Lens related glaucoma refer kansikis clinical ophthalmology and give answers
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content from Kanski's 10th edition. Let me compile the complete, well-structured answer.
Lens-Related Glaucoma
Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition (pp. 393-394)
Kanski classifies lens-related glaucoma into three distinct entities:
- Phacolytic glaucoma
- Phacomorphic glaucoma
- Pupillary block from disruption of lens position
1. Phacolytic Glaucoma
Pathogenesis
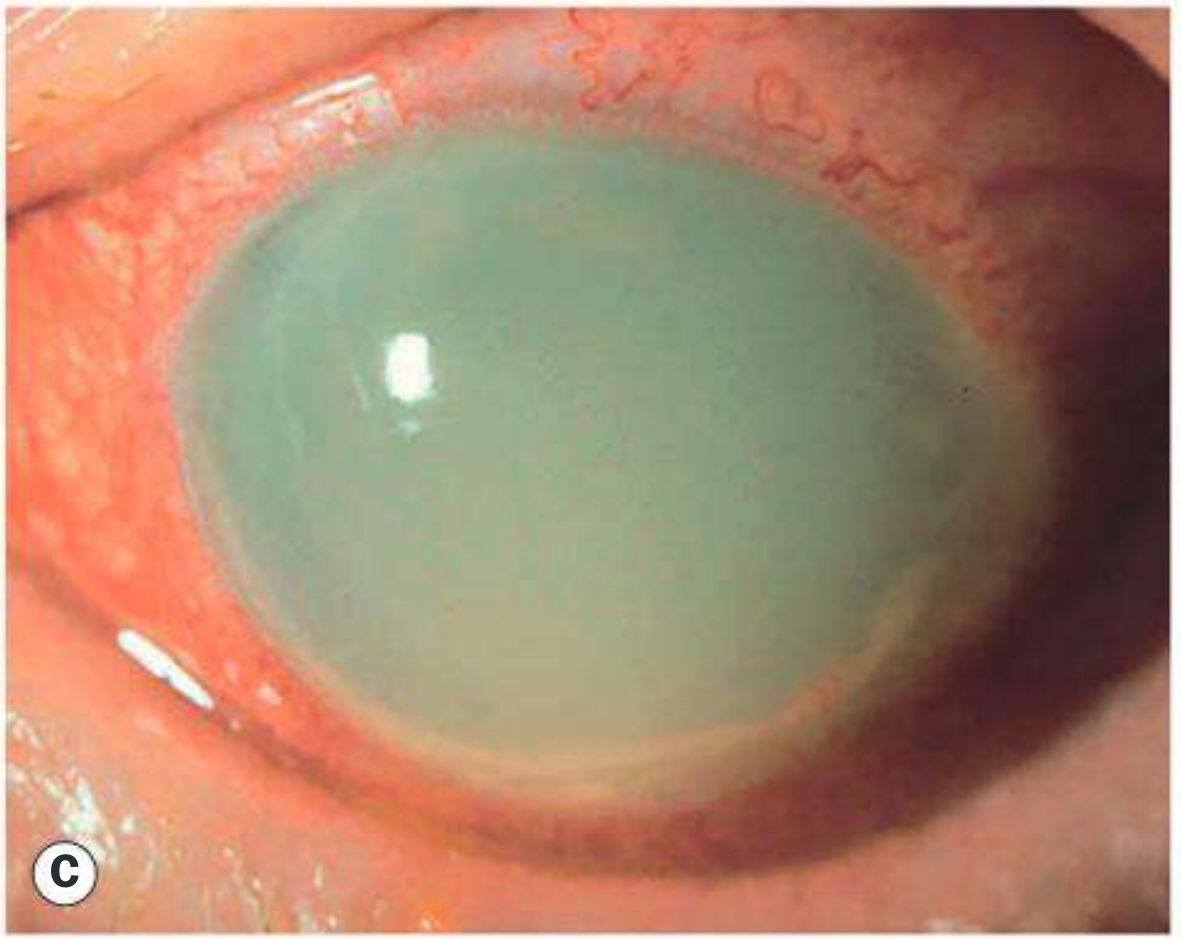
