Assignment on hepatitis for microbiology MBBS including all types and lab diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have enough comprehensive content from the authoritative medical microbiology textbooks to write a thorough, well-structured assignment. Let me compose it now.
Viral Hepatitis: A Comprehensive Assignment for MBBS Microbiology
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology 28th Edition; Sherris & Ryan's Medical Microbiology 8th Edition; Tietz Textbook of Laboratory Medicine 7th Edition; Harrison's Principles of Internal Medicine 22nd Edition
1. INTRODUCTION
Viral hepatitis is a systemic infection primarily involving the liver, caused by a group of hepatotropic viruses. At least five distinct viruses are responsible for the majority of cases: Hepatitis A (HAV), B (HBV), C (HCV), D (HDV), and E (HEV). Each belongs to a different virus family, with different modes of transmission, clinical course, and outcomes. Together they represent a major global health burden, causing acute and chronic liver disease, cirrhosis, and hepatocellular carcinoma (HCC).
Other viruses that can cause incidental hepatitis include Epstein-Barr virus (EBV), cytomegalovirus (CMV), herpes simplex virus (HSV), yellow fever virus, and rubella virus - but these are not primary hepatitis viruses. A sixth agent, hepatitis G virus (HGV/GBV-C), has been identified in blood donors and patients co-infected with HCV or HIV, but is not associated with clinical liver disease.
"The causes of hepatitis (inflammation of the liver) are varied and include viruses, bacteria, and protozoa, as well as drugs and toxins. The clinical symptoms and course of acute viral hepatitis can be similar, regardless of etiology, and determination of a specific cause depends primarily on the use of laboratory tests." - Sherris & Ryan's Medical Microbiology
2. COMPARISON TABLE OF HEPATITIS VIRUSES
(Based on Sherris & Ryan's Medical Microbiology, Table 13-1)
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Virus type | ssRNA (+) | dsDNA (partial) | ssRNA (+) | ssRNA (-) | ssRNA (+) |
