Post Herpes zoster opthalmicus management for pain and itching
Reading File
Finding Sources
Finding Sources
Searching PubMed
postherpetic neuralgia treatment pain management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching the Web
post herpes zoster ophthalmicus postherpetic itch pruritus management treatment 2024
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Post-Herpes Zoster Ophthalmicus: Management of Pain and Itching
Background: HZO involves reactivation of varicella-zoster virus (VZV) in the ophthalmic division (V1) of the trigeminal nerve. The two most distressing post-acute sequelae are postherpetic neuralgia (PHN) and postherpetic itch/pruritus - both neuropathic phenomena arising from peripheral nerve and dorsal root ganglion damage.
Postherpetic Neuralgia (PHN) - Definition & Epidemiology
PHN is defined as pain persisting for more than one month after the rash has healed. It develops in up to 75% of patients over 70 years of age. The pain may be:
- Constant or intermittent
- Burning, stabbing, itching, or aching in character
- Worse at night
- Aggravated by minor stimuli (allodynia - pain from light touch or heat)
PHN generally improves over time, with only ~2% of patients still affected after 5 years. However, it can be severely debilitating, with risk of depression and social withdrawal. - Kanski's Clinical Ophthalmology, 10th ed.
PAIN MANAGEMENT
Step 1 - Prevention (Early Antiviral Therapy)
Starting antivirals within 72 hours of rash onset is the most effective strategy to reduce PHN risk:
- Valacyclovir 1 g TDS x 7-10 days (preferred - better bioavailability, convenient dosing)
- Famciclovir 500 mg TDS x 7-10 days
- Acyclovir 800 mg five times daily x 7-10 days (older regimen, still effective)
Early gabapentin added to valacyclovir during acute HZO (in patients with moderate-to-severe pain) was shown in one open study to be more effective in preventing PHN than valacyclovir alone - this combination is recommended for that subset of patients. - Dermatology 2-Volume Set, 5th ed.
Note: Adding systemic steroids (prednisone/prednisolone) reduces acute pain and speeds skin healing but does not reduce the incidence or severity of PHN in controlled trials. It remains useful for neurological complications.
Step 2 - Acute Phase Pain (during active disease)
| Treatment | Detail |
|---|---|
| Cool compresses | Simple, safe, provides immediate relief |
| Bacitracin/erythromycin ointment | On skin lesions to prevent secondary infection |
| Simple analgesics | Paracetamol/acetaminophen (regular dosing schedule preferred over as-needed) |
| Stronger analgesics | Codeine or NSAIDs for moderate pain |
| Opioids | For severe acute-phase pain; short-term use |
| Topical cycloplegics | Cyclopentolate 1% TDS for significant ocular pain from iritis |
| Topical steroids | Prednisolone acetate 1% for iritis (ophthalmologist consultation first) |
| Calamine lotion | On open lesions to reduce acute pain AND pruritus |
Important: Topical anaesthetics (e.g. tetracaine eye drops) must never be prescribed for self-use due to corneal toxicity. - AAFP Guidelines
Step 3 - Established PHN (Systemic Stepped Therapy)
Treatment is staged from least to most potent:
First-line agents (all with good RCT evidence, FDA-approved for PHN):
| Drug | Dose | Notes |
|---|---|---|
| Gabapentin | 300-600 mg up to TDS (titrate) | 50% pain reduction may take 2-3 months of titration; most commonly used |
| Pregabalin | Titrated (start 75 mg BD) | FDA-approved for PHN; faster titration than gabapentin |
| Tricyclic antidepressants - Nortriptyline or Amitriptyline | 25 mg nocte, titrate up to 75 mg | Combined with gabapentin is more effective than either alone (RCT evidence); poorly tolerated in elderly (confusion, sedation, urinary retention, cardiotoxicity) |
Second-line agents:
| Drug | Dose | Notes |
|---|---|---|
| Lidocaine 5% patch | Apply to affected area | Topical; provides ~8 hours of relief in controlled trial |
| Capsaicin 0.075% cream | Apply after lesions crust | Low-strength cream has limited evidence; applied after crusting, not on open lesions |
| Capsaicin 8% patch | Single 1-hour application | Reduces PHN pain for up to 12 weeks; ~1/3 of patients cannot tolerate transient burn |
| Opioids - Sustained-release oxycodone | 10-30 mg BD | For refractory cases; use cautiously |
| Carbamazepine | 400 mg daily | Specifically for lancinating (electric shock-like) pain |
Other agents:
- EMLA cream (lidocaine/prilocaine 2.5%/2.5%) - topical option for allodynia
- SNRIs (duloxetine) - used in neuropathic pain protocols where TCAs not tolerated
- Nerve blocks - stellate ganglion or trigeminal nerve blocks for refractory cases
- Biofeedback and non-pharmacological approaches
Combined nortriptyline + gabapentin was shown in a RCT to reduce pain more than either agent alone. - Dermatology 2-Volume Set, 5th ed.
