Physiological effect of Growth Hormone
Reading File
Finding Sources
Finding Sources
Searching PubMed
"growth hormone" AND physiology
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I have comprehensive content from multiple authoritative textbooks. Now I can compile a thorough, well-structured answer.
Physiological Effects of Growth Hormone (GH)
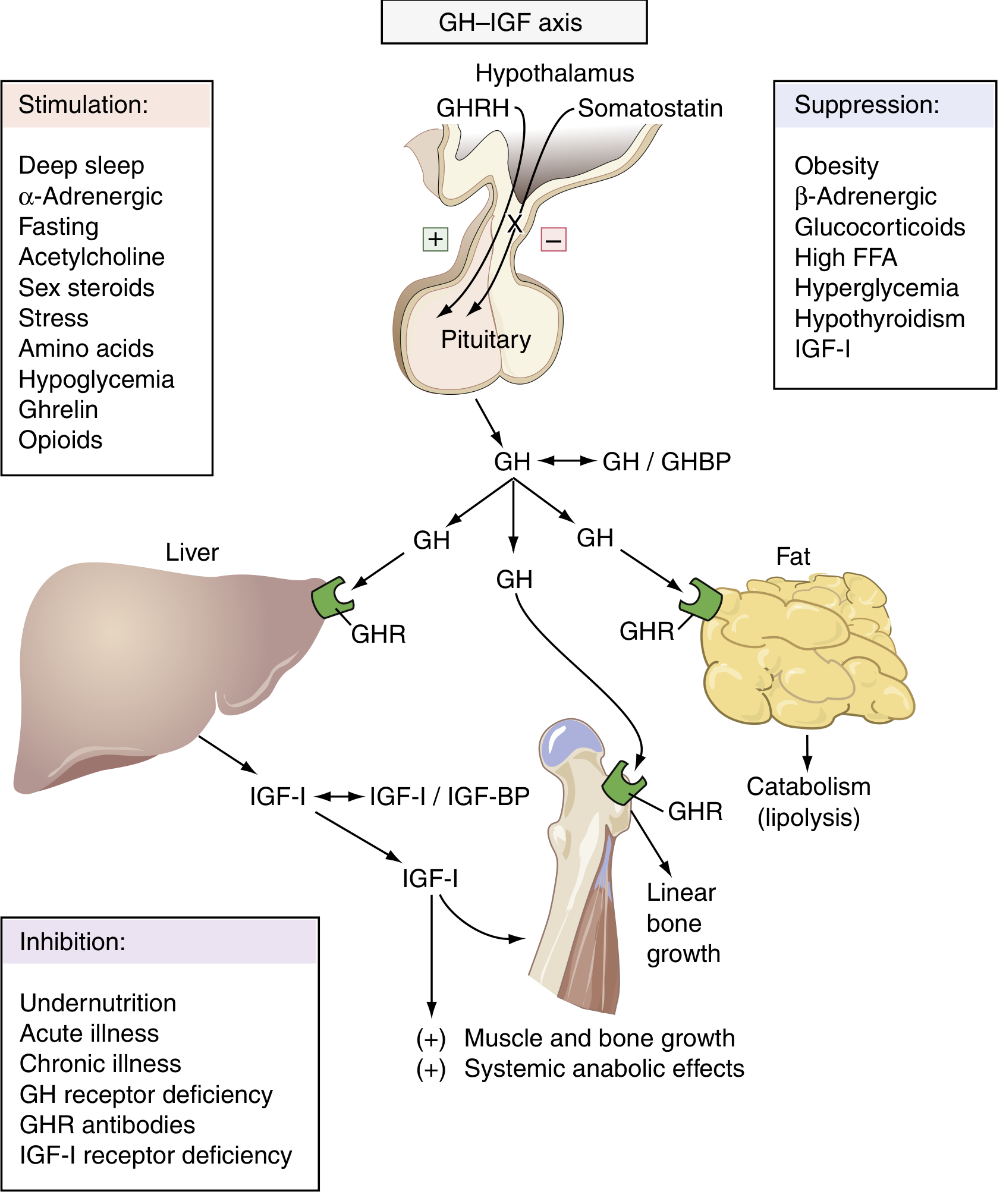
The GH-IGF axis: stimulatory and suppressive inputs to the pituitary, and downstream effects on target tissues via direct GH signaling and IGF-1. (Henry's Clinical Diagnosis & Management by Laboratory Methods)
1. Chemistry and Source
Growth hormone (GH, somatotropin) is a 191-amino acid single-chain polypeptide with two internal disulfide bridges, secreted by somatotrophs of the anterior pituitary. It is structurally homologous to prolactin (75% homology) and human placental lactogen (80% homology). GH is the single most important hormone for normal growth to adult stature and exerts broad metabolic effects throughout life. - Costanzo Physiology 7th Edition
2. Regulation of Secretion
GH is secreted in a pulsatile pattern (~every 2 hours), with the largest burst occurring 1 hour after onset of deep sleep (stages III/IV). Up to 70% of daily GH secretion occurs during slow-wave sleep. Secretory rates peak at puberty (driven by estrogen and testosterone) and decline progressively with senescence. - Costanzo Physiology, Henry's Clinical Diagnosis
Two hypothalamic hormones act in opposition:
- GHRH (growth hormone-releasing hormone): stimulates GH release by raising cAMP and Ca²⁺ in somatotrophs
