post laryngectomy rehabilitation in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
laryngectomy rehabilitation voice restoration
tracheoesophageal puncture voice prosthesis laryngectomy
laryngectomy quality of life swallowing rehabilitation
heat moisture exchanger laryngectomy pulmonary rehabilitation
post laryngectomy rehabilitation RGUHS ENT 50 marks tracheoesophageal speech voice restoration
electrolarynx digital voice aid laryngectomy communication
Blom Singer Provox voice prosthesis indwelling vs exdwelling types comparison laryngectomy
laryngectomy psychological rehabilitation counseling support
POST-LARYNGECTOMY REHABILITATION
A Comprehensive Guide for RGUHS Examinations (50 Marks)
INTRODUCTION
- Voice/Speech rehabilitation
- Swallowing rehabilitation
- Pulmonary/respiratory rehabilitation (Heat and Moisture Exchange)
- Stoma care
- Psychological and social rehabilitation
- Nutritional rehabilitation
- Olfaction and taste rehabilitation
FLOWCHART 1: Overview of Post-Laryngectomy Rehabilitation
TOTAL LARYNGECTOMY
|
├──────────────────────────────────────────────┐
↓ ↓
IMMEDIATE/EARLY LONG-TERM
REHABILITATION REHABILITATION
(Perioperative period) (Weeks-months-years)
| |
┌─────┴──────┐ ┌────────────────┼───────────────┐
↓ ↓ ↓ ↓ ↓
Wound care Nasogastric VOICE SWALLOW PULMONARY
Stoma care tube feeding REHAB REHAB REHAB (HME)
Counseling (7-10 days) |
↓ ┌────┼─────┐
Oral diet ES TEP EL AAC
PART I: VOICE AND SPEECH REHABILITATION
Physiology of Alaryngeal Voice
Prerequisites for Good Alaryngeal Voice
| Factor | Requirement |
|---|---|
| PE segment tone | Tonic (neither hypo- nor hypertonic) |
| Stoma size | Adequate for valve maintenance |
| Lung function | Adequate expiratory pressure |
| Motivation | High patient motivation |
| Cognitive function | Intact enough to learn technique |
THREE MAIN METHODS OF VOICE REHABILITATION
METHOD 1: TRACHEO-ESOPHAGEAL PUNCTURE / SURGICAL VOICE RESTORATION (TEP/SVR) - GOLD STANDARD
- 1980: Blom and Singer described TEP with a voice prosthesis
- Original concept: An anecdotal observation when a laryngectomee deliberately punctured the posterior tracheal wall (with a heated ice pick), discovered that stoma occlusion + exhalation produced a voice
- Singer and Blom (1980) formalized the technique
| Timing | Type | When Performed |
|---|---|---|
| Primary TEP | At time of laryngectomy | Same operative sitting |
| Secondary TEP | After healing | 6-8 weeks post-op |
- Avoids a second procedure
- Allows earlier voice rehabilitation
- Does not increase fistula risk when done in elective (non-salvage) cases
- Scott-Brown's: "No good evidence that this increases the risk of pharyngocutaneous fistula formation."