ITCH (Postherpetic Pruritus) MANAGEMENT
Postherpetic itch is a neuropathic phenomenon - it represents aberrant afferent C-fiber signaling in the same damaged neural pathways that cause pain. In HZO, it is typically felt in the periorbital/forehead dermatomal distribution.
Topical agents:
- Calamine lotion - applied to open/crusted lesions; reduces both pain and pruritus during acute phase
- Capsaicin cream (0.075%) - depletes substance P from sensory nerve endings; applied once lesions are fully crusted; reduces neuropathic itch
- Lidocaine 5% patch - effective for both pain and itch via Na-channel blockade
- Menthol-containing preparations - counter-irritant effect (TRPM8 activation) can reduce itch perception
Systemic agents:
- Gabapentin/Pregabalin - first-line for neuropathic itch, same as for PHN pain
- Tricyclic antidepressants (amitriptyline/nortriptyline) - also effective for neuropathic pruritus
- Antihistamines (hydroxyzine, cetirizine) - limited efficacy for neuropathic itch (this is not histamine-mediated), but sedating antihistamines (hydroxyzine) can help at night via sedative + mild anti-pruritic effect
- Low-dose naltrexone - emerging evidence for neuropathic itch (off-label)
Non-pharmacological:
- Cool/cold compresses over the affected area
- Avoiding heat and friction to the periorbital skin
Summary Algorithm
POST-HZO PAIN & ITCH
ACUTE PHASE (< 1 month):
├── Antiviral (valacyclovir/famciclovir) within 72h - reduces PHN risk
├── Cool compresses + calamine lotion (pain + itch)
├── Simple analgesics → codeine → opioids (stepped)
├── Topical cycloplegic + steroid for ocular pain/iritis
└── Consider gabapentin + antiviral for moderate-severe acute pain
ESTABLISHED PHN (> 1 month):
├── Step 1: Gabapentin OR pregabalin (titrate slowly)
├── Step 2: Add TCA (nortriptyline/amitriptyline 25-75 mg nocte)
├── Step 3: Topical lidocaine 5% patch or capsaicin 8% patch
├── Step 4: Opioids (sustained-release oxycodone) for refractory pain
├── Carbamazepine for lancinating pain specifically
└── Nerve block for refractory cases
ITCH-SPECIFIC:
├── Topical: capsaicin cream, lidocaine, calamine
└── Systemic: gabapentin/pregabalin (first-line), TCAs, sedating antihistamines (night)
Recent Evidence Note
A 2024 meta-analysis (PMID 39029866) confirmed that early antiviral intervention significantly reduces PHN incidence, particularly in older patients. The ZEDS trial (completed 2024) is evaluating 1-year valacyclovir suppression post-HZO for reducing ocular complications and PHN - results are emerging in 2025 and may update suppression protocols.
Sources: Kanski's Clinical Ophthalmology 10th ed. | Tintinalli's Emergency Medicine | Bradley & Daroff's Neurology in Clinical Practice | Cummings Otolaryngology | Dermatology 2-Volume Set 5th ed. | Morgan & Mikhail's Clinical Anaesthesiology 7th ed. | AAFP AFP Guidelines
Treatment for tinea
Reading File
Finding Sources
Finding Sources
Searching PubMed
tinea dermatophytosis treatment antifungal
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
terbinafine resistant Trichophyton indotineae treatment 2025 guidelines
Loading Image
Excellent - I now have comprehensive, up-to-date information from multiple authoritative textbooks and current literature. Let me compile the full response.
Treatment of Tinea (Dermatophytosis)
Tinea refers to superficial fungal infections caused by dermatophytes (Trichophyton, Microsporum, Epidermophyton spp.) that invade keratinized tissue. Treatment depends heavily on the site of infection, extent of disease, and species involved.