| Family | Picornaviridae | Hepadnaviridae | Flaviviridae | Deltaviridae | Hepeviridae |
| Size | 27-32 nm | 42 nm (Dane) | 50-60 nm | 35-37 nm | 27-34 nm |
| Envelope | No | Yes | Yes | Yes (from HBV) | No |
| Incubation (weeks) | 15-45 (mean 25) | 60-150 (mean 90) | 14-182 (mean 42) | 21-49 | 15-60 (mean 40) |
| Onset | Sudden | Gradual | Insidious | Variable | Variable |
| Fecal-oral | +++ | ± | - | ± | +++ |
| Parenteral | - | +++ | +++ | ++ | - |
| Sexual | + | ++ | + | ++ | +? |
| Vertical (mother-child) | Rare | +++ | + | + | Rare |
| Carrier state | None | Yes | Yes | Yes | No |
| Chronicity | None | ~10% (adults), ~90% (neonates) | 80-85% | 50-80% | Rare (except in pregnancy) |
| Fulminant hepatitis | Rare (<0.1%) | <1% | Rare | Up to 20% (coinfection) | 20-25% in pregnancy |
| HCC risk | None | High | High | High | None |
| Vaccine available | Yes | Yes | No | Prevented by HBV vaccine | Yes (some countries) |
3. HEPATITIS A (HAV)
3.1 Virology
- Family: Picornaviridae, Genus: Hepatovirus
- 27-32 nm, non-enveloped, icosahedral, positive-sense single-stranded RNA (7.5 kb)
- Single serotype - no antigenic cross-reactivity with other hepatitis viruses
- 7 genotypes based on the 1D/2A gene junction sequence
- Resistant to acid (pH 1 for 2 hours), ether (20%), and heat (60°C for 1 hour)
- Destroyed by: autoclaving (121°C/20 min), boiling (5 min), dry heat (180°C/1 hr), UV irradiation, formalin, chlorine (10-15 ppm/30 min)
- Does not grow easily in cell culture (no cytopathic effects); primate cell lines used
3.2 Epidemiology
- Fecal-oral route is the primary mode of transmission (contaminated water/food)
- Common in developing countries with poor sanitation
- Affects older children and young adults preferentially
- Shellfish from sewage-contaminated waters, raw vegetables/fruits, waterborne outbreaks
- Highly contagious - can spread by person-to-person contact
3.3 Pathogenesis
- Ingested virus replicates in the GI tract
- Spreads to the liver via bloodstream (viremia)
- Immune-mediated liver cell destruction by CD8+ CTLs
- HAV itself is not directly cytotoxic
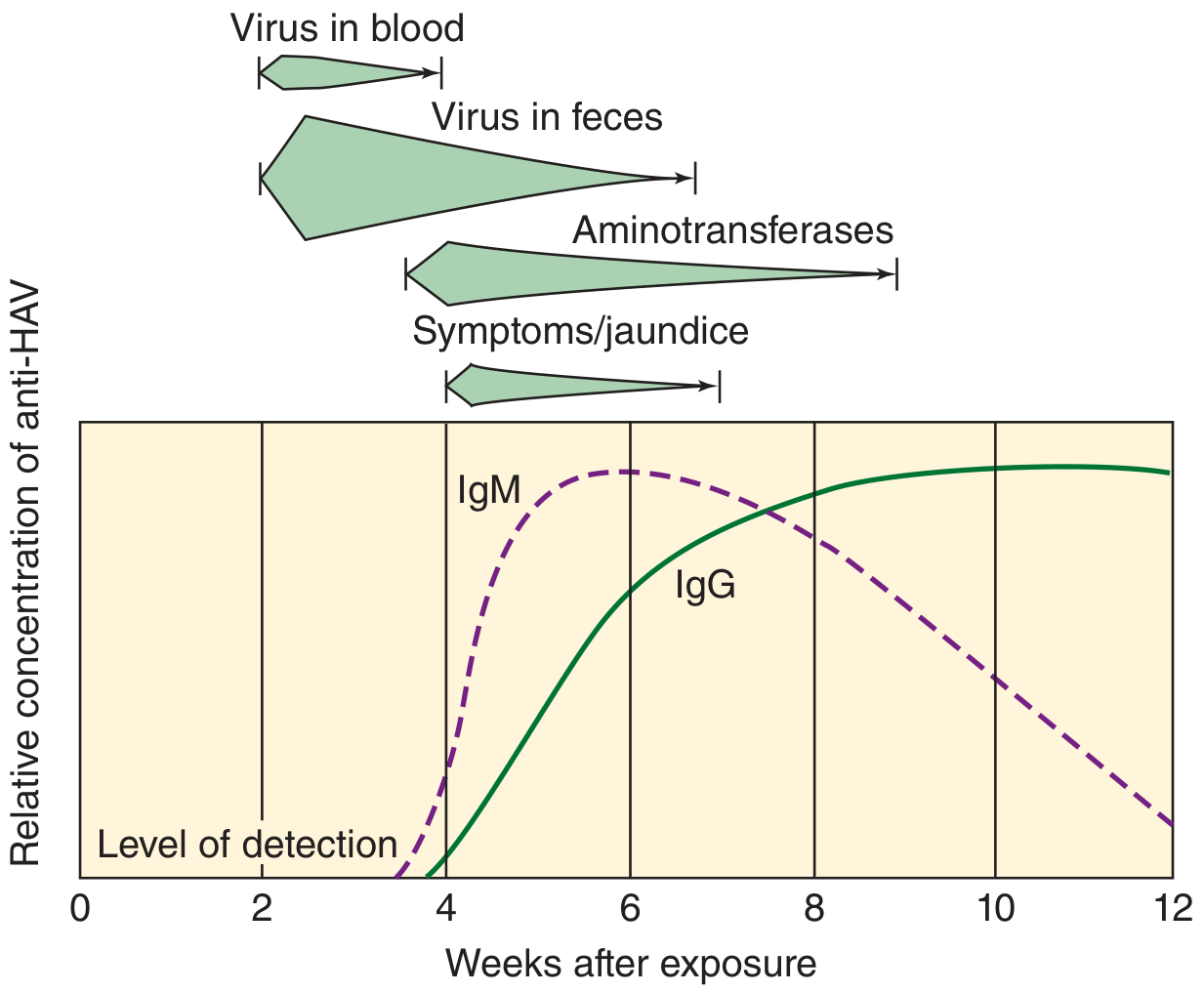