FLOWCHART 2: TEP Voice Production Mechanism
EXPIRATION (patient closes stoma with finger or HME valve)
↓
Air passes from TRACHEA → through ONE-WAY PROSTHETIC VALVE → ESOPHAGUS
↓
Air causes vibration of PE SEGMENT (neoglottis / vibratory segment)
↓
SOUND produced → amplified by PHARYNGEAL RESONATING CAVITIES
↓
Modified by ARTICULATORS (tongue, lips, teeth, palate) → SPEECH
Voice Prostheses - Types and Classification
| Type | Description | Changed by |
|---|---|---|
| Indwelling (in-situ) | Stays in place for weeks-months | Healthcare professional only |
| Ex-dwelling (non-indwelling) | Removed by patient or carer | Patient/carer |
- Blom-Singer (InHealth Technologies) - classic, low pressure, advantage, dual valve
- Provox series (Atos Medical) - Provox, Provox 2, Provox Vega, Provox NID, Provox ActiValve
- VoiceMaster, HiPro, Henley-Cohn, Staffieri (older/less used)
- Tracheal flange
- Esophageal flange
- One-way valve (duckbill or slit design)
- Retention strap/collar

Candidacy Criteria for TEP
- Adequate stoma size (≥1.5 cm diameter)
- Good manual dexterity (for self-care)
- Adequate pulmonary reserve
- Motivated patient
- Adequate visual acuity
- Good caregiver support (if patient dependent)
- Very small stoma
- Severe COPD (cannot build adequate pressure)
- Dementia/severe cognitive impairment
- Inability to manage prosthesis
- Severe radiation fibrosis
- Very poor general condition
Hands-Free Speech
- The valve seals during expiration (when pressure builds)
- Opens during inspiration
- Patient achieves spontaneous hands-free voice
PE Segment Tonicity - Problems and Management
FLOWCHART 3: PE Segment Tonicity Assessment and Management
POOR TE SPEECH
↓
VIDEOFLUOROSCOPY + INSUFFLATION TEST
/ \
HYPOTONICITY HYPERTONICITY/SPASM
(voice weak, (voice high pitched,
whispery, wet) effortful, absent)
↓ ↓
Digital pressure Myotomy (at surgery) OR
against neck ↓
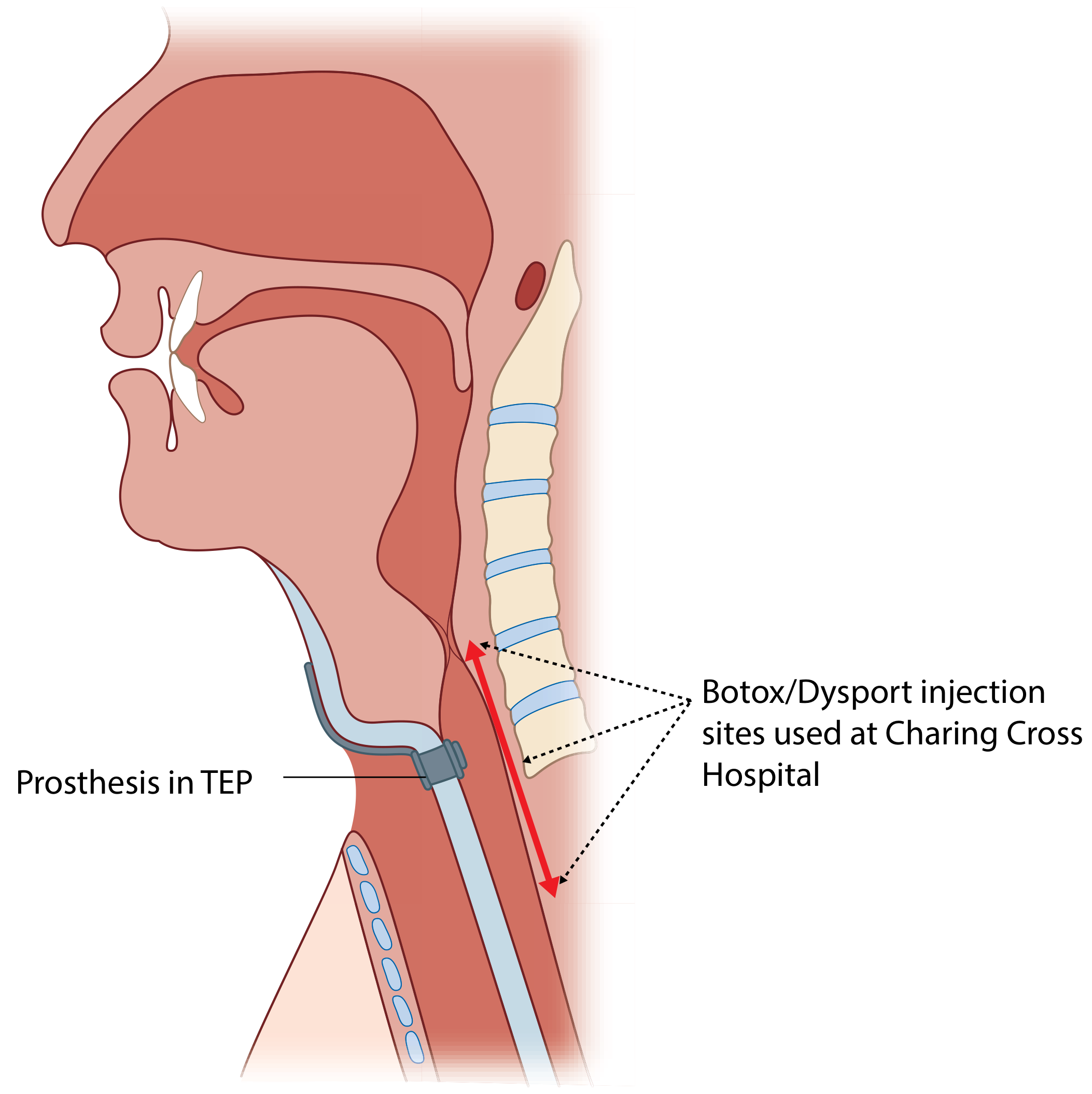
Low pressure prosthesis POST-OP: Botulinum toxin
injection (unilateral, 3 sites)
OR Secondary myotomy
(rarely done now)
- Injected unilaterally at 3 sites along the posterior cricopharyngeal myotomy line
- Dosage: guided by degree of hypertonicity, neck fibrosis, prior myotomy
- Can be repeated
- Preceded by lignocaine injection to confirm diagnosis
Complications of TEP and Voice Prosthesis
| Complication | Cause | Management |
|---|---|---|