Pathogens & Key Principle
| Organism | Common species |
|---|---|
| Trichophyton | T. rubrum, T. mentagrophytes, T. tonsurans, T. indotineae (emerging) |
| Microsporum | M. canis, M. gypseum |
| Epidermophyton | E. floccosum |
Core rule: Topical antifungals work for most uncomplicated skin infections (tinea corporis, cruris, pedis, versicolor). Systemic therapy is mandatory for tinea capitis, onychomycosis, and tinea manuum. - Harrison's 22E; Dermatology 5e
Mechanisms of Action
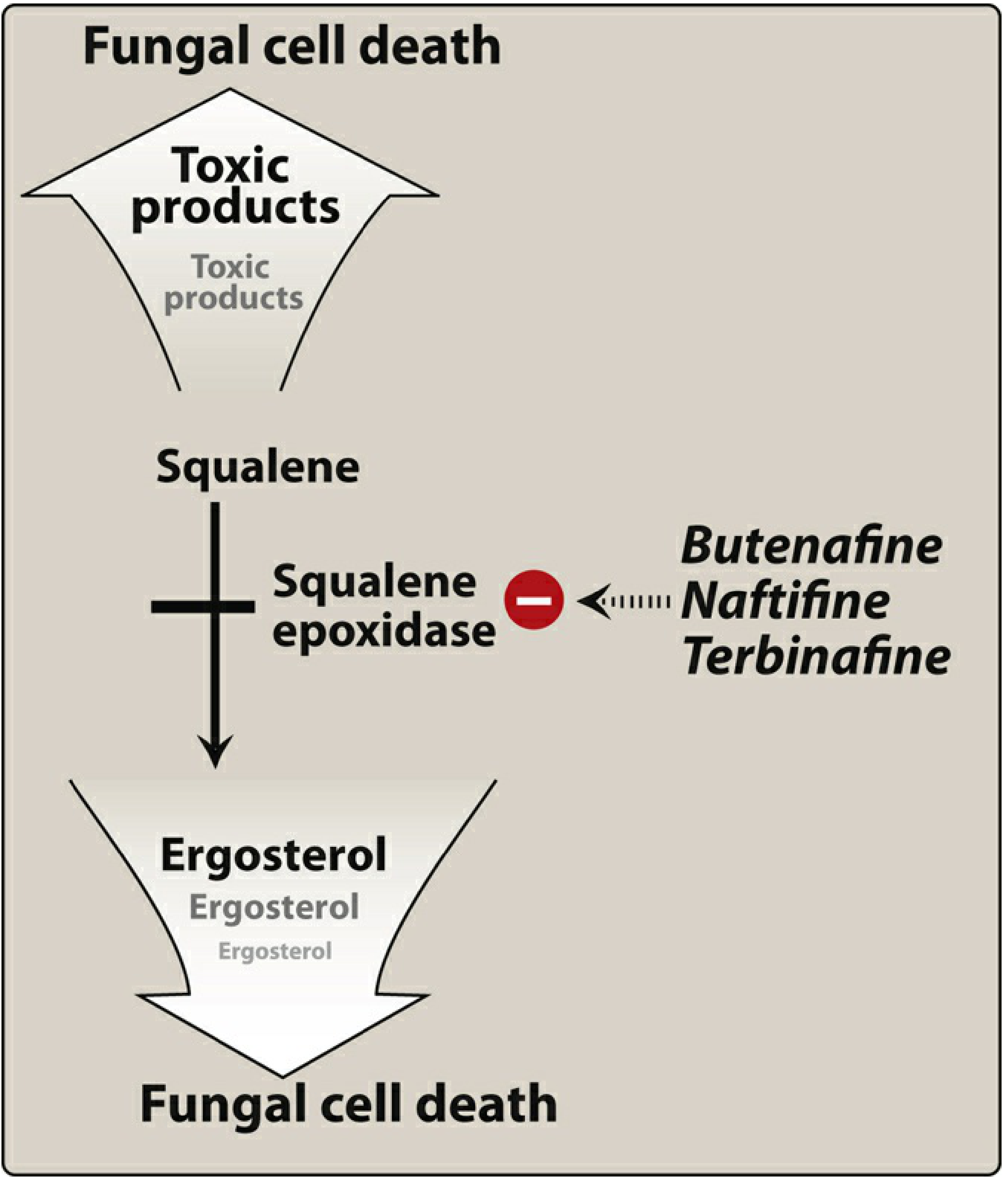
Squalene epoxidase inhibitors (terbinafine, naftifine, butenafine): Block ergosterol synthesis by inhibiting squalene epoxidase - squalene accumulates to toxic levels, disrupting the fungal cell membrane.