- Peak fecal shedding occurs 2 weeks before jaundice onset (before the patient is symptomatic - key epidemiological concern)
3.4 Clinical Features
- Incubation period: 15-45 days (mean 25 days)
- Prodromal phase (3-10 days): fever, malaise, anorexia, nausea, vomiting, right upper quadrant discomfort
- Icteric phase: jaundice, dark urine (bilirubinuria), pale stools, pruritus, hepatomegaly, elevated liver enzymes
- Self-limiting in nearly all patients; recovery within 3-6 months
- Fulminant hepatitis: rare (<0.1%)
- No chronicity, no carrier state
- Anicteric infection is common, especially in children
3.5 Lab Diagnosis
Serology (Method of choice):
| Marker | Significance |
|---|---|
| IgM anti-HAV | Acute infection - appears at onset of symptoms, peaks at ~2 weeks, declines in 3-6 months |
| IgG anti-HAV | Past infection or vaccination; lifelong immunity |
Other tests:
- ELISA: Method of choice for measuring anti-HAV antibodies
- RT-PCR: Detects HAV RNA in stool (from 2 weeks before jaundice to 2 weeks after onset) - used in research/epidemiology
- Immune electron microscopy (IEM): Historical; HAV was originally identified this way in stool
- Liver function tests: Elevated ALT, AST; elevated bilirubin (direct and indirect)
- Stool HAV antigen detection: Immunoassays, nucleic acid hybridization
3.6 Treatment and Prevention
- Supportive treatment (no specific antiviral)
- Passive prophylaxis: Normal immunoglobulin (IG) within 2 weeks of exposure
- Active vaccination: Inactivated HAV vaccine (Havrix, Vaqta); 2 doses; long-lasting immunity
- TWINRIX: combined HAV + HBV vaccine (age ≥18 years)
4. HEPATITIS B (HBV)
4.1 Virology
- Family: Hepadnaviridae, Genus: Orthohepadnavirus
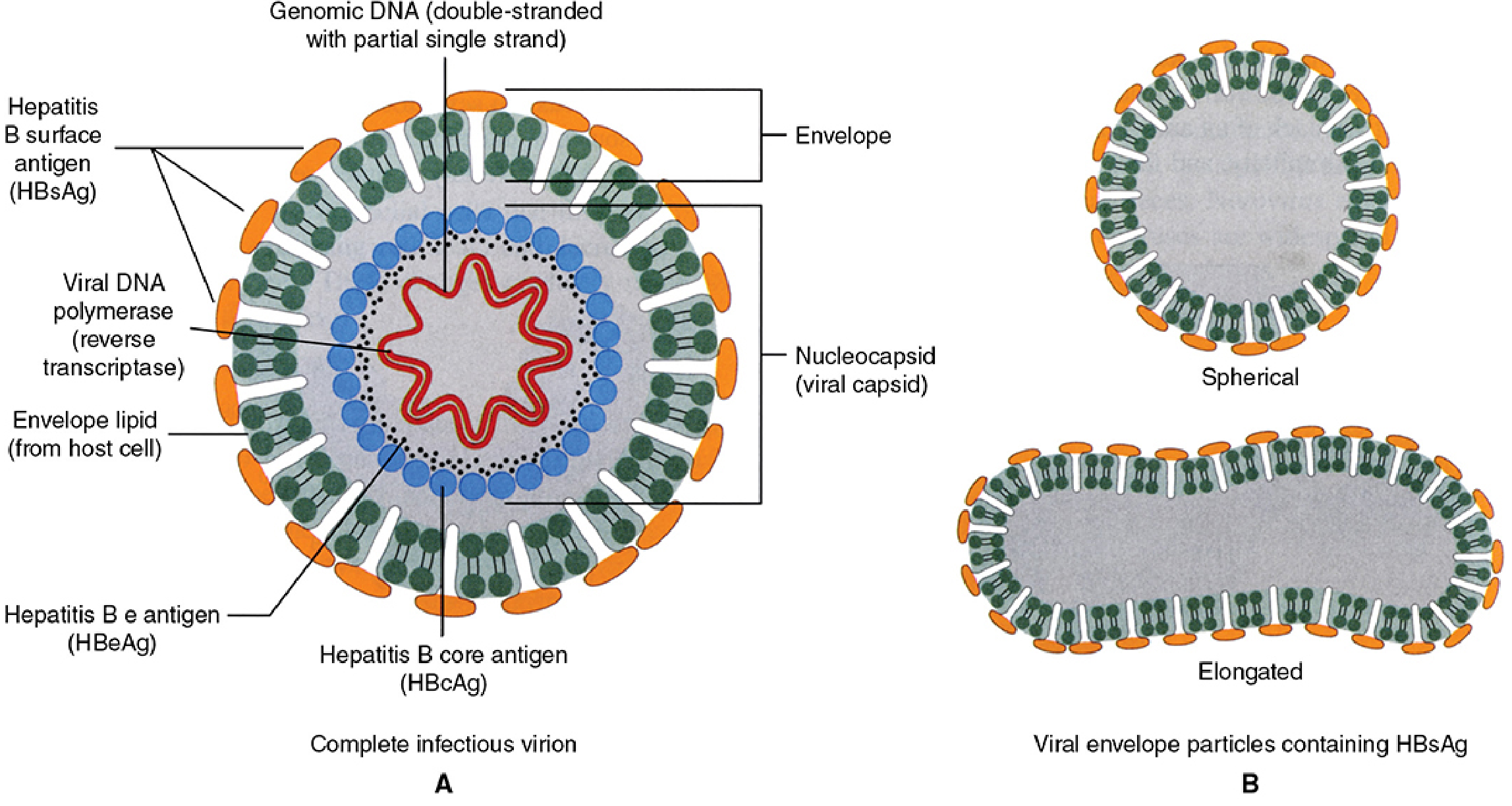
- 42 nm enveloped particle = Dane particle (the complete infectious virion)
- Additionally produces 22 nm spherical and filamentous subviral HBsAg particles (excess surface antigen - non-infectious, outnumber virions 1000:1 in serum)
- Partially double-stranded DNA genome (~3.2 kb), with a nick in the long strand
- Unique replication: Uses reverse transcriptase to convert pregenomic RNA → DNA