- Somatostatin (SS): inhibits adenylyl cyclase, lowers Ca²⁺, suppresses GH release
A third regulator, ghrelin (28-amino acid peptide from gastric neuroendocrine cells), binds GH secretagogue receptor 1a (GHSR1a) and potently stimulates GH secretion, particularly in the fasted state. - Medical Physiology (Boron & Boulpaep)
Factors Affecting GH Secretion
| Stimulatory | Inhibitory |
|---|---|
| Hypoglycemia, fasting, starvation | Hyperglycemia, high FFA |
| Stage III/IV sleep | Obesity, senescence |
| Exercise, stress | Somatostatin |
| Sex steroids (puberty) | IGF-1 (negative feedback) |
| Arginine, amino acids | Beta-adrenergic agonists |
| Alpha-adrenergic agonists | Glucocorticoids |
| Ghrelin, opioids | Hypothyroidism |
- Costanzo Physiology, Goodman & Gilman's
3. Mechanism of Action: Direct vs. IGF-1 Mediated
GH acts via two routes:
A. Direct effects - GH binds to GH receptors (GHR), which are tyrosine kinase-associated receptors (JAK2-STAT signaling). These primarily affect carbohydrate and fat metabolism.
B. Indirect effects via IGF-1 - GH stimulates the liver (primarily) to produce IGF-1 (somatomedin C), which circulates bound to IGF-binding proteins (mainly IGF-BP3). Free IGF-1 acts on target tissues via receptors with intrinsic tyrosine kinase activity (structurally similar to the insulin receptor). The growth-promoting effects of GH (bone, muscle, organs) are largely IGF-1 mediated. - Costanzo Physiology, Henry's Clinical Diagnosis
IGF-1 also provides negative feedback to the pituitary and hypothalamus to suppress GH secretion.
