Organic mental disorders. Dementia, types, characteristics. Mental disorders in vascular diseases of the brain. Clinic. Treatment.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"vascular dementia"[MeSH Terms] AND "treatment"[MeSH Terms]
I now have a comprehensive set of information from multiple textbooks. Let me compose the full, well-structured answer.
Organic Mental Disorders: Dementia - Types, Characteristics, and Vascular Brain Disease
1. Organic Mental Disorders - Overview
"Organic mental disorders" is the older ICD-10 terminology for conditions where mental and behavioral disturbances arise from demonstrable brain disease, brain damage, or dysfunction. The term reflects the contrast with "functional" (idiopathic) psychiatric disorders. DSM-5 replaced "dementia" and related organic syndromes with the umbrella term Major (and Mild) Neurocognitive Disorder (NCD), specifying the underlying etiology (e.g., "major NCD due to Alzheimer's disease").
The spectrum includes:
- Dementia (Major Neurocognitive Disorder) - the primary focus below
- Delirium (acute confusional state)
- Amnestic syndromes (isolated memory loss)
- Organic personality/mood/psychotic disorders (due to brain lesions)
2. Dementia - Definition and Core Criteria
Dementia is defined as a decline in memory or other cognitive abilities from a previously higher level of function, leading to impaired activities of daily living. The decline is typically gradual and progressive over months to years, though acute-onset forms occur.
DSM-5 criteria for Major NCD (Dementia):
- A. Evidence of significant cognitive decline from a previous level in one or more domains (complex attention, executive function, learning/memory, language, perceptual-motor, social cognition)
- B. Cognitive deficits interfere with independence in everyday activities
- C. Not exclusively in the context of delirium
- D. Not better explained by another mental disorder (depression, schizophrenia)
Mild Cognitive Impairment (MCI) is a prodromal state - decline beyond statistical norms for age without significant functional impairment. Some MCI cases progress to dementia; others do not.
Cortical vs. Subcortical Dementia (a traditional but still useful distinction):
- Cortical dementias (e.g., Alzheimer's): prominent disturbances in language, praxis, visuospatial functions, and memory
- Subcortical dementias (e.g., Huntington's, progressive supranuclear palsy, vascular): psychomotor slowing, executive dysfunction, attentional deficits, with relative sparing of language and praxis
3. Types of Dementia and Their Characteristics
3.1 Alzheimer's Disease (AD) - Most Common (~50-68% of cases)
Epidemiology: Prevalence 11% in those ≥65 years; 68% of memory disorder clinic cases.
Neuropathology: Hallmark amyloid plaques and neurofibrillary tangles (hyperphosphorylated tau), beginning in the hippocampal and entorhinal regions. Definitive diagnosis requires postmortem examination; clinical diagnosis uses established criteria (McKhann 2011; DSM-5 "probable AD").
Clinical features:
- Insidious onset, gradual progression
- Early: prominent anterograde memory failure - rapid forgetting of new information, intrusion errors, lack of primacy effect on word lists
- Recognition memory severely impaired (unlike VaD where recognition is relatively preserved)
- Paraphasias, naming problems, semantic difficulties
- Visuospatial impairment, executive dysfunction
- Anosognosia (impaired insight into deficits) - common
- Genetic risk factors: APOE-e4; rare autosomal dominant mutations (APP, PSEN1, PSEN2) account for <1%
Neuroimaging: FDG-PET shows bilateral temporoparietal hypometabolism, with posterior cingulate gyrus and precuneus involvement even early; frontal cortex affected as disease advances.
(Bradley and Daroff's Neurology in Clinical Practice)
3.2 Vascular Dementia (VaD) - Second Most Common (~8-12%)
See Section 4 for full clinical detail on this type as it is the focus of the "mental disorders in vascular disease" portion.
3.3 Dementia with Lewy Bodies (DLB)
Neuropathology: Diffuse cortical neurons with Lewy body inclusions (aggregated alpha-synuclein); absence or inconspicuous neurofibrillary tangles/plaques. Second most frequent pathologic dementia diagnosis after AD.
Core diagnostic features (McKeith criteria - 2 of 3 required):
- Parkinsonian syndrome (usually symmetric)
- Fluctuations in behavior and cognition (episodic delirium, especially nocturnal)
- Recurrent visual hallucinations (highly specific; unlike AD where psychosis is rare until late)
Additional features:
- REM sleep behavior disorder
- Severe neuroleptic sensitivity (extreme and sometimes fatal - contraindicates typical antipsychotics)
- Orthostatic hypotension (autonomic involvement)
- Supranuclear gaze palsy (in some cases)
Cognitive profile: Progressive dementia with executive and attentional deficits; parkinsonian motor features may precede, coincide with, or follow cognitive decline. Memory less severely affected early compared to AD. The "vacuous, anxious state with intermittent psychotic or delirious behavior" imposes high caregiver burden.