- Smallest human DNA virus
- 8 genotypes (A-H)
- 4 overlapping ORFs: Surface (preS1, preS2, S), Core (preC, C), Polymerase (P), X
Key antigens and antibodies:
| Antigen/Antibody | Location/Significance |
|---|---|
| HBsAg | Surface antigen; outer envelope; marker of active infection (acute or chronic) |
| Anti-HBs | Antibody to HBsAg; indicates immunity (from infection or vaccination); protective |
| HBcAg | Core antigen; not detectable in serum (intracellular); nucleocapsid protein |
| Anti-HBc IgM | Marker of acute HBV infection; also positive in "window period" |
| Anti-HBc IgG | Past infection (lifetime marker of exposure) |
| HBeAg | Secreted e antigen; marker of active viral replication and high infectivity |
| Anti-HBe | Appears as HBeAg clears; indicates decreasing replication |
| HBV DNA | Direct marker of viral replication; quantified by PCR for monitoring |
4.2 Epidemiology
- ~350-400 million chronic carriers worldwide; 2 billion have serological evidence of past infection
- Transmission:
- Parenteral: blood/blood products, needlestick, IV drug use, tattooing, hemodialysis
- Sexual: most common route in adults in developed countries
- Vertical (perinatal): mother-to-child during delivery; highest risk if mother is HBeAg positive; most important route in endemic areas (Asia)
- Incubation: 60-150 days (mean 90 days)
4.3 Pathogenesis
- HBV enters hepatocytes via NTCP (sodium taurocholate co-transporting polypeptide) receptor
- HBV itself is NOT directly cytopathic - liver damage is immune-mediated
- CD8+ cytotoxic T lymphocytes (CTL) attack HBV-infected hepatocytes - causes acute hepatitis and jaundice
- Immune complex deposition (HBsAg-anti-HBs) activates complement → serum sickness-like illness early on (rash, arthralgia)
- Inadequate immune response → chronic infection
Why does HBV cause higher chronicity in neonates? Neonates have an immature immune system, particularly deficient T-cell responses; they develop immune tolerance to HBV antigens encountered during development - resulting in >90% chronicity vs ~5-10% in immunocompetent adults.
