How fungal ball is different from fungal sinusitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fungal sinusitis" classification "fungal ball"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content from Scott-Brown's and KJ Lee's. Let me compile the full answer.
Fungal Ball vs. Fungal Sinusitis
Fungal sinusitis is the broad umbrella term for all forms of fungal infection of the paranasal sinuses. Fungal ball (also called mycetoma or aspergilloma) is one specific subtype within that classification. The entire classification splits into invasive vs. non-invasive disease, and fungal ball falls under non-invasive.
The Classification of Fungal Sinusitis
According to Scott-Brown's Otorhinolaryngology, fungal rhinosinusitis is classified into 3 invasive and 2 non-invasive subgroups:
| Non-Invasive | Non-Invasive | Invasive | Invasive | Invasive | |
|---|---|---|---|---|---|
| Fungal Ball (Mycetoma) | Allergic Fungal Sinusitis | Acute Invasive | Chronic Invasive | Chronic Granulomatous Invasive | |
| Pathogen | Aspergillus spp., Pseudallescheria boydii | Bipolaris, Alternaria, Curvularia, Aspergillus | Mucormycosis (diabetics); Aspergillus fumigatus (immunocompromised) | A. flavum, A. fumigatus | A. flavum |
| Host immune status | Immunocompetent | Atopic (IgE-mediated) | Immunocompromised | Immunocompetent or mildly compromised | Immunocompetent |
| Geography | Humid areas | Humid areas (e.g. Mississippi basin) | Non-specific | Non-specific | North Africa (Sudan), South Asia |
| Tissue invasion | No | No | Yes | Yes | Yes |
(Table 21.1 - Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1)
What Defines a Fungal Ball Specifically?
A fungal ball is a dense amalgamation (conglomeration) of fungal hyphae within the sinus cavity, without any invasion of the mucosal tissue.
Key features:
Pathology:
- Densely packed, septate fungal hyphae (dematiaceous or hyaline molds)