Treatment: Cholinesterase inhibitors (donepezil, rivastigmine) improve both cognition and psychiatric symptoms including psychosis. L-dopa has limited, inconsistent benefit and may worsen hallucinations.
(Adams and Victor's Principles of Neurology, 12th Edition)
3.4 Frontotemporal Dementia (FTD)
Epidemiology: Second most common dementia in those under age 65; frequently misdiagnosed as AD.
Behavioral Variant (bvFTD) - the most common:
- Early, prominent personality and behavioral changes: impulsivity, poor judgment, stereotypic behaviors, loss of social behaviors, sexual disinhibition
- Euphoria and disinhibition highly characteristic and predictive of FTD versus other dementias
- Apathy is common but nonspecific
- Impaired metacognition - more severe than in AD; patient is indifferent to their behavior
- Neuropsychological profile: impaired executive functions (mental flexibility, planning, word generation), phonemic fluency worse than semantic fluency
- Memory and visuospatial functioning relatively preserved until late stages - an important differentiator from AD
Language Variants (Primary Progressive Aphasias):
- Semantic variant: impaired single-word comprehension, object/person knowledge, dyslexia; spared repetition and motor speech
- Nonfluent/Agrammatic variant: impaired motor speech, grammatical errors, comprehension of complex sentences; single-word comprehension intact
- Logopenic/Phonologic variant: deficits in word retrieval and sentence repetition; single-word comprehension and motor speech intact
(Bradley and Daroff's Neurology in Clinical Practice)
3.5 Mixed Dementia
More common than pure AD or pure VaD. Typically refers to coexistence of AD and cerebrovascular pathology. Key facts:
- 30% of VaD patients have concurrent AD neuropathology
- 21-80% of dementia autopsy cases have mixed AD + vascular pathology
- Persons with multiple pathologies are 3 times more likely to develop dementia than those with only one identifiable diagnosis
- Mixed dementia cases are more globally impaired than similarly staged pure AD patients
(Bradley and Daroff's Neurology in Clinical Practice)
3.6 Other Dementia Types
| Type | Key Feature |
|---|---|
| Parkinson Disease Dementia | Dementia developing >1 year after motor PD onset; dopaminergic + cholinergic deficit; rivastigmine FDA-approved |
| Normal Pressure Hydrocephalus | Classic triad: gait disturbance + urinary incontinence + dementia (Hakim's triad); potentially reversible with VP shunt |
| Huntington's Disease | Subcortical dementia + chorea + psychiatric symptoms; autosomal dominant (CAG repeat expansion in HTT gene) |
| Prion Disease (CJD) | Rapidly progressive dementia + myoclonus, ataxia, characteristic EEG (periodic sharp wave complexes) |
| Secondary/Reversible Dementias | Hypothyroidism, B12/folate deficiency, neurosyphilis, HIV, normal pressure hydrocephalus, chronic subdural hematoma - all targets for evaluation |
(Neuroanatomy through Clinical Cases, 3rd Ed.)
4. Mental Disorders in Vascular Diseases of the Brain
4.1 Terminology and Scope
Vascular Contributions to Cognitive Impairment and Dementia (VCID) is the current preferred framework (Harrison's, 2025), encompassing:
- Symptomatic strokes (ischemic or hemorrhagic)
- Silent brain infarcts (found in up to 35% of individuals with vascular disease - double the VaD risk)
- Small-vessel disease (arteriolosclerosis, cerebral amyloid angiopathy)
- White matter hyperintensities / Binswanger's disease
VaD is the second most frequent dementia overall, but is especially prevalent in populations with under-treated vascular risk factors, and historically more common than AD in some Asian countries.