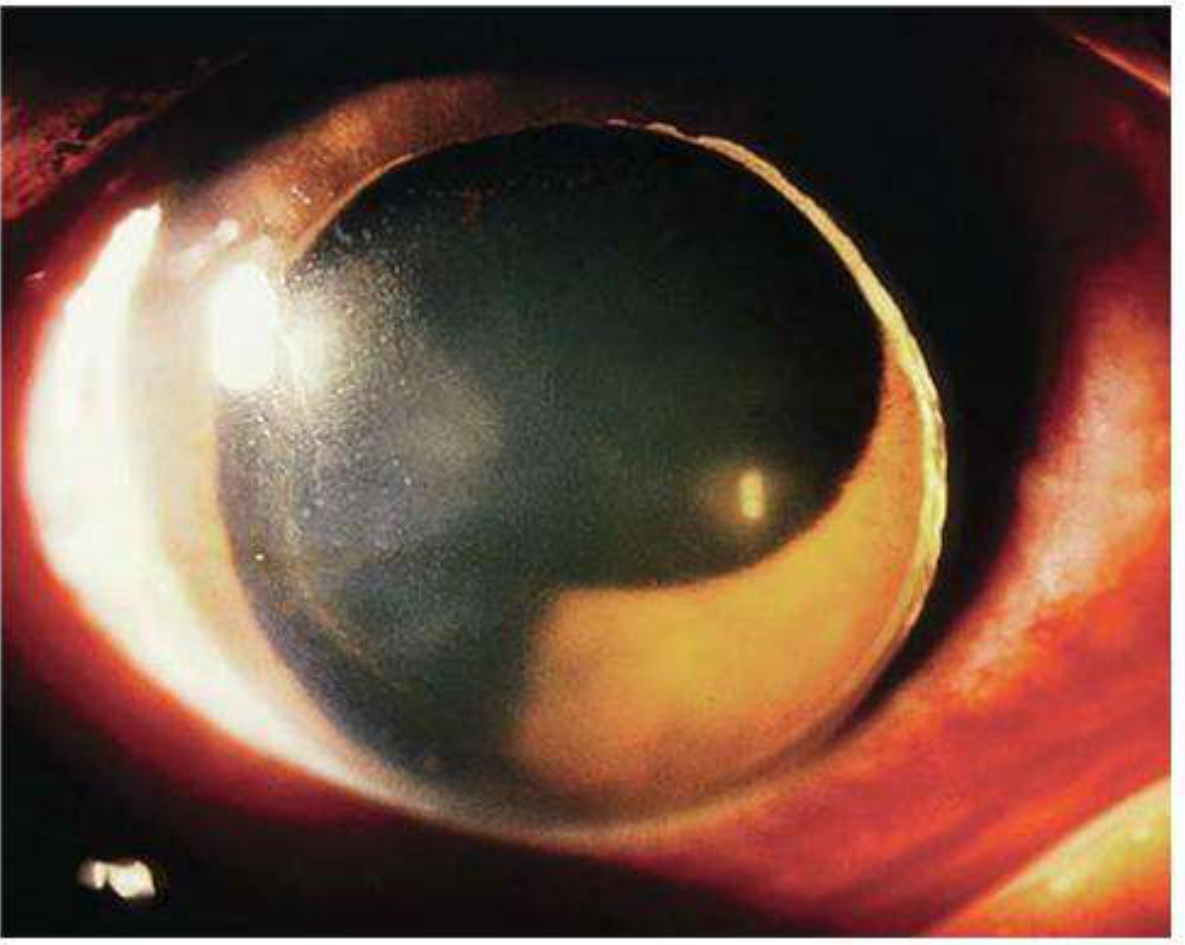
Phacolytic glaucoma is a secondary open-angle glaucoma occurring in association with a hypermature cataract. High molecular-weight lens proteins leak through the intact capsule into the aqueous humour, causing trabecular obstruction. Macrophages that have engulfed these lens proteins may also contribute to the blockage.
Important distinction: Phacolytic glaucoma must NOT be confused with phacogenic (phacoanaphylactic) uveitis, which is an autoimmune granulomatous reaction to exposed lens proteins occurring when the capsule is compromised (not intact).