- Non-specific chronic inflammatory changes in the surrounding mucosa
- Critically: no fungal invasion into mucosa, submucosa, bone, or vessels - this is the histopathological hallmark that distinguishes it from all invasive forms
- The underlying sinus mucosa appears edematous and inflamed but intact
Clinical:
- Occurs almost exclusively in immunocompetent patients
- Most common sinus: maxillary >> sphenoid >> ethmoid >> frontal
- Often asymptomatic - incidentally found on CT or dental X-ray
- When symptomatic: cheek pressure/fullness, nasal drainage, retro-orbital pressure (if sphenoid)
- Endoscopy shows gritty, chalky, "clay-like" or "cheesy" debris - distinctly characteristic
Imaging (CT - the study of choice):
- Hyperdense foci within an opacified sinus (due to calcium and heavy metal deposits from fungal metabolism)
- Multifocal hyperdensities are more specific for the diagnosis
- Sinus wall thickening and hyperostosis - NOT the expansile bone erosion seen in AFS
- Usually unilateral, single sinus
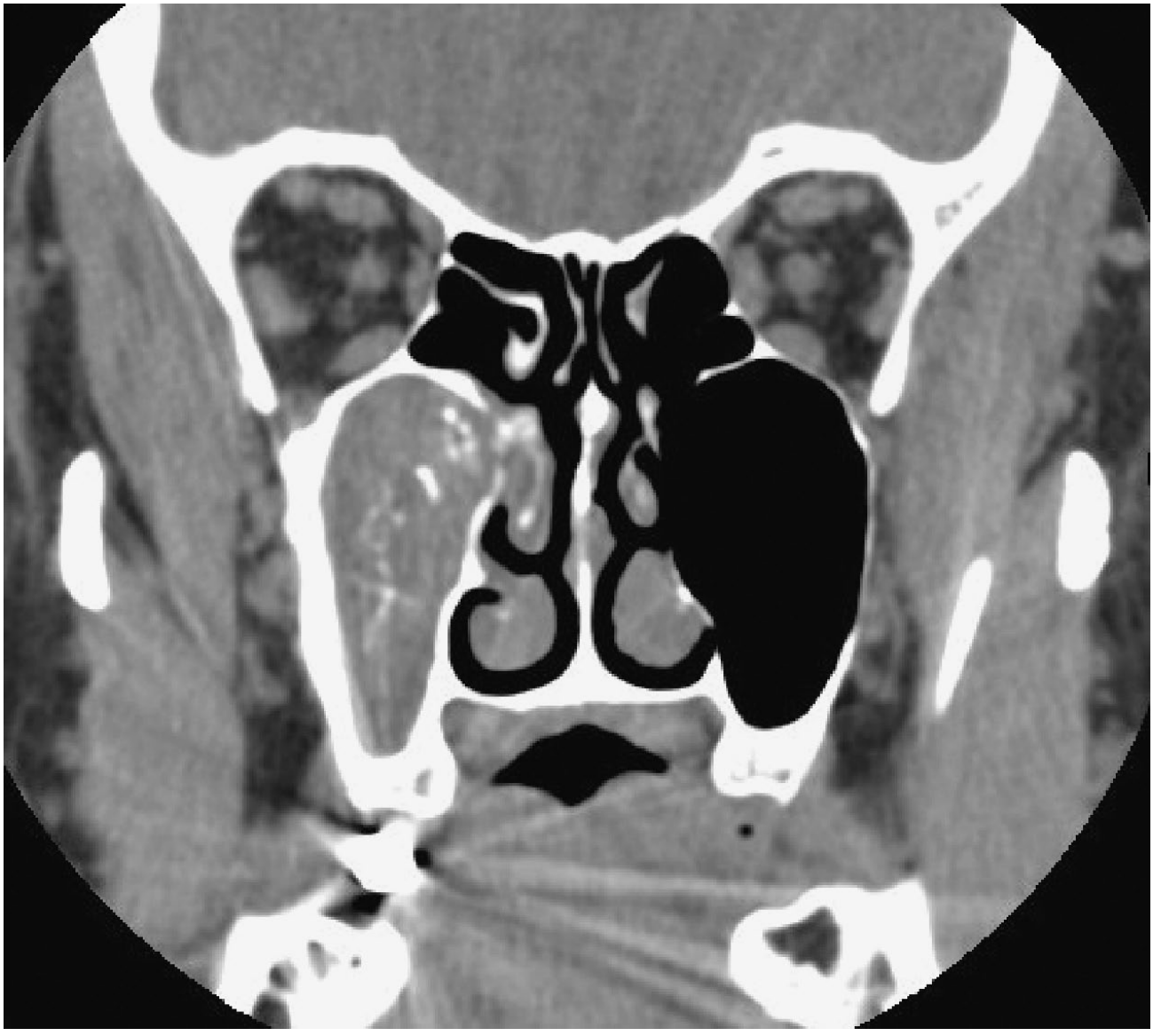
Coronal CT of a right maxillary fungal ball showing the characteristic multifocal hyperdensities within an opacified sinus (K.J. Lee's Essential Otolaryngology)
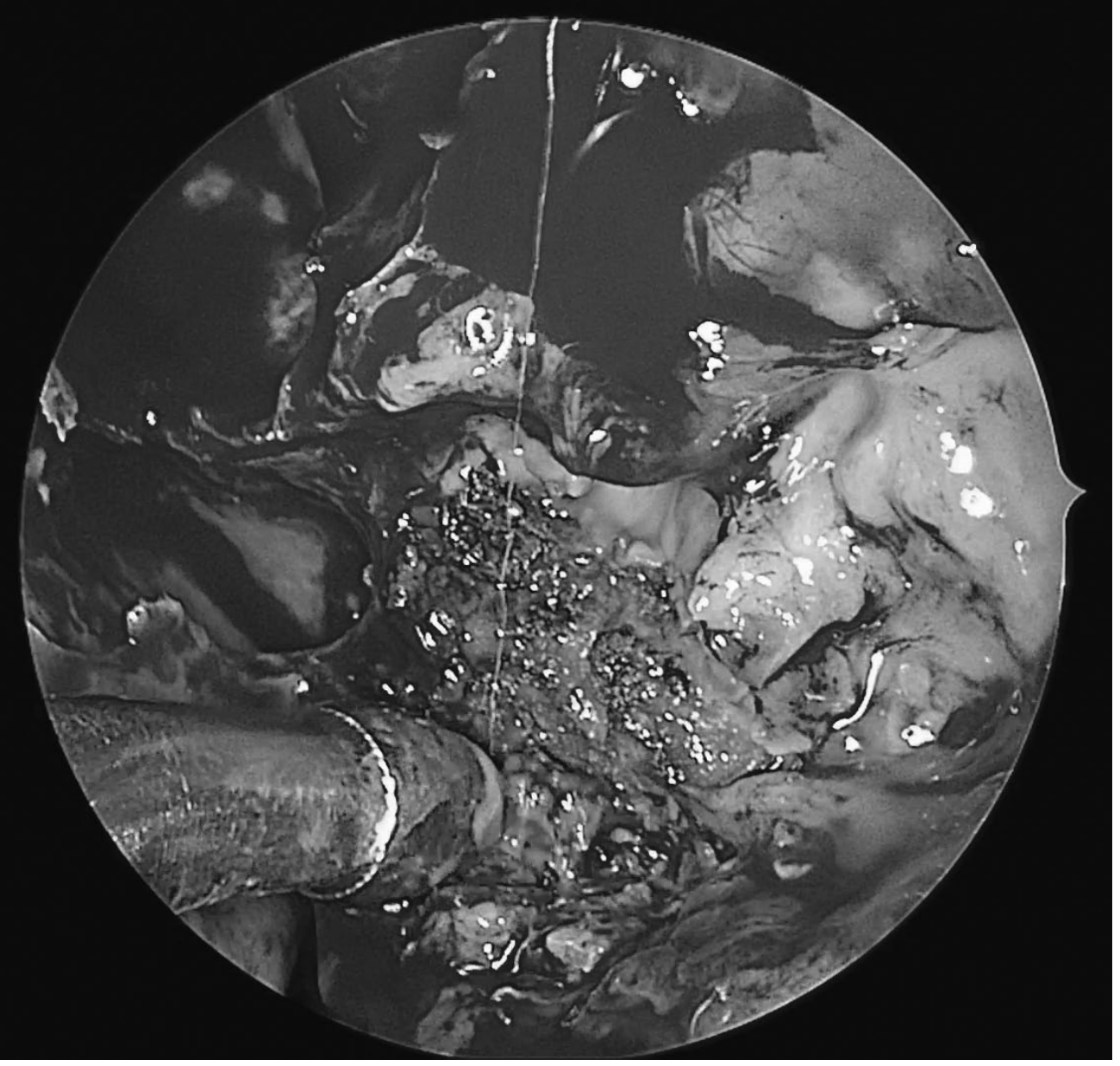
Intraoperative endoscopy of a fungal ball: dense, chalky discrete balls of fungal elements with purulent debris (K.J. Lee's)
Treatment:
- Surgery alone (FESS - functional endoscopic sinus surgery) is the mainstay
- Goals: confirm diagnosis, complete extirpation of fungal debris, and wide ostial patency for postoperative irrigation
- Antifungals are NOT effective and not necessary - the ball is non-invasive, so systemic or topical antifungals do not penetrate the mass
- Recurrence is uncommon after thorough surgery
- Even asymptomatic cases generally warrant surgery due to risk of secondary infection and rare progression to invasive disease in immunocompromised patients