4.4 Clinical Features
- Acute HBV: Gradual onset of fatigue, anorexia, nausea, RUQ pain; arthralgia/arthritis and rash (serum sickness-like) in early disease; progressing to jaundice, dark urine, clay stools
- Outcomes:
- 90% of immunocompetent adults resolve completely
- <1% develop fulminant hepatitis (massive hepatic necrosis, encephalopathy)
- ~10% adults → chronic hepatitis → cirrhosis → HCC (risk ~30% of cirrhotics)
- Neonates: >90% chronicity; young children: ~50%
4.5 Lab Diagnosis
Serological sequence of markers (see Figure below):
| Phase | HBsAg | Anti-HBs | HBeAg | Anti-HBe | Anti-HBc IgM | Anti-HBc IgG | HBV DNA |
|---|---|---|---|---|---|---|---|
| Incubation | + | - | + | - | - | - | + |
| Acute hepatitis | + | - | + | - | + | - | + |
| Window period | - | - | - | +/- | + | + | +/- |
| Recovery | - | + | - | + | - | + | - |
| Chronic infection (>6 months) | + | - | +/- | +/- | - | + | + |
| Vaccination | - | + | - | - | - | - | - |
| Past infection | - | + | - | + | - | + | - |
Key diagnostic interpretation:
- Acute HBV: HBsAg + Anti-HBc IgM (both positive)
- Chronic HBV: HBsAg positive for >6 months + Anti-HBc IgG
- Window period: Only Anti-HBc IgM detectable (HBsAg cleared, Anti-HBs not yet appeared) - must not be missed
- Immunity from infection: Anti-HBs + Anti-HBc IgG
- Immunity from vaccination: Anti-HBs alone (anti-HBc negative)
- High infectivity: HBeAg positive or HBV DNA high titer
- Pre-core mutant: HBsAg+ but HBeAg negative; anti-HBe positive; HBV DNA still detectable
Tests used:
- ELISA/CLIA (Chemiluminescent Immunoassay): For all serological markers (HBsAg, anti-HBs, HBeAg, anti-HBe, anti-HBc IgM/IgG)
- PCR (Quantitative HBV DNA): Gold standard for monitoring viral load; used to guide treatment decisions; also useful in window period
- Liver function tests: ALT, AST (elevated); bilirubin; prothrombin time
- Liver biopsy: Histology (Knodell/Metavir scoring of inflammation and fibrosis); ground-glass hepatocytes on H&E stain (accumulation of HBsAg in ER)
- Immunofluorescence: Detect HBsAg and HBcAg in liver biopsy specimens
- ELISA for HBsAg: First-line screening test in blood banks
4.6 Treatment and Prevention
- Acute: Supportive
- Chronic: Pegylated interferon-alpha, nucleoside/nucleotide analogues (Tenofovir, Entecavir, Lamivudine)
- Vaccine: Recombinant HBsAg subunit vaccine (Engerix-B, Recombivax HB); 3 doses at 0, 1, 6 months; >95% efficacy
- Neonatal prophylaxis: HBIG (hepatitis B immunoglobulin) + vaccine at birth for babies born to HBsAg-positive mothers
- Post-exposure prophylaxis: HBIG + vaccine within 24 hours of needlestick
5. HEPATITIS C (HCV)
5.1 Virology
- Family: Flaviviridae, Genus: Hepacivirus
- 50-60 nm, enveloped, positive-sense single-stranded RNA genome (~9.6 kb)
- Structural proteins: Core (C), Envelope (E1, E2)
- Non-structural proteins: NS2, NS3 (serine protease + helicase), NS4A, NS4B, NS5A (phosphoprotein), NS5B (RNA-dependent RNA polymerase) - key antiviral drug targets
- 6 major genotypes (1-6) with multiple subtypes; Genotype 1 most common globally
- High mutation rate due to error-prone RNA polymerase → hypervariable region 1 (HVR1) of E2 - major reason no vaccine is available
- No proofreading activity → quasispecies within host
5.2 Epidemiology
- ~170 million chronic carriers worldwide (~1% of world population; up to 10% in parts of Africa)
- Transmission primarily parenteral:
- IV drug users (~80%)
- Blood transfusion (pre-1992 screening)
- Hemodialysis patients
- Needlestick injuries (healthcare workers ~1%)
- Organ transplantation
- Sexual transmission: lower risk than HBV
- Vertical transmission: 3-10%
- Incubation period: 6-7 weeks average (range 2-26 weeks)
5.3 Pathogenesis
- HCV replicates primarily in liver (~10% of hepatocytes infected) but also in mononuclear cells
- Immune-mediated liver damage via CD8+ CTLs and proinflammatory cytokines
- Immune complex deposition → extrahepatic manifestations (vasculitis, arthritis, glomerulonephritis, cryoglobulinemia)