Diagnosis
- Symptoms: Pain; poor vision due to cataract
- Slit lamp findings:
- Corneal oedema
- Hypermature cataract with a deep anterior chamber
- Large floating white particles in the AC (lens protein + protein-containing macrophages)
- Dense milky aqueous if particles are very abundant
- Pseudohypopyon may form (Fig. 11.48C and D)
- Gonioscopy: Open angle with lens-derived material and inflammatory cells, most prominent inferiorly
Treatment
- Medical IOP control first (to reduce inflammation and corneal oedema)
- Wash out proteinaceous material from the AC
- Cataract extraction (definitive treatment)
- Note: The zonule is likely more fragile than usual - handle with care during surgery
2. Phacomorphic Glaucoma
Pathogenesis
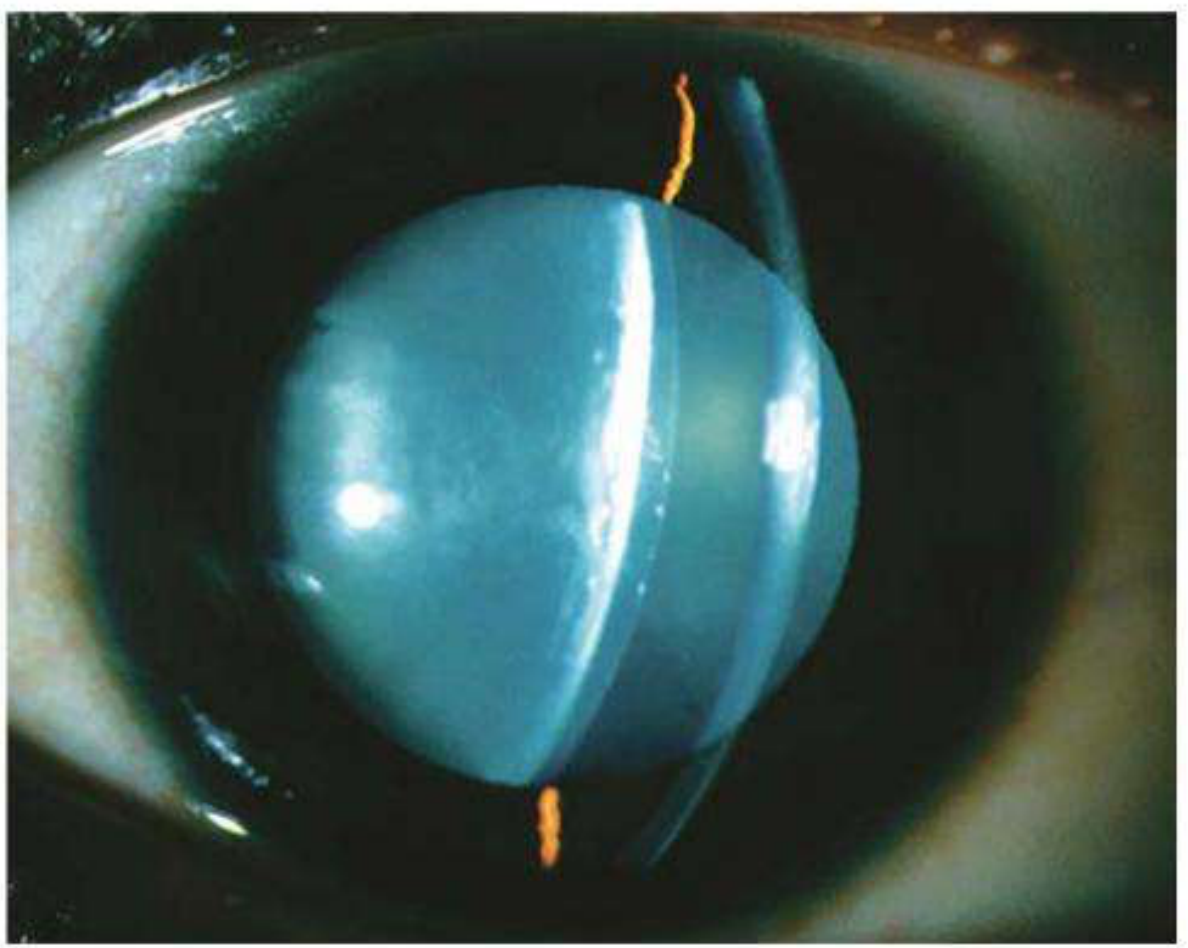
Phacomorphic glaucoma is an acute secondary angle-closure glaucoma precipitated by an intumescent (swollen) cataractous lens. The mechanism is:
- Equatorial age-related lens growth slackens the suspensory ligament → lens moves anteriorly
- Anteroposterior growth increases iridolenticular contact
- This potentiates pupillary block and iris bombé
Diagnosis
- Presentation similar to acute primary angle-closure glaucoma (PACG): shallow AC and mid-dilated pupil
- A dense white (intumescent) cataract is evident
- Fellow eye: More likely in eyes with shorter axial length and shallower AC; the fellow eye may paradoxically show a deep AC and open angle
- Anterior segment OCT or US biomicroscopy may be useful
Treatment
- Medical treatment initially similar to acute PACG
- Miotics are OMITTED - they increase iris-lens apposition and shift the lens anteriorly
- Dilatation may be helpful but should be used with caution
- Systemic hyperosmotic agents may be required more commonly than in PACG
- Laser iridotomy - may be worthwhile but often not possible (corneal oedema or lens-cornea proximity) or ineffective
- Laser iridoplasty - useful temporizing measure
- Cataract extraction - definitive treatment, ideally after IOP is normalized and the eye is quiet
- Surgery is difficult and carries a higher risk of complications
- Consider a similar prophylactic procedure for the fellow eye
3. Pupillary Block from Disruption of Lens Position
Causes
- Blunt ocular trauma (even relatively trivial)
- Congenitally small lens (microspherophakia), e.g., Weill-Marchesani syndrome
Pathogenesis
- Dislocation may be into the AC
- Zonules may be stretched, or only partial disruption with the intact part acting as a hinge
- The lens may remain fully or partially in the posterior chamber
- Vitreous herniation may be contributory
Diagnosis
- A lens fully or partially dislocated into the anterior chamber is usually evident on slit lamp
- Acute pupillary block causes sudden severe IOP elevation with visual impairment
- Ultrasound biomicroscopy is often diagnostic
Treatment
This is an ophthalmic emergency - prolonged lenticular corneal contact, especially with high IOP, can cause permanent endothelial damage.