How Each Form of Fungal Sinusitis Differs
1. Allergic Fungal Sinusitis (AFS) - also non-invasive, but very different from fungal ball
| Feature | Fungal Ball | Allergic Fungal Sinusitis |
|---|---|---|
| Mechanism | Direct fungal colonization, no immune reaction | IgE-mediated hypersensitivity to fungal antigen |
| Host | Immunocompetent (no atopy needed) | Atopic/allergic individuals |
| Distribution | Single sinus (usually unilateral) | Multiple sinuses, often bilateral |
| Hallmark finding | Dense hyphal mass | "Allergic mucin" (eosinophilic mucin with Charcot-Leyden crystals) |
| Polyps | Absent | Nasal polyposis is a prominent feature |
| CT appearance | Hyperdense ball-like focus, wall hyperostosis | Heterogeneous opacification, sinus expansion, bone erosion/remodeling |
| Antifungals | Not useful | Adjunct role (topical/systemic debated) |
| Steroids | Not needed | Systemic steroids are a key part of treatment |
| Recurrence | Low after surgery | High - "known for its high recidivism" |
2. Acute Invasive Fungal Sinusitis (AIFS) - the most dangerous
- Only in severely immunocompromised (neutropenia, hematologic malignancy, DKA/DM)
- Fungi invade through vessels and nerves causing vessel thrombosis and mucosal necrosis
- Rapidly progressive and fatal within days; mortality ≥ 50%
- CT: "black turbinate" sign on MRI (non-enhancing devitalized tissue), subtle bone erosion, extra-sinus soft tissue extension
- Treatment: urgent surgical debridement + IV antifungals (amphotericin B) + reverse immunosuppression
3. Chronic Invasive Fungal Sinusitis
- Patients are immunocompetent or mildly immunocompromised (e.g. diabetics)
- Slow progression over >4 weeks
- Homogeneous soft tissue opacification on CT, limited bony erosion only at points of extra-sinus extension
- Treatment: surgical debridement + antifungal therapy
4. Chronic Granulomatous Invasive Fungal Sinusitis