4. Effects on Linear Growth (Skeletal)
This is the most dramatic and well-known effect. GH, acting through IGF-1, stimulates:
- DNA synthesis, RNA synthesis, and protein synthesis in chondrocytes
- Widening of epiphyseal growth plates in long bones
- Increased cartilage metabolism and chondrocyte proliferation
- Deposition of new bone at the ends of long bones
When GH excess occurs before puberty (before epiphyseal plate closure) → gigantism
When GH deficiency occurs in childhood → pituitary dwarfism
When GH excess occurs after puberty (plates fused) → acromegaly (periosteal thickening, enlargement of hands/feet/tongue/facial features, organomegaly) - Costanzo Physiology, Medical Physiology
5. Effects on Protein Metabolism (Anabolic)
GH is a potent anabolic agent for protein:
- Increases amino acid uptake into cells
- Stimulates synthesis of DNA, RNA, and protein in virtually all organs
- Decreases protein catabolism - by mobilizing free fatty acids for energy, GH spares protein from being used as fuel (a "protein-sparing" or anti-catabolic effect)
- Net result: increased lean body mass and increased organ size
These effects can begin within minutes. GH replacement in adults with GH deficiency increases lean body mass and decreases body fat. - Guyton & Hall, Medical Physiology
6. Effects on Fat Metabolism (Lipolytic)
GH stimulates lipolysis in adipose tissue:
- Releases free fatty acids (FFA) into the circulation
- Enhances conversion of fatty acids to acetyl-CoA for energy utilization in peripheral tissues
- Fat is preferentially used for energy over carbohydrates and protein
In excess GH: extensive fat mobilization can cause ketogenesis (formation of acetoacetic acid by the liver) and fatty liver. - Guyton & Hall
7. Effects on Carbohydrate Metabolism (Diabetogenic)
GH has a counter-insulin / diabetogenic action:
- Decreases glucose uptake by skeletal muscle and adipose tissue (insulin resistance)
- Increases hepatic gluconeogenesis (inhibits insulin's suppression of liver glucose production)
- Net effect: raised blood glucose and compensatory increased insulin secretion
The mechanism involves GH-induced lipolysis raising FFA levels, which in turn impair insulin signaling in liver and skeletal muscle. - Guyton & Hall, Costanzo Physiology
This is why:
- Excess GH (acromegaly) can cause glucose intolerance resembling type 2 diabetes
- Deficient GH in adults reduces gluconeogenic capacity
- Permissive amounts of GH (along with cortisol) are required for normal counter-regulatory response to hypoglycemia - Goldman-Cecil Medicine
8. Effects on Bone Mineral Metabolism
IGF-1 generated under GH influence stimulates protein synthesis in bone. GH also promotes calcium retention and increases renal reabsorption of phosphate. Excessive GH can contribute to hypercalciuria. - Ganong's Review of Medical Physiology
9. Effects on Other Organ Systems
| System | Effect |
|---|---|
| Muscle | Increased protein synthesis, increased lean mass |
| Liver | IGF-1 production, protein synthesis, glycogenesis (via IGF-1) |
| Kidneys | Increased size; contributes to phosphate reabsorption |
| Heart | Increased cardiac muscle mass; GH receptors present on cardiomyocytes |
| Immune system | Promotes immune responses (estrogen and GH enhance immune activity, vs. glucocorticoids which suppress) |
| Skin, connective tissue | Thickening in acromegaly |
| GI tract | Organomegaly in acromegaly |
| CNS | GH and IGF-1 receptors present; roles in neuroprotection and cognition under investigation |
10. GH Deficiency vs. Excess: Clinical Correlates
| Condition | Timing | Features |
|---|---|---|
| Pituitary dwarfism | Childhood | Normal birth size, growth failure, short stature, mild obesity, delayed puberty |
| Laron dwarfism | Childhood | Elevated GH, defective GH receptor → no IGF-1 generation; GH treatment ineffective |
| Gigantism | Pre-pubertal excess | Extreme linear growth (>2.7 m possible) |
| Acromegaly | Post-pubertal excess | Periosteal bone thickening, enlarged hands/feet, coarse facial features, organomegaly, insulin resistance, hypertension, heart failure if untreated |
| Adult GH deficiency | Adulthood | Decreased lean mass, increased body fat, possible reduced well-being |
- Medical Physiology, Costanzo Physiology
Summary
GH is a multi-system hormone with effects that can be organized as:
- Growth (via IGF-1): linear bone growth, organ size, lean mass
- Protein metabolism: anabolic - increases synthesis, decreases catabolism
- Fat metabolism: lipolytic - mobilizes FFA, promotes fat as fuel
- Carbohydrate metabolism: diabetogenic - raises blood glucose, causes insulin resistance
- Counter-regulatory: permissive role in response to hypoglycemia
Its net metabolic "purpose" is to redirect substrates toward growth and tissue building, particularly during periods of physiological demand (sleep, puberty, stress, fasting).
Sources: Costanzo Physiology 7th Ed. | Guyton & Hall Textbook of Medical Physiology | Medical Physiology (Boron & Boulpaep) | Henry's Clinical Diagnosis & Management | Goldman-Cecil Medicine | Ganong's Review of Medical Physiology | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.