| Leakage through prosthesis | Candida valve damage | Nystatin/antifungal, prosthesis change |
| Leakage around prosthesis | TEP enlargement | Tissue augmentation (collagen, fat) |
| Prosthesis dislodgement | Poor fitting | Re-sizing, stoma revision |
| Granulation tissue | Foreign body reaction, Candida | Steroids, silver nitrate, excision |
| TEP stenosis/closure | Healing/fibrosis | Dilation, re-puncture |
| Aspiration | Valve failure | Prosthesis change |
| Candida colonization | Biofilm formation | Antifungals, daily cleaning |
- Daily brushing and flushing of prosthesis in situ
- Optional liquid antifungal (nystatin) via flush
- Exdwelling: removed, washed, sterilized overnight in 3% hydrogen peroxide
- Antifungal-impregnated prostheses available
- Newer fungal-resistant materials under development
METHOD 2: ESOPHAGEAL SPEECH (ES)
| Method | Learning | Equipment | Sound quality | Cost |
|---|---|---|---|---|
| Injection | Active tongue pressure used | None | Better | Free |
| Inhalation | Passive air sucked in | None | Variable | Free |
- No prosthesis, no surgery
- No equipment dependency
- Most natural-sounding of non-surgical methods
- "Hands-free" - no stoma occlusion needed
- Hardest to learn (only ~30% achieve functional speech)
- Short utterances (limited air reservoir)
- Low volume, poor loudness
- Long training period (months)
- Old literature: ~25-30% achieve functional ES
- Success dependent on PE segment characteristics
METHOD 3: ELECTROLARYNX (EL)
- Transcervical (neck-type) - most common; device held against neck/submandibular region; vibrations transmitted through skin
- Intraoral - tube placed in mouth corner; for patients with neck radiation/fibrosis
- Servox (most widely used)
- Western Electric #5
- TruTone
- NuVois
- Easy to learn (available immediately post-op)
- Reliable
- Good for immediate communication post-laryngectomy
- Mechanical, robotic sound quality
- Both hands required (or neck placement)
- Cannot be used while eating
- Needs battery/maintenance
- Poor acceptance long-term
METHOD 4: AAC (AUGMENTATIVE AND ALTERNATIVE COMMUNICATION)
- Writing pads/whiteboards
- Mobile phone/tablet text-to-speech apps
- Sign language
- Lip-reading facilitated communication
FLOWCHART 4: Algorithm for Post-Laryngectomy Voice Rehabilitation
POST-LARYNGECTOMY
↓
PRE-OPERATIVE COUNSELLING
(SLT, surgeon, ENT team)
↓
SURGERY
TEP TIMING?