- Immunocompetent hosts; mainly in North Africa and South Asia
- Caused exclusively by Aspergillus flavum
- Forms granulomas with giant cells on histology
- Disease burden often more outside the sinuses (intra-orbital) than within
Core Principle: The Defining Difference
Invasive fungal disease = hyphae within mucosa, submucosa, bone, blood vessels, or nerves. Non-invasive disease (fungal ball and AFS) = colonization of the surface without tissue penetration.
The fungal ball is essentially a passive accumulation of fungus in a sinus cavity - the fungus is contained, not invading. The invasive forms are life-threatening because the fungus actively destroys tissue. AFS sits in an odd middle ground - non-invasive histologically, yet can cause bone destruction through immune-mediated pressure and expansion.
Clinical bottom line: A patient presenting with a hyperdense maxillary sinus mass on CT, intact immunity, and gritty debris on endoscopy almost certainly has a fungal ball - manage with FESS, no antifungals needed. If the same patient is neutropenic or diabetic with DKA and has a black, necrotic middle turbinate, treat as acute invasive fungal sinusitis - a surgical and medical emergency.
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, Table 21.1; K.J. Lee's Essential Otolaryngology, Chapter 30
What are the diagnostic criteria for confirming fungal ball on histology?
Finding Sources
Finding Sources
Searching PubMed
"fungal ball" sinusitis histology diagnosis criteria
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have a complete picture from multiple authoritative sources. Here is the full answer:
Histological Diagnostic Criteria for Fungal Ball
The histological diagnosis of a fungal ball rests on a combination of positive findings (what is present) and negative findings (what must be absent). The criteria were formally defined by DeShazo et al. and are consistently cited across ENT textbooks.