- HCV's ability to mutate rapidly and evade immune responses explains high chronicity rate
5.4 Clinical Features
- 75% asymptomatic in acute phase
- 25% develop symptoms: fever, fatigue, abdominal pain, anorexia, jaundice
- Fulminant hepatitis: rare
- Chronicity: 80-85% - the highest of all hepatitis viruses
- Chronic infection: waxing/waning, often asymptomatic, elevated or normal ALT
- Long-term: cirrhosis (20-30% over 20 years) → HCC
- Extrahepatic: essential mixed cryoglobulinemia, membranoproliferative glomerulonephritis, lymphoma, porphyria cutanea tarda, lichen planus
5.5 Lab Diagnosis
- Anti-HCV (ELISA/CLIA): Screening test; detects antibody to HCV; does not distinguish active from past infection (antibody persists); seroconversion takes 8-9 weeks; ~90% positive by 5 months
- HCV RNA by RT-PCR (Quantitative):
- Gold standard for confirming active infection
- Detectable as early as 1-2 weeks post-exposure (before antibody)
- Used for monitoring treatment response
- HCV genotyping: PCR-based; essential for treatment planning (determines regimen and duration)
- RIBA (Recombinant Immunoblot Assay): Confirmatory test (historical; now largely replaced by HCV RNA PCR)
- Core antigen detection (HCV Ag): Emerging test; positive during window period before antibody
- Liver biopsy: Histology for fibrosis staging (Metavir F0-F4) - important for treatment decisions
- Liver function tests: ALT (often fluctuating or normal), AST, bilirubin
Algorithm: Anti-HCV positive → confirm with HCV RNA PCR (if positive = active infection; if negative, may be past/cleared infection → recheck in 6 months)
5.6 Treatment and Prevention
- Direct-acting antivirals (DAAs): NS3/4A protease inhibitors (glecaprevir), NS5A inhibitors (pibrentasvir), NS5B polymerase inhibitors (sofosbuvir); cure rates >95% in 8-12 weeks
- Older regimens: Pegylated interferon-alpha + ribavirin (largely replaced)
- No vaccine available - due to high antigenic variability
- Prevention: universal blood product screening, harm reduction (needle exchange programs)
6. HEPATITIS D (HDV) - Delta Hepatitis
6.1 Virology
- Family: Deltaviridae, Genus: Deltavirus
- 35-37 nm, enveloped virus, uses HBsAg as its envelope (derived from HBV co-replicating in the same cell)
- Defective/satellite virus - absolutely requires HBV for replication and infection
- Negative-sense single-stranded circular RNA genome (~1.7 kb) - the smallest human pathogenic RNA virus
- Encodes only one protein: hepatitis D antigen (HDAg) in two forms - small (p24, promotes replication) and large (p27, inhibits replication; required for assembly)
- Resembles viroids of plants
6.2 Epidemiology
- Found worldwide; highest prevalence in Italy, Middle East, Central Asia, West Africa, South America
- Two patterns of infection:
- Co-infection: Simultaneous acquisition of HDV and HBV (usually more severe acute disease but lower chronicity ~5%)
- Superinfection: HDV infection in a chronic HBV carrier (70-80% chronicity; more severe; more likely to progress to fulminant hepatitis or cirrhosis)
- Routes of transmission: similar to HBV (parenteral, sexual)
- HDV does not spread perinatally as readily as HBV
- IV drug users and hemophiliacs are high-risk groups
6.3 Clinical Features
- Co-infection: Acute hepatitis; self-limited in most; fulminant hepatitis more common (~5%) than HBV alone
- Superinfection: Higher risk of fulminant hepatitis (~20%); rapid progression to cirrhosis; chronic disease in up to 80%
- Clinically can mimic acute hepatitis B exacerbation
6.4 Lab Diagnosis
| Test | Significance |
|---|---|
| HBsAg positive | Required (HDV cannot exist without HBV) |
| Anti-HDV (IgM) | Acute HDV infection |
| Anti-HDV (IgG) | Past or chronic HDV |
| Anti-HBc IgM positive + Anti-HDV positive | Co-infection (both viruses acquired simultaneously) |
| Anti-HBc IgG positive + Anti-HDV positive | Superinfection (HDV in chronic HBV carrier) |
| HDAg | Detectable early in acute infection (disappears quickly) |
| HDV RNA by PCR | Confirms active HDV replication |