/ \
PRIMARY NO PRIMARY TEP
TEP (complex, salvage,
↓ poor candidate)
Prosthesis ↓
placed IMMEDIATE:
same op Electrolarynx
↓ +
└───────→ Esophageal speech training
↓
6-8 weeks: SECONDARY TEP assessment
↓
PE segment assessment (videofluoroscopy + insufflation)
↓ ↓
TONIC PE segment HYPER/HYPO-TONIC PE
↓ ↓
TEP + Prosthesis Correct tonicity first,
then TEP
PART II: SWALLOWING REHABILITATION
Physiological Changes After Laryngectomy
| Phase | Normal Laryngeal Swallow | Alaryngeal Swallow |
|---|---|---|
| Oral | Lips seal, tongue forms bolus | Same |
| Pharyngeal | Larynx elevates, epiglottis covers | Larynx absent; reduced stripping action |
| Laryngeal | Laryngeal sphincters protect airway | Absent (no larynx) |
| Oesophageal | Normal peristalsis | Modified PE opening |
Swallowing Problems Post-Laryngectomy
- Pharyngo-esophageal stenosis/stricture - most common (5-30%)
- At surgical closure site or throughout neopharynx
- Investigation: Esophagography (barium swallow), endoscopy
- Management: Serial dilatation, surgical revision
- Pharyngocutaneous fistula - early complication (10-15%)
- Risk factors: Prior radiotherapy, malnutrition, diabetes
- Detected by esophagogram (extravasation)
- Management: Conservative initially (NPO, NG tube feeding), surgical closure if persistent
- Pseudoepiglottis - normal post-op appearance
- Ridge of tissue at anterior surgical bed on fluoroscopy
- Looks like epiglottis (benign)
- Dysphagia due to radiation fibrosis - progressive
- Long-term: stricture, hypopharyngeal scarring
- Management: Dilatation, swallowing therapy, PEG/PEJ tube
Post-Laryngectomy Swallowing Rehabilitation
- Nasogastric tube feeding
- Nothing by mouth
- Cummings: Feeding typically commenced within 5-7 days post-op (in narrow-field laryngectomy with linear stapler closure)
- Videofluoroscopic swallowing study (VFSS) before oral feeding
- Start with thin liquids or thickened fluids (depending on VFSS findings)
- Speech-language therapist guidance
- Bolus modification (texture, consistency)
- Compensatory swallowing maneuvers
- Postural adjustments
- Thermal-tactile stimulation
- Exercises to strengthen tongue base, pharyngeal constrictors
PART III: PULMONARY AND RESPIRATORY REHABILITATION - HEAT AND MOISTURE EXCHANGER (HME)
Physiological Basis
- Warms inspired air to 32°C
- Humidifies air to 95% relative humidity
- Filters particulate matter
- Reduces airways resistance
- Increased mucus production
- Crusting and coughing
- Increased respiratory infections
- Poor sleep quality
- Reduced exercise tolerance
Heat and Moisture Exchanger (HME)
- Small hygroscopic/hygrothermic filter contained in a cassette
- Attached to stoma by: a. Base plate (adhesive on para-stomal skin) b. Inserted into laryngectomy tube
- Standard daily activity HME
- Night HME (lower resistance)
- Exercise HME (higher capacity)
- HME with voice valve attached (enables hands-free speech + pulmonary rehab simultaneously)
- A 2023 study (Ward et al., Head Neck 2023, PMID 36808179) showed significant improvement in pulmonary and related symptoms following adoption of an optimal day-and-night HME regimen
- A 2022 RCT (Longobardi et al., Otolaryngol Head Neck Surg 2022, PMID 35316144) confirmed new generation HME devices optimize pulmonary outcomes post-laryngectomy
PART IV: STOMA CARE AND MANAGEMENT
Immediate Stoma Care
- Tracheostomy tube (Shiley/Portex) placed initially
- Regular suctioning (initially)
- Humidified environment in ICU/ward
- Patient education: stoma hygiene
Long-term Stoma Care
- Laryngectomy button or tube insertion
- Regular dilatation if stenosis develops
- Surgical stoma revision (if too narrow for valve/HME)
- Clean with soft gauze/cloth
- Remove crusts gently