Azoles (imidazoles/triazoles): Inhibit lanosterol 14-α-demethylase (CYP51), blocking ergosterol synthesis at a later step - disrupts fungal cell membrane integrity.
Griseofulvin: Disrupts the mitotic spindle - fungistatic. Requires prolonged therapy.
Ciclopirox: Disrupts transport of essential ions - inhibits DNA, RNA, and protein synthesis.
Treatment by Type
1. Tinea Corporis & Tinea Cruris (ringworm, jock itch)
First-line: Topical antifungals (applied BD for 2-4 weeks, continued 1-2 weeks beyond clinical resolution)
| Drug class | Examples |
|---|---|
| Allylamines | Terbinafine 1% cream/gel (1 week), Naftifine cream/gel (2-4 weeks) |
| Imidazoles | Clotrimazole, Miconazole, Econazole, Oxiconazole |
| Thiocarbamate | Tolnaftate cream/solution |
| Pyridine | Ciclopirox cream/gel |
Oral therapy if: extensive disease, hairy sites, immunocompromised, or failure of topicals:
- Terbinafine 250 mg/day x 2-4 weeks
- Itraconazole 200 mg/day x 1-2 weeks
- Fluconazole 150-300 mg/week x 2-4 weeks
- Griseofulvin 500-1000 mg/day (microsize) x 4 weeks
Cure rates with topical agents applied for 2-4 weeks: 70-100%. - Jawetz Microbiology 28E
2. Tinea Pedis (athlete's foot)
Topical antifungals are first-line (same agents as above, but often need longer courses as tinea pedis frequently relapses). Oral agents are needed for recalcitrant or moccasin-type tinea pedis:
| Oral drug | Regimen |
|---|---|
| Terbinafine | 250 mg/day x 2 weeks |
| Itraconazole | 200 mg/day x 2-4 weeks |
| Fluconazole | 150-450 mg/week x 4-6 weeks |
| Griseofulvin | 750-1000 mg/day x 4 weeks |
3. Tinea Capitis (scalp ringworm)
Systemic therapy is mandatory - topical antifungals do not penetrate the hair shaft adequately.
| Drug | Dose/Duration | Notes |
|---|---|---|
| Griseofulvin | 10-25 mg/kg/day x 6-12 weeks (microsize); enhanced by fatty meals | Traditional first-line; fungistatic; long course required |
| Terbinafine | 250 mg/day x 4-6 weeks adults; weight-based in children (granule formulation) | Preferred for Trichophyton; FDA-approved for tinea capitis (granules) |
| Itraconazole | 100 mg/day x 4-6 weeks | Effective alternative |
| Fluconazole | 6 mg/kg/day x 3-6 weeks | Off-label |
Adjunctive: Selenium sulfide or ketoconazole shampoo twice weekly (to reduce shedding and spread - not curative alone)
If markedly inflammatory (kerion): Add systemic corticosteroids (short course) to prevent scarring and hair loss. - Harrison's 22E; Dermatology 5e
4. Tinea Unguium / Onychomycosis (nail infection)
The most difficult tinea to treat. Oral therapy is almost always required for toenails. Topical-only therapy has low cure rates.
Oral regimens (toenails):
| Drug | Regimen | Combined cure rate |
|---|---|---|
| Terbinafine | 250 mg/day x 12 weeks | ~25-35% (toenails) |
| Itraconazole (continuous) | 200 mg/day x 12 weeks | ~20-30% |
| Itraconazole (pulse) | 200 mg BD x 1 week/month x 3 cycles | Similar efficacy |
| Fluconazole | 150-300 mg/week x 6-12 months | Off-label |
| Griseofulvin | 1000 mg/day x 12-18 months | Now largely replaced; long course |
Terbinafine is preferred over itraconazole for Trichophyton (most common pathogen) and requires a shorter course. - Lippincott Pharmacology; Dermatology 5e
Topical options (for mild-moderate disease, or as adjuncts; combined mycologic + clinical cure rates are low 6-20%):
| Drug | Use | Duration |
|---|---|---|
| Efinaconazole 10% solution | Toenail onychomycosis | 48 weeks daily |
| Ciclopirox 8% lacquer | Onychomycosis | 48 weeks daily |
| Tavaborole 5% solution | Toenail onychomycosis | 48 weeks daily |
Preventive measures for onychomycosis: breathable footwear, antifungal powders, frequent nail clipping, discarding old shoes. - Dermatology 2-Volume Set 5e
5. Tinea Manuum (hand ringworm)
Generally requires oral therapy (same agents as corporis/pedis). Adjunctive use of topicals with keratolytics (glycolic acid, lactic acid, urea) helps reduce hyperkeratosis. - Dermatology 5e
