Tomorrow is my presentation on periodontal disease . Provide me concept on this along with figure . From standard books of dental
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive content and figures from multiple standard textbooks. Let me compile a thorough, well-illustrated presentation on periodontal disease.
🦷 Periodontal Disease - Complete Presentation Guide
Sources: Robbins & Cotran Pathologic Basis of Disease (10e), Junqueira's Basic Histology (17e), Sherris & Ryan's Medical Microbiology (8e), Goldman-Cecil Medicine, Scott-Brown's Otorhinolaryngology, Park's Preventive & Social Medicine, Rosen's Emergency Medicine
1. DEFINITION & OVERVIEW
Periodontal disease refers to a group of oral infections affecting the periodontium - the hard and soft tissues that support and maintain teeth in the jaws. It is the most common cause of tooth loss worldwide and was ranked the 11th most prevalent disease globally (2016).
"Periodontal diseases are a group of oral infections that affect the periodontium... A worldwide problem, it is the most common cause of tooth loss."
- Goldman-Cecil Medicine, International Edition
2. THE NORMAL PERIODONTIUM (Anatomy Foundation)
The periodontium comprises four structures:
| Structure | Description |
|---|---|
| Gingiva | Keratinized mucosa; free gingival (FG) overlies the tooth neck |
| Cementum | Covers dentin of root; avascular; bone-like; maintained by cementocytes |
| Periodontal Ligament (PDL) | Collagen (Sharpey) fibers binding cementum to alveolar bone; 150-350 μm thick; highly vascular and innervated |
| Alveolar Bone | Supports tooth sockets; continuously remodeled by osteoblasts/osteocytes |
Fig. 15-11 - Normal Periodontium (Junqueira's Basic Histology, 17e):
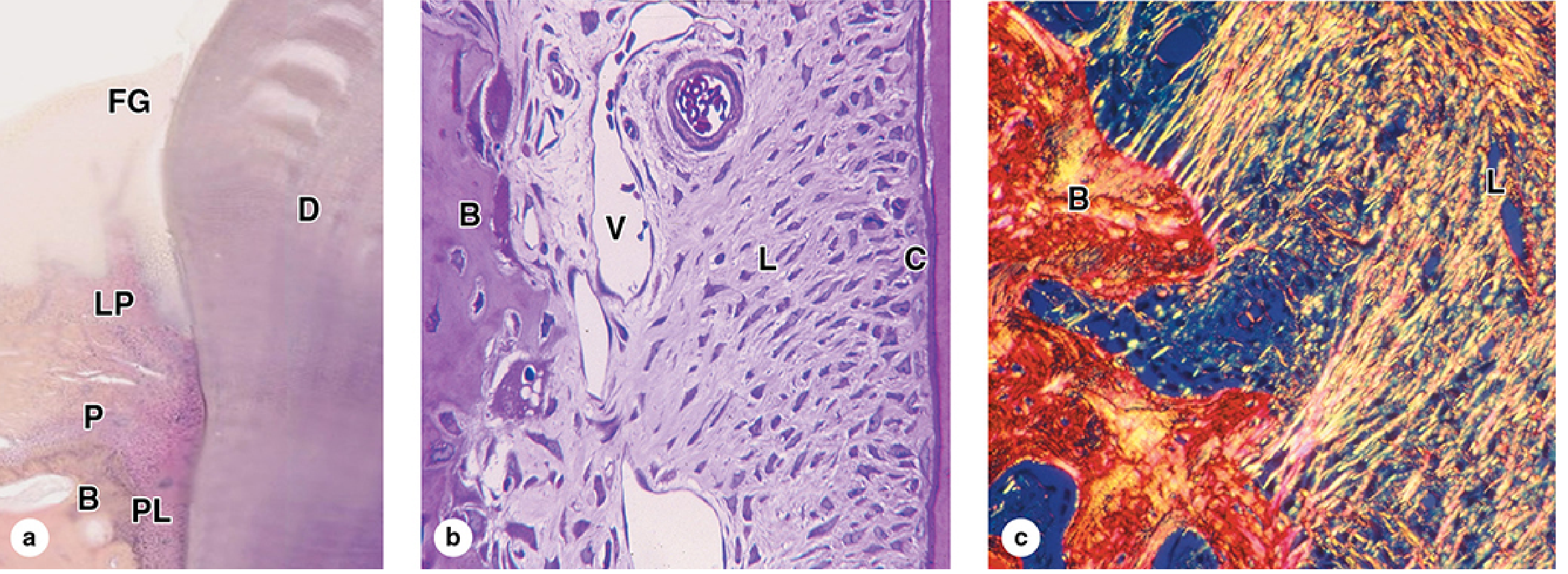
(a) Low-power H&E: Free gingiva (FG) over dentin (D), lamina propria (LP) continuous with periosteum (P) of alveolar bone (B), and PDL (PL). (b) The PDL (L) with abundant blood vessels (V) inserting into alveolar bone (B); cementum (C) is thin and bone-like. (c) Picrosirius/polarized light: collagen continuity from alveolar bone (B) periosteum into PDL (L).