- HME cassette changed daily
- All laryngectomees should carry an ID card/medic-alert bracelet
- Emergency resuscitation: bag-mask to stoma (NOT mouth)
- Standard mouth-to-mouth CPR ineffective/dangerous
FLOWCHART 5: Stoma Complications and Management
STOMA PROBLEMS
|
├─── STENOSIS ──→ Dilatation → Revision stoma surgery
|
├─── SECRETIONS/CRUSTING ──→ HME / Humidification / Saline instillation
|
├─── STOMAL RECURRENCE ──→ PET-CT / Biopsy → Salvage RT/surgery
|
└─── PERISTOMAL SKIN PROBLEMS ──→ Change base plate / Skin barrier creams
PART V: PSYCHOLOGICAL AND SOCIAL REHABILITATION
Psychological Impact of Laryngectomy
- Loss of natural voice (major identity/communication impact)
- Altered body image (permanent neck stoma)
- Fear of cancer recurrence
- Social isolation (difficulty in communication)
- Employment difficulties
- Anxiety and depression (documented in up to 40% of patients)
Psychological Rehabilitation Strategies
- Comprehensive counseling by surgeon + SLT
- Meeting with a "laryngectomee visitor" (peer support from experienced patient)
- Clear explanation of voice rehabilitation options
- Family/caregiver involvement
- Continued counseling and emotional support
- SLT visits during inpatient stay
- Occupational therapy assessment
- Depression screening (PHQ-9)
- Laryngectomy support groups (e.g., National Association of Laryngectomee Clubs - NALC)
- Online support communities
- Vocational rehabilitation / return to work planning
- Marriage/relationship counseling as needed
PART VI: NUTRITIONAL REHABILITATION
Phases
- Nasogastric tube: standard
- PEG (percutaneous endoscopic gastrostomy): if long-term feeding needed (post-radiation patients)
- Nutritional goals: 25-35 kcal/kg/day, 1.2-1.5 g protein/kg/day
- Modified texture diets as per VFSS findings
- Dietitian involvement
- Monitor weight, albumin, prealbumin
- Soft/normal diet usually achieved
- Address specific deficiencies (Vitamin D, zinc)
- Weight monitoring
PART VII: OLFACTION AND TASTE REHABILITATION
Nasal Airflow Induction Maneuver (NAIM) - "Polite Yawn"
- Patient performs a gentle "polite yawn" with lips closed (lowering floor of mouth, drawing air nasally)
- This creates low-pressure nasal airflow
- Restores smell and taste to near-normal
- Can be taught by SLT or OT
PART VIII: MULTIDISCIPLINARY TEAM IN REHABILITATION
| Team Member | Role |
|---|---|
| Head & Neck Surgeon/ENT | Surgical technique, stoma revision, TEP |
| Speech-Language Therapist (SLT) | Voice/swallowing rehabilitation, TEP management |
| Oncologist (radiation/medical) | Cancer surveillance, chemoradiation effects |
| Dietitian/Nutritionist | Nutritional support |
| Physiotherapist | Shoulder/neck exercises, pulmonary rehab |
| Psychologist/Psychiatrist | Mental health, counseling |
| Occupational Therapist | ADL, olfaction rehab |
| Specialist Nurse | Stoma care, wound care, patient education |
| Social Worker | Financial aid, vocational rehabilitation |
PART IX: SECONDARY VOICE RESTORATION
Assessment Steps for Secondary TEP (Scott-Brown's):
- PE segment tonicity assessment - videofluoroscopy first
- Botulinum toxin injection if PE segment is hypertonic
- Stoma assessment - revise if too narrow
- Lung function - must be adequate
- TEP creation under endoscopic/surgical guidance
- Prosthesis sizing - careful measurement with sizing gauge
- Prosthesis selection - from range of diameters/lengths/opening pressures
FLOWCHART 6: Secondary TEP Decision Algorithm
PATIENT WITH FAILED / INADEQUATE VOICE POST-LARYNGECTOMY
↓
Videofluoroscopy + insufflation test
↓ ↓ ↓
HYPERTONIC HYPOTONIC TONIC
PE segment PE segment PE segment
↓ ↓ ↓
Botulinum toxin Consider digital PROCEED to TEP
injection pressure + ↓
↓ encourage ES Stoma adequate?