The DeShazo Criteria (Formal Diagnostic Definition)
(Scott-Brown's Otorhinolaryngology, Table 21.1 / Definition section)
A fungal ball is confirmed histologically when ALL of the following are met:
Positive criteria (must be present):
- Dense mass of tightly packed fungal hyphae within the sinus lumen - the central defining feature
- Extramucosal location - the hyphal mass sits in the sinus cavity and separates easily from the underlying sinus mucosa
- Non-specific chronic inflammatory changes in the sinus mucosa (lymphocytes, plasma cells - a generic inflammatory backdrop)
Negative criteria (must be absent - each exclusion rules out a rival diagnosis):
| What must be ABSENT | What it would diagnose instead if present |
|---|---|
| No fungal invasion of mucosa, submucosa, vessels, or bone | Invasive fungal sinusitis (any form) |
| No eosinophil predominance in the mucosa or mucin | Allergic fungal rhinosinusitis (AFS) |
| No eosinophilic mucin (no "allergic mucin") | AFS |
| No Charcot-Leyden crystals | AFS |
| No granuloma formation | Chronic granulomatous invasive fungal sinusitis |
| No allergic mucin in the sinus contents | AFS |
"The mucosa may show non-specific inflammation, but in particular there is an absence of invasion by fungal elements, or granulomatous reaction." - Scott-Brown's Vol. 1
Macroscopic / Gross Appearance
Before microscopy, the gross specimen provides strong diagnostic clues:
- The mass is cheesy, clay-like, or rubbery in consistency
- Color is green, yellow, brown, or black
- The ball separates easily from the underlying mucosa - it is not adherent or invasive
- The underlying mucosa may be normal or hypertrophic, but is intact and not necrotic
Microscopic Features in Detail
Low-power view:
- Densely packed hyphae filling the sinus lumen
- "Onion-skin" layering - alternating zones of dense and less-dense hyphal growth creating concentric laminar rings (a characteristic low-power pattern)
- Inflammatory cell infiltrate within the hyphal mass (cell debris, inflammatory exudate)
High-power view:
- Hyphae are typically septate, with dichotomous branching at ~45°(when Aspergillus)
- Hyphae are extramucosal only - the mucosal epithelium is the boundary; no hyphae cross into the lamina propria, blood vessel walls, or bone
- The surrounding mucosa shows chronic non-specific inflammation without tissue necrosis
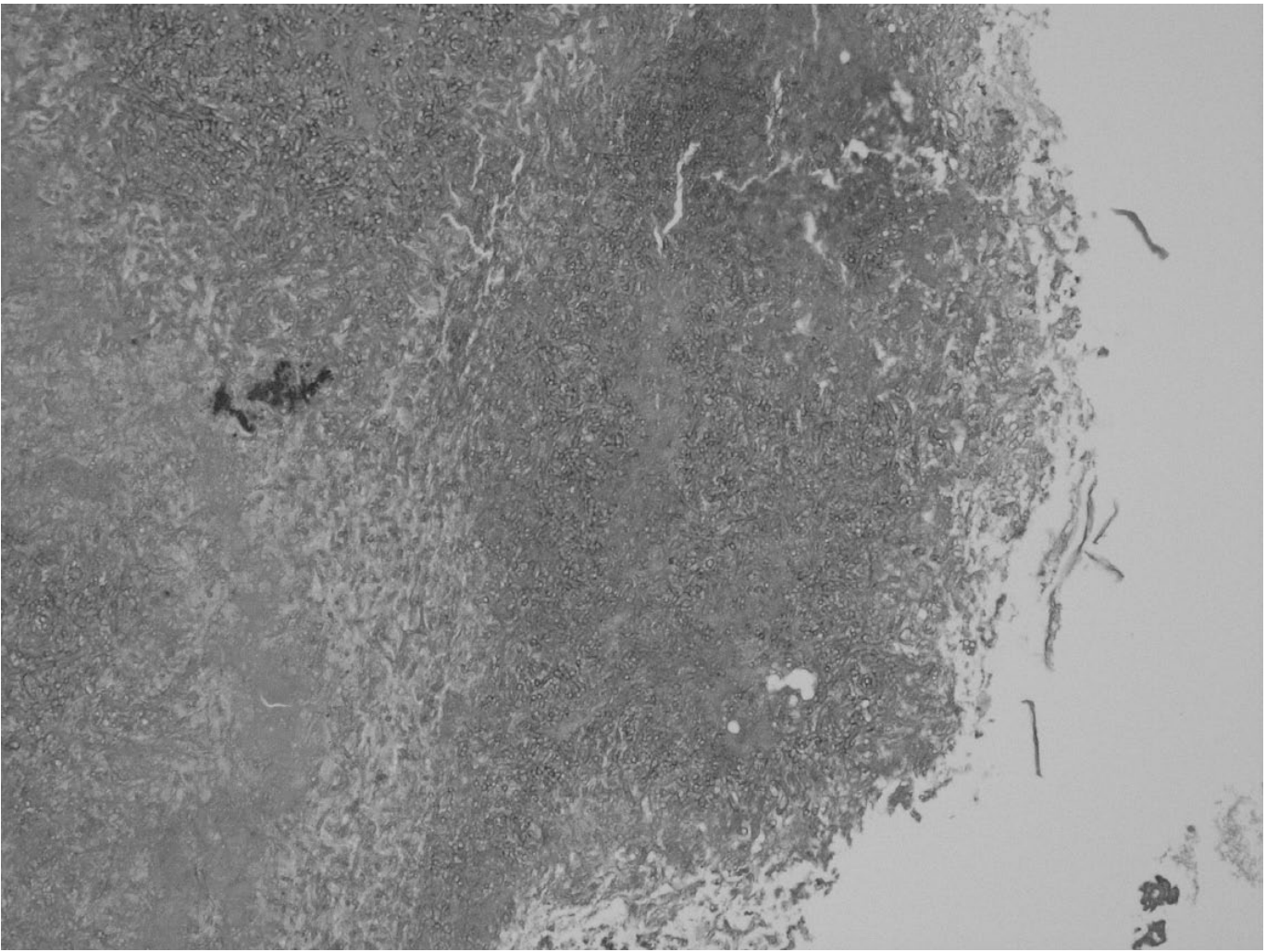
Microscopy of a fungal ball showing tightly packed hyphae with inflammatory exudates and cell debris. Fungal invasion into tissue is not seen - the critical histological feature. (K.J. Lee's Essential Otolaryngology)