6. Tinea Versicolor (Pityriasis versicolor)
Caused by Malassezia furfur (a non-dermatophyte) - treatment differs slightly:
First-line topical:
- Selenium sulfide lotion/shampoo (2.5%) - apply daily x 1-2 weeks, wash off after 10 min
- Ketoconazole 2% shampoo/cream
- Topical terbinafine 1% (also active vs Malassezia)
- Zinc pyrithione shampoo
- Salicylic acid / sulfur-containing preparations
Oral (for widespread disease, or to prevent recurrence):
- Itraconazole 200 mg/day x 5-7 days
- Fluconazole 300 mg single dose or 300 mg/week x 2-4 weeks
- Oral ketoconazole (rarely used now due to hepatotoxicity risk)
Note: Hypopigmentation may persist for months after successful treatment. - Harrison's 22E
Oral Antifungal Comparison
| Drug | Class | MOA | Key use | Key adverse effects | Cautions |
|---|---|---|---|---|---|
| Terbinafine | Allylamine | Squalene epoxidase inhibitor (fungicidal) | Onychomycosis, tinea capitis | GI upset, taste/visual disturbance, hepatotoxicity (rare) | Avoid in hepatic/renal impairment; CYP2D6 inhibitor |
| Itraconazole | Triazole | CYP51 inhibitor | Onychomycosis, tinea capitis | Hepatotoxicity, negative inotropy | Avoid in CHF; multiple CYP450 drug interactions |
| Fluconazole | Triazole | CYP51 inhibitor | Off-label for tinea | GI, hepatotoxicity | Drug interactions (CYP2C9) |
| Griseofulvin | Benzofuran | Mitotic spindle disruption (fungistatic) | Tinea capitis | GI distress, headache, urticaria, photosensitivity | CYP450 inducer; contraindicated in pregnancy and porphyria; long duration |
| Ketoconazole (oral) | Imidazole | CYP51 inhibitor | No longer first-line | Severe hepatotoxicity, adrenal suppression | FDA black box warning; not first-line for any fungal infection |
Combination Topical Steroid + Antifungal
While these formulations reduce inflammation acutely, high-potency corticosteroid-antifungal combinations are not recommended for routine use. High-potency steroids impair immune defenses, can cause striae, and lead to unacceptable treatment failure rates. Reserve antifungal stewardship for straightforward regimens. - Dermatology 5e
⚠️ Emerging Resistance Alert (2025-2026)
Terbinafine-resistant T. indotineae (formerly T. mentagrophytes ITS genotype VIII) has spread globally from an epidemic in India. It frequently causes widespread, intensely pruritic tinea corporis/cruris/faciei with treatment failure on terbinafine (due to SQLE gene mutations).
- Treatment for suspected T. indotineae: Itraconazole 200 mg/day x 8 weeks (first-line per current expert consensus)
- Refractory to itraconazole: Posaconazole or voriconazole (severe cases); combination anidulafungin + itraconazole reported (2026 CDC case report)
- Confirmatory culture and antifungal susceptibility testing is important
- Avoid combination topical corticosteroid-antifungal products (contribute to resistance)
Sources: [Dermatology 5e SQLE resistance section]; CDC Emerg Infect Dis 2026; [PMID 40704771 - Systematic Review 2025]
Summary Quick Reference
TINEA - TREATMENT CHOICE BY SITE
Tinea corporis/cruris → Topical antifungal x 2-4 weeks (terbinafine 1%, clotrimazole, etc.)
Tinea pedis → Topical (longer course); oral for moccasin type / recalcitrant
Tinea capitis → ORAL MANDATORY (griseofulvin or terbinafine) + antifungal shampoo
Tinea unguium → ORAL PREFERRED (terbinafine 12w or itraconazole 12w/pulse x3)
Topical lacquers only for mild/superficial disease
Tinea manuum → Usually oral; add keratolytics
Tinea versicolor → Topical selenium sulfide / ketoconazole shampoo first-line
Oral itraconazole/fluconazole for widespread disease
Resistant (T. indotineae) → Itraconazole 200 mg/day x 8 weeks; culture/susceptibility test
Sources: Harrison's Principles of Internal Medicine 22E | Dermatology 2-Volume Set 5e | Lippincott Illustrated Reviews: Pharmacology | Jawetz Melnick & Adelberg's Medical Microbiology 28E | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.