Reassess ↓ ↓
↓ YES NO
TEP + prosthesis ↓ Stoma revision
Create TEP ↓
↓ Then TEP
Size + select
prosthesis
↓
Voice training
(SLT-guided)
PART X: RECENT ADVANCES (2023-2026)
1. Systemic Review of TE Voice Therapy (2026)
2. HME Optimization
- Next-generation HME devices (Almajali et al., Ear Nose Throat J 2026, PMID 37776012) demonstrate significantly reduced cough, secretions, and improved QOL compared to older HME generation.
- 3D-printed reusable metal HME (Leemans et al., Respir Care 2023) - sustainable design reducing environmental waste and cost.
- Optimal day-and-night HME regimen proven to improve pulmonary symptoms significantly (Ward et al., Head Neck 2023).
3. Tissue Augmentation for Periprosthetic Leakage
4. TEP in Emergency Settings
5. Dysphagia Management Advances (2026)
- High-resolution manometry for dysphagia assessment
- Neuromuscular electrical stimulation (NMES/VitalStim)
- Pharyngeal electrical stimulation
- Surface EMG biofeedback
6. AI-Powered Voice Restoration
- AI-based voice synthesis apps for text-to-speech that mimic the patient's pre-operative voice using AI learning (emerging technology)
- Neural interface neuroprosthetics for silent speech decoding (experimental)
7. Quality of Life Evidence
8. Laryngeal Transplantation (Experimental)
COMPARATIVE TABLE: Three Methods of Voice Rehabilitation
| Feature | Esophageal Speech | Electrolarynx | TEP/SVR |
|---|---|---|---|
| Sound source | PE segment | Battery device | PE segment |
| Air source | Esophageal air | Electrical vibration | Pulmonary air |
| Stoma occlusion needed | No | No | Yes (finger/valve) |
| Surgery needed | No | No | Yes (TEP) |
| Equipment cost | Nil | Moderate | High (prosthesis) |
| Speech quality | Variable | Robotic | Most natural |
| Learning difficulty | Hardest | Easiest | Moderate |
| Hands-free possible | Yes | No | Yes (with ATSV) |
| Success rate | 25-30% functional | ~95% | 80-90% with TEP |
| Volume | Low | Moderate | Good |
| Immediate availability | No (weeks) | Yes | Yes (primary TEP) |
KEY EXAMINATION POINTS (RGUHS Focus)
- Gold standard for voice rehabilitation = TEP (Surgical Voice Restoration)
- First described by = Blom and Singer (1980)
- PE segment (pharyngo-esophageal segment) = the new vibrating source = neoglottis = pseudoglottis
- Primary TEP = at time of laryngectomy; Secondary TEP = later (6-8 weeks+)
- Indwelling prosthesis = changed by surgeon/SLT; Exdwelling = changed by patient
- HME = artificial nose; essential for pulmonary rehabilitation
- Botulinum toxin = management of PE segment hypertonicity/spasm
- Candida = most common cause of voice prosthesis failure
- NAIM ("polite yawn") = technique to restore olfaction post-laryngectomy
- Videofluoroscopy = best investigation before TEP for PE segment assessment
- Pharyngocutaneous fistula = commonest early complication of laryngectomy (10-15%)
- Pharyngo-esophageal stenosis/stricture = commonest late swallowing complication
SUMMARY DIAGRAM: Post-Laryngectomy Rehabilitation - At a Glance
┌─────────────────────────────────────────────────────────────────┐
│ POST-LARYNGECTOMY REHABILITATION │
│ │