3. ETIOLOGY & PATHOGENESIS
The Central Role of Dental Plaque
- Dental plaque is a sticky, colorless biofilm containing bacteria, salivary proteins, and desquamated epithelial cells
- Forms above (supragingival) and below (subgingival) the gingival margin
- If not removed, mineralizes into calculus (tartar)
- Subgingival plaque within the gingival crevice/sulcus is the primary etiologic agent
Microbial Shift in Disease
| Healthy Sites | Active Periodontitis |
|---|---|
| Facultative gram-positive organisms | Anaerobic & microaerophilic gram-negative flora |
Key Pathogens (from 300 oral species)
- Aggregatibacter (Actinobacillus) actinomycetemcomitans - produces leukotoxin; key in aggressive/juvenile periodontitis
- Porphyromonas gingivalis - key virulence factors; synergy with Treponema
- Prevotella intermedia
- Treponema denticola - cross-feeds with P. gingivalis; drives gingivitis → periodontitis progression
"Synergism between P. gingivalis, T. denticola, and other plaque members is felt to foster progression of gingivitis to chronic periodontitis."
- Sherris & Ryan's Medical Microbiology, 8e
Risk Factors
- Local: Poor oral hygiene, tobacco use, dental malocclusion
- Systemic: Diabetes mellitus (bidirectional relationship), HIV/AIDS, Down syndrome, Crohn's disease, sarcoidosis, neutrophil deficiency/dysfunction, pregnancy
- Genetic: Altered microbiome composition
4. CLASSIFICATION & STAGES
Stage 1 - GINGIVITIS (Reversible)
Definition: Inflammation limited to the marginal gingiva; no bone resorption.
Features:
- Develops within 2 weeks of cessation of effective oral hygiene
- Erythema, edema, bleeding on probing, contour changes
- Loss of soft tissue support without bone loss
- Fully reversible with oral hygiene restoration
"Gingivitis is inflammation of the oral mucosa surrounding the teeth, caused by accumulation of dental plaque and calculus... Fortunately, it is reversible."
- Robbins & Cotran Pathologic Basis of Disease, 10e
Histopathology of Gingivitis:
- Marked inflammatory infiltrate of PMNs, lymphocytes, and plasma cells in connective tissue adjacent to crevicular epithelium
- Collagen loss from inflamed connective tissue
- No direct bacterial invasion in early stages
Stage 2 - PERIODONTITIS (Irreversible)
Definition: Extension of inflammation to supporting structures - PDL, alveolar bone, cementum.
Key Events in Progression:
- Supragingival → subgingival plaque accumulation
- Deepening of gingival sulcus via apical migration of gingival attachment
- Loss of connective tissue attachment
- Alveolar bone resorption → periodontal pocket formation
- Loosening → eventual tooth loss
"Periodontitis is not considered to be a reversible disease in that the lost alveolar bone and periodontal ligament do not regenerate with cessation of inflammation, even though further progression may be halted."
- Sherris & Ryan's Medical Microbiology, 8e
Clinical Parameters Assessed:
- Pocket depth (periodontal probe in gingival sulcus)
- Bleeding on probing = active gingival inflammation
- Attachment loss
- Tooth mobility
5. CLINICAL PHOTOGRAPHS
Fig. 41-5 - Normal vs. Periodontal Disease (Sherris & Ryan's Medical Microbiology, 8e):
A. Normal Gingiva - Pink, firm, well-adapted to teeth, no bleeding:

B. Periodontal Disease - Plaque, severe inflammation, bleeding, gingival recession with root exposure ("teeth look longer"):

Fig. 42.1 - Chronic Periodontitis (Scott-Brown's Otorhinolaryngology, Head & Neck Surgery):

6. TYPES OF PERIODONTITIS
| Type | Age Group | Key Feature |
|---|---|---|
| Chronic Periodontitis | >35-40 years | Slow progressive destruction; most common cause of adult tooth loss |
| Localized Aggressive Periodontitis | Adolescents | Rapid bone loss; associated with A. actinomycetemcomitans leukotoxin |
| Generalized Aggressive Periodontitis | Young adults | Rapid widespread destruction |
| Necrotizing Periodontal Disease | Immunocompromised | HIV+, poorly controlled diabetes; requires debridement |
| Periodontal Abscess | Any | Acute exacerbation when pocket neck becomes constricted; requires drainage |
7. CAUSES OF GINGIVAL BLEEDING
(Scott-Brown's Table 42.2)
| Local Causes | Systemic Causes |
|---|---|
| Chronic gingivitis | Pregnancy (exacerbates gingivitis) |
| Chronic periodontitis | Leukaemia |
| Acute necrotizing gingivitis | HIV infection |
| Angioma/telangiectasia | Clotting defects |
| Anticoagulant drugs | |
| Scurvy (Vitamin C deficiency) |
8. SYSTEMIC ASSOCIATIONS
Periodontal disease is associated with multiple systemic conditions. When localized to the gums, it is linked to:
- Diabetes mellitus (bidirectional - each worsens the other)
- Atherosclerotic vascular disease (significant research exists; periodontitis is a source of bacteremia)
- Infective endocarditis (periodontal bacteria may seed cardiac valves)
- Brain and lung abscesses (hematogenous spread)
- AIDS/HIV
- Down syndrome, Crohn disease, sarcoidosis
Note: Despite ongoing concerns, Goldman-Cecil Medicine states there is currently "no evidence that periodontal disease is an independent risk factor for coronary artery disease."