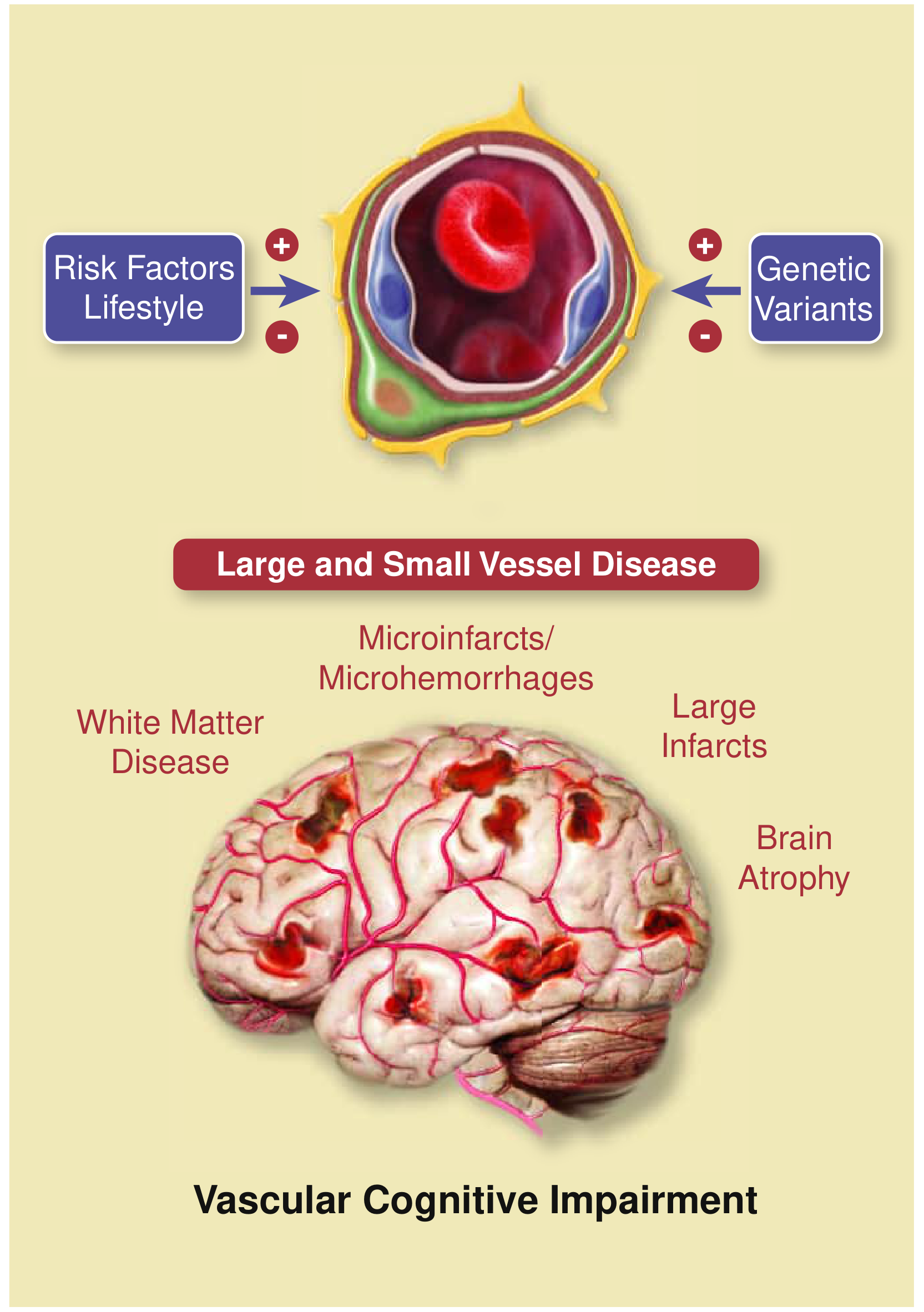
Fig. Vascular Dementia - pathogenesis and structural brain lesions (from Iadecola et al., JACC 2019)
4.2 Subtypes of Cerebrovascular Disease Causing Cognitive Impairment
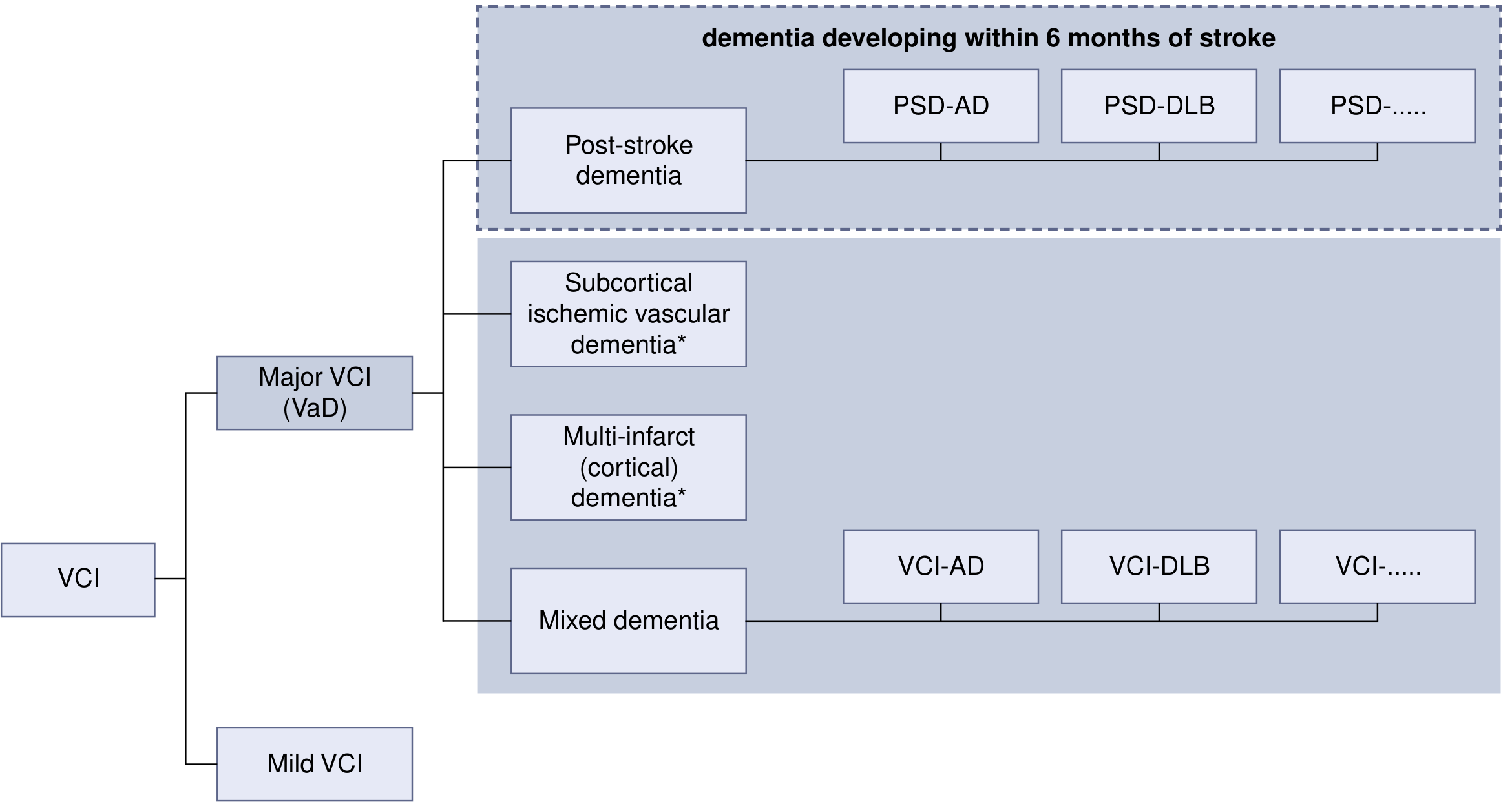
Fig. VICCCS Classification of Vascular Cognitive Impairment
a) Multi-Infarct (Cortical) Dementia
- Results from multiple large cortical infarcts
- Stepwise cognitive deterioration coinciding with each stroke
- Focal neurological deficits corresponding to infarct locations
b) Subcortical Ischemic Vascular Dementia (SIVD) / Small Vessel Disease
- Most frequently observed vascular pathology causing cognitive decline
- Lacunar infarcts in thalamus, basal ganglia, brainstem; periventricular white matter changes
- Prominent executive dysfunction, psychomotor slowing, frontal-subcortical circuit disruption
c) Strategic Infarct Dementia
- Single infarct in a "strategic" location (thalamus, medial temporal cortex, anterior corpus callosum, dominant angular gyrus) sufficient to cause dementia
d) Binswanger's Disease (Subcortical Arteriosclerotic Encephalopathy)
- Severe diffuse white matter injury from small-vessel ischemic disease
- Gradual cognitive deterioration + prominent white matter changes on MRI (periventricular confluent T2/FLAIR hyperintensities)
- Associated with hypoperfusion and hypometabolism
e) CADASIL
- Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy
- Hereditary cause; NOTCH3 gene mutation
- Early-onset (40s-50s), recurrent strokes, migraine with aura, psychiatric symptoms, dementia
(Harrison's Principles of Internal Medicine, 22nd Ed.)