Staining Techniques
| Stain | Purpose |
|---|---|
| H&E (Haematoxylin & Eosin) | Aspergillus hyphae often visible; good for evaluating mucosal inflammation and confirming absence of eosinophilic mucin, granulomas, and invasion |
| Silver impregnation stains (GMS - Gomori Methenamine Silver; or PAS - Periodic Acid-Schiff) | Mandatory for all samples; highlights fungal cell walls in black (GMS) or magenta (PAS), allowing confident identification of hyphae that may be faint on H&E |
| Culture | Needed to identify the species, but has a low yield (~50%) since many fungal balls culture negative - histology alone is sufficient for diagnosis |
"All samples, including mucosa and fungal samples, should be stained with silver impregnation stains in order to identify the presence of fungi." - Scott-Brown's Vol. 1
An important practical point: two separate specimens should be sent - one from the fungal ball contents itself, and one mucosal biopsy from the sinus wall - to confirm both the presence of fungal elements and the absence of mucosal invasion.
How Histology Distinguishes Fungal Ball from Other Forms
| Fungal Ball | AFS | Acute Invasive | Chronic Invasive | Chronic Granulomatous | |
|---|---|---|---|---|---|
| Hyphae present | Yes (extramucosal mass) | Yes (in eosinophilic mucin) | Yes (in tissue) | Yes (in tissue) | Yes (in tissue) |
| Tissue invasion | No | No | Yes - vessels, nerves, necrosis | Yes - slow | Yes - granulomatous |
| Eosinophilic mucin | Absent | Present | Absent | Absent | Absent |
| Charcot-Leyden crystals | Absent | Present | Absent | Absent | Absent |
| Granuloma | Absent | Absent | Absent | Absent | Present (giant cells) |
| Necrosis | Absent | Absent | Present | May be present | Present |
| Eosinophil predominance | Absent | Present | Absent | Absent | Absent |
Summary Statement
The histological diagnosis of fungal ball requires: (1) a dense extramucosal mass of packed hyphae that separates from the mucosa; (2) no invasion of mucosal tissue, vessels, or bone on silver-stained sections; and (3) absence of eosinophilic mucin, Charcot-Leyden crystals, and granulomas.** Harrison's (2025) states it plainly: "No tissue invasion is demonstrable histologically or radiologically." The negative criteria are just as important as the positive ones - their absence differentiates fungal ball from AFS and from all invasive forms.
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (DeShazo criteria); K.J. Lee's Essential Otolaryngology Ch. 30; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.