9. GLOBAL BURDEN (Park's Preventive & Social Medicine)
- Severe periodontal disease was the 11th most prevalent disease globally in 2016
- Major causes: poor oral hygiene and tobacco use
- Dental caries + periodontal disease = leading causes of tooth loss
- Severe tooth loss ranked among top 10 causes of years lived with disability (YLD) in high-income countries with aging populations
10. MANAGEMENT
Non-Surgical (Mainstay)
| Treatment | Notes |
|---|---|
| Oral hygiene | Twice-daily brushing + flossing |
| Scaling & root planing | Removal of subgingival calculus and biofilm (gold standard) |
| Chlorhexidine rinse | 0.12%-0.2% preferred; antibacterial mouthwash for moderate/severe cases |
| 3% H₂O₂ | Diluted 1:1 warm water; alternative rinse |
| Smoking cessation | Most important risk factor modification in HIV-negative patients |
Analgesia
- Ibuprofen 400-600 mg every 6-8 hours, OR
- Acetaminophen 650 mg every 6 hours
- Topical: Viscous lidocaine (applied to small areas only)
Antibiotics (for severe/spreading disease, systemic symptoms, or immunocompromise)
(Rosen's Emergency Medicine, Table 56.2)
| Antibiotic | Dose | Duration |
|---|---|---|
| Penicillin V | 500 mg TID-QID | 10 days |
| Amoxicillin/clavulanate | 500/125 mg TID | 10 days |
| Metronidazole | 500 mg BID (PCN allergy) | 10 days |
| Clindamycin | 300 mg QID (PCN allergy) | 10 days |
| Nystatin | 100,000 U/mL swish/spit QID (immunocompromised) | 10 days |
(Goldman-Cecil first-line: Amoxicillin 250 mg TID × 3 days; alternative: Clindamycin 150 mg QID × 3 days)
Surgical
- Debridement of necrotic tissue (necrotizing disease)
- Periodontal abscess: drainage essential
- Referral to dentist for all cases
11. PREVENTION
- Regular oral hygiene (brushing ×2/day, flossing)
- Regular dental check-ups and professional scaling
- Smoking cessation
- Control of systemic risk factors (glycemic control in diabetics)
- Community water fluoridation (reduces caries which can co-contribute)
SUMMARY FLOW CHART
DENTAL PLAQUE/CALCULUS (poor hygiene, smoking, systemic risk factors)
↓
GINGIVITIS
(Reversible - inflammation of marginal gingiva only)
↓ (if unchecked - subgingival plaque, gram-negative anaerobes)
PERIODONTITIS
(Irreversible - PDL destruction + alveolar bone loss + pocket formation)
↓
TOOTH LOOSENING → TOOTH LOSS / PERIODONTAL ABSCESS
Key Textbooks Referenced:
- Robbins & Cotran Pathologic Basis of Disease, 10e - Gingivitis & Periodontitis, p. 493-500
- Junqueira's Basic Histology, 17e - Periodontium, Fig. 15-11
- Sherris & Ryan's Medical Microbiology, 8e - Chronic Periodontitis, Fig. 41-5
- Goldman-Cecil Medicine, International Ed. - Periodontal Disease section
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Fig. 42.1, Table 42.2
- Park's Textbook of Preventive & Social Medicine - Global burden data
- Rosen's Emergency Medicine - Management Table 56.2
Good luck with your presentation tomorrow!
This is a shared conversation. Sign in to Orris to start your own chat.