- IOP reduction with osmotic agents (reduce vitreous volume) - urgent
- Initial repositioning attempt: Patient adopts supine posture with pupil dilated → attempt to reposition lens in posterior chamber → miotic can then be used with caution
- Bilateral laser iridotomy may provide extended control in some cases
- Definitive treatment: Surgical lens extraction
- An anterior chamber IOL, iris-fixated IOL, or sclera-fixated IOL will be necessary
Summary Comparison Table
| Feature | Phacolytic | Phacomorphic | Pupillary Block (Dislocation) |
|---|---|---|---|
| Type | Secondary open-angle | Secondary angle-closure | Secondary angle-closure |
| Lens status | Hypermature (intact capsule) | Intumescent cataract | Dislocated/subluxated |
| AC depth | Deep | Shallow | Variable |
| Mechanism | Lens protein + macrophage trabecular blockage | Pupillary block/iris bombé from swollen lens | Direct pupillary block by displaced lens |
| Key finding | Floating white particles, pseudohypopyon | Dense white cataract, iris bombé | Visible dislocation on slit lamp |
| Definitive Rx | Cataract extraction | Cataract extraction | Surgical lens extraction + IOL |
| Special caution | Fragile zonules at surgery | Avoid miotics | Urgent - risk of corneal endothelial damage |
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition, pp. 393-394
Treatment for snake bite
Reading File
Finding Sources
Finding Sources
Searching PubMed
snakebite envenomation treatment management
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from both Tintinalli's Emergency Medicine and Sabiston's Surgery. Let me compile the full, authoritative answer.
Treatment of Snakebite
Sources: Tintinalli's Emergency Medicine (Comprehensive Study Guide) & Sabiston Textbook of Surgery, 7th Edition
Overview
Venomous snakebites are a medical emergency. Mortality with modern treatment is <0.5% (compared to ~25% historically), largely due to antivenom availability and advances in critical care. Venomous snakes fall into two major groups:
| Group | Examples | Venom Type | Predominant Injury |
|---|---|---|---|
| Crotalinae (Pit Vipers) | Rattlesnakes, copperheads, water moccasins | Cytotoxic, hemotoxic | Local tissue necrosis + coagulopathy |
| Elapidae (Coral snakes, cobras, mambas) | Coral snake, king cobra, mamba | Neurotoxin | Neuromuscular paralysis |
Up to 25% of crotaline bites are "dry bites" - no venom is injected.