6.5 Treatment and Prevention
- No specific treatment for acute HDV; supportive
- Pegylated interferon-alpha for chronic HDV (limited efficacy)
- Bulevirtide (entry inhibitor) - newer approved agent
- Prevention of HBV = Prevention of HDV: HBV vaccination protects against HDV co-infection
- HBV carriers should be advised on safe practices to prevent superinfection
7. HEPATITIS E (HEV)
7.1 Virology
- Family: Hepeviridae, Genus: Hepevirus
- 27-34 nm, non-enveloped (naked capsid), icosahedral with surface spikes
- Positive-sense single-stranded RNA genome (7.2 kb)
- Three ORFs: ORF-1 (nonstructural: methyltransferase, protease, helicase, RdRp); ORF-2 (capsid protein); ORF-3 (multifunctional small protein - virus release)
- 4 genotypes: Genotype 1 (Asia, Africa), Genotype 2 (Mexico, West Africa), Genotype 3 (developed countries, zoonotic), Genotype 4 (China, Taiwan, Japan)
- Resembles caliciviruses but is distinct
7.2 Epidemiology
- ~20 million infections/year worldwide; 44,000 deaths in 2015 (WHO data)
- Fecal-oral route primary transmission - via contaminated water (large outbreaks in endemic areas)
- Endemic areas: South Asia (India), East Asia, Africa, Central America, Mexico
- Genotypes 1 & 2: epidemic waterborne; Genotypes 3 & 4: zoonotic (pigs, boar, deer - undercooked meat; isolated cases in developed countries)
- Affects young adults predominantly; rare in infants
- Special risk: Pregnant women (especially 3rd trimester) - 20-25% mortality from fulminant hepatic failure
7.3 Pathogenesis
- Oral ingestion → GI replication → viremia → hepatocellular damage
- Immune-mediated mechanism
- Self-limited in most healthy individuals
- No chronic infection in immunocompetent hosts
- Exception: Immunosuppressed patients (organ transplant recipients) can develop chronic HEV infection - primarily genotype 3
7.4 Clinical Features
- Clinically resembles hepatitis A - self-limiting acute illness
- Incubation: 15-60 days (mean 40 days)
- Symptoms: malaise, anorexia, nausea, vomiting, RUQ pain, fever, jaundice
- Severe in pregnancy: 20-25% mortality; associated with fulminant hepatitis, DIC, fetal loss
- No carrier state in immunocompetent hosts; very rare chronicity
7.5 Lab Diagnosis
- Anti-HEV IgM: Diagnostic of acute infection; appears at onset of symptoms
- Anti-HEV IgG: Past infection; seroprevalence marker
- HEV RNA by RT-PCR: Confirms active replication; useful early in infection before antibody appearance; also in stool and blood
- Liver function tests: Elevated ALT, AST, bilirubin
- Diagnosis is confirmed serologically as "cases of hepatitis E are not clinically distinguishable from other types of acute viral hepatitis" (Park's Textbook of Preventive & Social Medicine)
- Electron microscopy of stool: Historical - 27-34 nm particles
7.6 Treatment and Prevention
- Primarily supportive (no licensed antiviral for immunocompetent)
- Ribavirin used in chronic HEV in transplant patients
- HEV vaccine (Hecolin): Approved in China; not yet globally licensed
- Prevention: safe drinking water, proper sanitation, avoiding uncooked pork/wild game
- Pregnant women in endemic areas should be especially cautious
8. COMPREHENSIVE LABORATORY DIAGNOSIS
8.1 General Biochemical (Non-specific) Tests
| Test | Finding in Acute Hepatitis |
|---|---|
| Serum ALT (SGPT) | Markedly elevated (best indicator of hepatocyte damage); ALT > AST |
| Serum AST (SGOT) | Elevated (ALT:AST >1 in viral hepatitis; <1 in alcoholic hepatitis) |
| Serum Bilirubin | Total, direct (conjugated), indirect all elevated |
| Serum Alkaline Phosphatase | Mildly elevated |
| Serum Albumin | Decreased in chronic/severe hepatitis (marker of synthetic function) |
| Prothrombin Time (PT) | Prolonged in severe hepatitis (marker of synthetic function) |
| Urine Bilirubin | Present (bilirubinuria = early sign before jaundice visible) |
| Urine Urobilinogen | Initially elevated; absent in complete cholestasis |
| CBC | Lymphocytosis; mild thrombocytopenia |
8.2 Specific Virological Tests
Serological Methods:
- ELISA (Enzyme-Linked Immunosorbent Assay): Used for all hepatitis virus antibody/antigen detection; screening method of choice
- CLIA (Chemiluminescent Immunoassay): More sensitive automated version of ELISA
- RIBA (Recombinant Immunoblot Assay): Confirmatory for anti-HCV (largely replaced by PCR)
Molecular Methods:
- RT-PCR (Reverse Transcription PCR): For HAV RNA, HCV RNA, HEV RNA (RNA viruses)
- PCR: For HBV DNA, HDV RNA
- Quantitative PCR (viral load): For HBV DNA and HCV RNA - essential for monitoring treatment
- Genotyping: For HCV (treatment planning) and HBV
Histological Methods:
- Liver Biopsy with H&E staining:
- Piecemeal necrosis, bridging necrosis, portal inflammation
- Ground-glass hepatocytes: Characteristic of chronic HBV (HBsAg accumulation in smooth ER)
- Immunohistochemistry: For HBsAg and HBcAg in tissue
- Immunofluorescence: For viral antigens in liver tissue
Electron Microscopy:
- Immune electron microscopy (IEM): Original method to detect HAV in stool; historical
8.3 Quick Reference: Specific Diagnostic Markers by Virus
| Virus | Best Screening Test | Confirmatory Test | Active Replication Marker |
|---|---|---|---|
| HAV | Anti-HAV IgM | - (sufficient for diagnosis) | HAV RNA by RT-PCR (stool) |
| HBV | HBsAg | Anti-HBc IgM (for acute); HBV DNA PCR | HBeAg / HBV DNA |
| HCV | Anti-HCV (ELISA) | HCV RNA by RT-PCR | HCV RNA by RT-PCR |
| HDV | Anti-HDV + HBsAg | HDV RNA by PCR | HDAg / HDV RNA |
| HEV | Anti-HEV IgM | HEV RNA by RT-PCR | HEV RNA in stool/serum |
9. HEPATITIS G (HGV / GBV-C)
- Discovered 1996; Flaviviridae family, Pegivirus genus
- Not associated with any clinical liver disease
- Found in ~1-2% of blood donors
- Often detected in patients co-infected with HCV or HIV
- Interestingly, HGV co-infection may slow HIV progression (experimental observation)
- No specific treatment or vaccine needed
- Of academic interest in blood screening and transfusion medicine
10. NON-A-TO-E HEPATITIS
- A term used when standard serological testing for HAV, HBV, HCV, HDV, and HEV is negative
- May represent:
- Uncharacterized viruses
- Drug-induced hepatitis
- Autoimmune hepatitis
- HGV or TTV (Torque Teno Virus) - not confirmed as clinical hepatitis agents
11. SPECIAL SITUATIONS IN HEPATITIS B SEROLOGY
The "Window Period"
- Occurs in acute HBV when HBsAg has cleared but anti-HBs has not yet appeared
- Only anti-HBc IgM is detectable during this period
- Window period may last days to weeks
- Clinically important: A patient may appear seronegative for HBsAg but be actively infected
Pre-core Mutant HBV
- Mutation in pre-core region prevents synthesis of HBeAg
- Patient is HBsAg positive but HBeAg negative; yet HBV DNA is detectable by PCR
- Anti-HBe is positive
- Common in Mediterranean countries and Asia
- Can still cause progressive liver disease
Occult HBV
- HBsAg negative but HBV DNA detectable in serum/liver
- Often anti-HBc IgG positive
- Risk of reactivation with immunosuppression
12. SUMMARY TABLE - KEY FACTS FOR EXAMS
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Diagnostic gold standard | Anti-HAV IgM | HBsAg + Anti-HBc IgM | Anti-HCV confirmed by HCV RNA PCR | Anti-HDV + HBsAg | Anti-HEV IgM |
| Window period diagnosis | N/A | Anti-HBc IgM | HCV RNA PCR | HDV RNA | HEV RNA/Anti-HEV IgM |
| Fecal-oral | Yes | No | No | No | Yes |
| Chronicity | No | 10% (adults) | 80-85% | 50-80% | No* |
| Vaccine | Yes | Yes | No | (HBV vax) | Partial |
| High-risk pregnancy | No | Vertical transmission | Vertical ~3-10% | Rare | Fulminant (20-25% mortality) |
| Carrier state | No | Yes | Yes | Yes | No |
| HCC risk | No | Yes | Yes | Yes | No |
| Specific antivirals | No | Yes (NUCs, IFN) | Yes (DAAs) | IFN, Bulevirtide | Ribavirin (chronic/immunosuppressed) |
References: Jawetz, Melnick & Adelberg's Medical Microbiology 28th Ed.; Sherris & Ryan's Medical Microbiology 8th Ed.; Tietz Textbook of Laboratory Medicine 7th Ed.; Harrison's Principles of Internal Medicine 22nd Ed.; Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.