30°, avoid hyponatremia, dexamethasone helps |
| Seizures | Start antiepileptic if seizures occur (levetiracetam preferred in CKD - less hepatic interaction with rifampicin vs phenytoin) |
MONITORING PROTOCOL
| Parameter | Frequency | Why |
|---|---|---|
| Visual acuity + color vision | Monthly | Ethambutol optic neuritis - early detection critical |
| LFTs (AST, ALT, bilirubin) | Baseline, 2-weekly | ATT hepatotoxicity (INH, RIF, PZA all hepatotoxic) |
| Serum uric acid | Monthly | PZA-induced hyperuricemia - may worsen gout in HD |
| CBC | 2-weekly | Bone marrow toxicity; rifampicin thrombocytopenia |
| Blood glucose (CBG) | Every 4-6h (ICU) | Dexamethasone hyperglycemia |
| Serum Na, K | Each HD | Electrolytes, SIADH |
| Vancomycin levels | Post-HD | Target trough 15-20 mcg/mL |
| Neurological exam | Daily | Cranial nerve palsies, consciousness level, meningism |
| CSF (LP) | As clinically indicated | Monitor response to therapy |
| Blood cultures | Repeat at 48-72h | Clear bacteremia |
DRUGS TO AVOID / USE CAUTION
| Drug | Reason to Avoid/Caution |
|---|---|
| Imipenem | CNS neurotoxicity (seizures, myoclonus) in TBM + CKD |
| Aminoglycosides (streptomycin, amikacin) | Nephrotoxic + ototoxic; contraindicated in CKD5 |
| Standard-dose Ethambutol daily | Accumulates → irreversible optic neuropathy in renal failure |
| Metformin | Contraindicated in CKD5 (lactic acidosis) |
| NSAIDs | Worsen residual renal function, raise BP |
| Daily standard-dose PZA | Pyrazinoic acid accumulates in HD - use 3x/week post-HD |
| Phenytoin | Rifampicin induces CYP450 → subtherapeutic phenytoin; multiple interactions; prefer levetiracetam |
| Fluoroquinolones (ciprofloxacin, ofloxacin) | Require dose reduction in CKD (GFR<30); moxifloxacin does not require dose reduction and is an alternative 4th drug if EMB cannot be used |
SUMMARY TREATMENT PLAN AT A GLANCE
SEPSIS:
→ Meropenem 500 mg IV q12h (after HD)
→ Vancomycin 1 g IV post-HD (level-guided)
→ Norepinephrine if MAP <65 despite 30 mL/kg crystalloid
→ Blood cultures × 2, lactate, CBC, LFT before antibiotics
→ De-escalate at 48-72h based on cultures
TBM + MILIARY TB:
→ INH 300 mg oral daily (no change)
→ Rifampicin 600 mg oral daily (no change)
→ Pyrazinamide 25-30 mg/kg oral 3×/week AFTER HD
→ Ethambutol 15-25 mg/kg oral 3×/week AFTER HD
→ Pyridoxine (B6) 25-50 mg oral daily (mandatory)
→ Dexamethasone 0.4 mg/kg/day IV (taper over 6 weeks)
Total duration: 9-12 months
COMORBIDITIES:
→ Continue HD schedule; add sessions if fluid-overloaded
→ Intensify insulin for dexamethasone-induced hyperglycemia
→ Stop metformin (already contraindicated in CKD5)
→ Adjust antihypertensives (rifampicin lowers levels of CCBs)
→ Monitor eyes monthly (EMB), LFTs 2-weekly, electrolytes each HD
→ Neurosurgery consult for hydrocephalus monitoring
Sources: Comprehensive Clinical Nephrology 7th Ed. | Harrison's Principles of Internal Medicine 22E | Katzung's Basic & Clinical Pharmacology 16th Ed. | Murray & Nadel's Textbook of Respiratory Medicine | Mulholland & Greenfield's Surgery | BTS Guidelines for TB in CKD | Queensland Health TB-Renal Guidelines | PMC Literature (PMID-referenced web sources)
And GCS 4 E4 VTM1
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.