STEP 1: First Aid / Pre-Hospital
DO these:
- Remove jewelry and tight clothing from the affected extremity (anticipate swelling)
- Immobilize and splint the limb in a functional position (reduces discomfort; may slow venom spread)
- Limit exertion - especially walking for lower extremity bites
- Transport to a specialized centre with snakebite experience as soon as possible
- Do NOT wash the bite wound if in Australia/PNG - a venom identification swab kit may be used
DO NOT do these (historical treatments to AVOID):
- No incision and suction - not recommended since 1980; only tiny amounts of venom extracted and risk of injury to vessels/tendons/nerves
- No ice or cryotherapy - associated with a high rate of amputation
- No tourniquets or ligation
- No massage of the wound
- No electrical current (some have tried outboard motor generators - ineffective and dangerous)
Pressure bandage / constrictor band is species-specific:
- Elapid bites (neurotoxic - e.g., Australia, coral snakes): Apply pressure bandage between wound and heart at ~55 mmHg - shown to reduce systemic toxicity
- Crotalid bites (US pit vipers): Constrictor band concentrates venom locally → increased necrosis - DO NOT use
STEP 2: Emergency Department Assessment
History and Identification
- Do not risk a second bite to catch the snake; do not handle dead snakes (reflexive bites possible)
- Contact regional poison control for identification, expected toxicity, and antivenom location
- Document time of bite, species if known, first aid given
Clinical Assessment
Local signs:
- Pain, edema, erythema at bite site
- Distance between fang marks correlates with snake size
- Mark the advancing border of edema with a pen every 30 minutes
Systemic signs:
- Muscle twitching, perioral paresthesias, metallic taste
- Crotalid: hypovolemia, coagulopathy, hemolysis
- Elapid: confusion, muscle spasm, nausea/vomiting, blurred vision, speech difficulty, respiratory failure
Investigations
- CBC, coagulation profile (PT, aPTT, fibrinogen), blood type and crossmatch
- Metabolic panel, renal function
- Repeat labs every 4 hours or after each antivenom course
STEP 3: Antivenom - The Definitive Treatment
Antivenom is the cornerstone of treatment. Administer in a critical care setting (ED or ICU) under direct physician supervision with resuscitative drugs (including epinephrine) and equipment immediately available.
Indications for Antivenom
- Any evidence of local envenomation
- Worsening significant thrombocytopenia (<100,000/μL) or hypofibrinogenemia (<100 mg/dL)
- Progressive edema despite initial treatment
- Systemic envenomation signs
Crotalid (Pit Viper) Antivenom
- FabAV (Crotalidae Polyvalent Immune Fab, Ovine) or equivalent
- Goal: establish initial control = cessation of progression of all components - local effects, systemic effects, and coagulopathy
- Additional doses if condition worsens
- FabAV is also effective for copperhead envenomation where progression occurs
- Measure limb circumference at multiple sites above and below bite every 30 minutes as guide
Elapid (Coral Snake) Antivenom
- Neurotoxicity onset: immediate (15-30 min for mamba/Australian brown snake) or delayed (2-5 hours for coral snakes)
- No longer any antivenom available for North American coral snakes - local zoos and other countries may help for exotic species
- Neurotoxic symptoms: confusion, muscle spasm, respiratory failure, cranial nerve palsies
Antivenom Reactions
- Incidence of acute reactions to modern antivenoms is low
- If allergic reaction occurs: stop infusion immediately, administer H1 and H2 antihistamines, have epinephrine ready for anaphylaxis
STEP 4: Supportive Care
- Fluid resuscitation with isotonic fluids for hypovolemia; vasopressors for refractory hypotension
- Blood component replacement (only if active bleeding AND after antivenom has been given - antivenom is the best treatment for hematologic abnormalities)
- Wound care: clean wound, tetanus prophylaxis
- Pain management
STEP 5: Compartment Syndrome Management
A critical complication - venom injected directly into a compartment causes increased pressure.
| Step | Action |
|---|---|
| 1 | Measure intracompartmental pressure |
| 2 | If not elevated: continue standard management |
| 3 | If signs present AND pressure >30 mmHg: elevate limb + mannitol 1-2 g/kg IV over 30 min + additional antivenom over 60 min simultaneously |
| 4 | If elevated pressure persists another 60 min: consider fasciotomy |
Key principle: The most effective treatment for snakebite-associated compartment syndrome is neutralizing the venom with antivenom - not fasciotomy. Antivenom reduces compartment pressure. Prophylactic fasciotomy has no role. Fasciotomy may actually increase severity of local tissue loss.
STEP 6: Surgical Considerations (Crotalid)
- Wound debridement may be required for necrotic tissue
- Fasciotomy only when compartment pressures do not respond to antivenom and mannitol
- Post-fasciotomy: consider negative-pressure wound therapy
- Do NOT do elective early debridement of tissue that may be salvageable with antivenom
Summary Algorithm
Snakebite
↓
First Aid: Remove jewelry, immobilize, limit exertion
↓
Transport to ER → Identify snake type, call poison control
↓
Assess: Local + systemic signs, serial labs
↓
Dry bite (no signs)? Yes → Observe 8-12h, discharge if no progression
↓ No
Antivenom (species-specific) → critical care setting
↓
Monitor progression (mark edema, serial labs every 4h)
↓
Compartment syndrome? → Mannitol + more antivenom → Fasciotomy if unresponsive
↓
Supportive: Fluids, vasopressors, blood products if needed
Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Ch. 212 | Sabiston Textbook of Surgery, 7th Ed. - Ch. 44
This is a shared conversation. Sign in to Orris to start your own chat.