│ ┌──────────┐ ┌──────────┐ ┌──────────┐ ┌───────────────┐ │
│ │ VOICE │ │ SWALLOW │ │PULMONARY │ │ PSYCHOSOCIAL │ │
│ │ REHAB │ │ REHAB │ │ REHAB │ │ REHAB │ │
│ │ │ │ │ │ (HME) │ │ │ │
│ │ 1. TEP │ │ NG tube │ │ Artificial│ │ Pre-op counsel│ │
│ │ (GOLD │ │ → Oral │ │ nose │ │ Peer visitor │ │
│ │ STANDARD)│ │ feeding │ │ cassette │ │ Support group │ │
│ │ 2. ES │ │ VFSS │ │ Stoma │ │ SLT + psychol.│ │
│ │ 3. EL │ │ Dilatation│ │ hygiene │ │ │ │
│ │ 4. AAC │ │ Therapy │ │ │ │ │ │
│ └──────────┘ └──────────┘ └──────────┘ └───────────────┘ │
│ │
│ ┌─────────────────────────────────────────────────────────┐ │
│ │ MULTIDISCIPLINARY TEAM │ │
│ │ ENT Surgeon | SLT | Oncologist | Dietitian │ │
│ │ Psychologist | Physiotherapist | OT | Nurse │ │
│ └─────────────────────────────────────────────────────────┘ │
└─────────────────────────────────────────────────────────────────┘
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 1, 8th Ed) - Chapter 15: Post-laryngectomy rehabilitation; Secondary voice restoration; Heat and Moisture Exchange; Swallow
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 2, 9th Ed) - Laryngectomy chapter
- Cummings Otolaryngology Head and Neck Surgery (7th Ed) - Total Laryngectomy chapter; Radiological assessment of post-laryngectomy neopharynx
- Dhingra PL, Dhingra S - Diseases of ENT, Head & Neck Surgery - Laryngectomy and rehabilitation
- Hazarika P - Textbook of ENT and Head & Neck Surgery - Laryngeal carcinoma and rehabilitation
- Stell PM, Maran AGD - Head and Neck Surgery - Voice restoration post-laryngectomy
- Zakir Hussain - ENT for ENT Surgeons - Laryngeal surgery and rehabilitation
- Sparks F, Coffey M, Dipper L. Tracheoesophageal Voice Therapy in Postlaryngectomy Rehabilitation: A Systematic Review. J Voice. 2026 Mar. PMID: 38000962
- Ward EC et al. Post-laryngectomy pulmonary and related symptom changes following adoption of an optimal day-and-night HME regimen. Head Neck. 2023 Apr. PMID: 36808179
- Mayo-Yanez M et al. Tissue augmentation treatment for periprosthetic leakage: A systematic review. Clin Otolaryngol. 2023. PMID: 37012583
- Longobardi Y et al. Optimizing Pulmonary Outcomes After Total Laryngectomy: Crossover Study on New HMEs. Otolaryngol Head Neck Surg. 2022. PMID: 35316144
- Murariu MO et al. Psychological Distress and Quality of Life in Patients with Laryngeal Cancer: A Review. Healthcare (Basel). 2025. PMID: 40648576
- Schellen C et al. Management of dysphagia in head and neck cancer: current and future perspectives. Front Oncol. 2026. PMID: 41939474
- Almajali O et al. New Generation HME in Laryngectomized Patients. Ear Nose Throat J. 2026. PMID: 37776012
Note for RGUHS students: This answer covers all standard domains expected for a 50-mark question as per RGUHS MS (ENT) syllabus: voice rehabilitation (methods, TEP in detail, candidacy, prostheses, complications), swallowing rehabilitation, pulmonary rehabilitation (HME), stoma care, psychological rehabilitation, multidisciplinary team, and recent advances. Draw the flowcharts clearly in the exam with labeled boxes and arrows - examiners specifically reward systematic diagrammatic representation.