4.3 Clinical Presentation of Vascular Dementia
Cognitive profile (the "subcortical profile"):
- Executive dysfunction is the hallmark - difficulties with complex organization, problem-solving, managing finances
- Psychomotor slowing, impaired complex attention
- Better free recall than AD but impaired retrieval (recognition relatively preserved)
- Phonemic fluency worse than semantic fluency (frontal-subcortical > temporal involvement)
- Verbal memory relatively better than in AD
Onset and progression:
- Can be abrupt with stepwise deterioration following CVAs
- Fluctuating or static course (unlike relentlessly progressive AD)
- Gradual progression with diffuse small-vessel disease is also common
Neuropsychiatric symptoms:
- Depression: 29-39% prevalence; most common neuropsychiatric complication; bidirectional - depression is also an independent risk factor for stroke
- Apathy: very common, especially with frontal lacunae; often mistaken for depression
- Pseudobulbar affect (emotional lability): uncontrolled laughing/crying disproportionate to mood
- Personality change: disinhibition, irritability, passivity
- Psychosis: less common; mania rare; no clear relation to lesion location
Vascular Depression (a distinct entity):
The "vascular depression hypothesis" posits that cerebrovascular disease causes late-onset depressive syndromes characterized by:
- Cognitive deficits + psychomotor retardation
- Lack of insight
- Disability disproportionate to depression severity
- Suboptimal response to antidepressants
- Neuroimaging: subcortical/deep white matter ischemic changes, lacunar infarcts
Key vascular risk factors:
- Hypertension (most common modifiable risk factor)
- Diabetes mellitus
- Dyslipidemia / hypertriglyceridemia
- Atrial fibrillation and cardiac disease (source of emboli)
- Smoking (>1 pack/day in 21% of cases)
- Limited education (reduced cognitive reserve)
- Hypotension (paradoxically the most common direct risk factor for VaD in some series)
(Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Harrison's, 22nd Ed.)
4.4 Diagnosis
Clinical evaluation:
- Identify vascular risk factors (hypertension, diabetes, dyslipidemia, atrial fibrillation, coronary/peripheral arterial disease, tobacco use)
- History of prior stroke or TIA
- Family history of early stroke or vascular disease
- Stepwise progression and executive-predominant cognitive deficits are suggestive
Neuroimaging - the mainstay:
- MRI (preferred): FLAIR + diffusion-weighted + T2*-weighted sequences
- Findings: large and small chronic infarcts, acute microinfarcts, microbleeds, white matter hyperintensities, periventricular confluent changes
- CT/MR angiography: useful for characterizing large-vessel infarcts
Neuropsychological testing: Identifies executive dysfunction, processing speed slowing, and distinguishes VaD from AD
Screening for atrial fibrillation: All patients with embolic-appearing infarcts should be screened; prolonged cardiac monitoring if needed
4.5 Treatment
Treatment is organized into three levels:
A. Primary and Secondary Stroke Prevention (Disease-Modifying)
The most important intervention is aggressive vascular risk factor management:
| Target | Goal |
|---|---|
| Blood pressure | <140/90 mmHg; <130/80 mmHg if 10-year CV risk ≥10%; goal <120 mmHg (SPRINT-MIND) reduced MCI incidence by 19% |
| Cholesterol | Statin therapy (for large-vessel/embolic disease) |
| Blood glucose | Diabetes control |
| Antiplatelet therapy | Antiplatelet agents (aspirin, clopidogrel) for ischemic stroke/TIA history |
| Anticoagulation | Atrial fibrillation management |
| Lifestyle | Smoking cessation, physical activity, heart-healthy diet, weight management, sleep hygiene |
Evidence base:
- Systolic Hypertension in Europe Trial: Aggressive BP control reduced dementia incidence from 7.7 to 3.8 cases per 1000 patient-years
- SPRINT-MIND: Targeting SBP <120 mmHg reduced mild cognitive impairment (HR 0.81) and combined MCI/dementia (HR 0.85)
- PROGRESS study (Perindopril in Recurrent Stroke): Cognitive decline occurred in 9.1% on treatment vs. 11.0% on placebo
(Harrison's; Bradley and Daroff's)
B. Symptomatic Cognitive Treatment
No agents are FDA-approved specifically for VaD, but evidence supports:
- Acetylcholinesterase inhibitors (AChEIs): donepezil, rivastigmine, galantamine - improve cognitive function modestly in VCI; reasonable given frequent mixed AD/vascular pathology
- Donepezil (high-dose) and memantine (NMDA antagonist) may be considered for moderate-to-severe cases
- These agents show modest benefits in VaD comparable in magnitude to those in AD
C. Neuropsychiatric Symptom Management
- Post-stroke depression: SSRIs (first-line); poststroke response to antidepressants also improves ADL function, cognitive function, and reduces disability
- Pseudobulbar affect: Dextromethorphan/quinidine (Nuedexta) - FDA approved for this indication; also SSRIs
- Psychosis, mania: Atypical antipsychotics with caution (stroke risk in elderly); evidence base is limited
- Apathy: Difficult to treat; some benefit with stimulants, dopaminergic agents; behavioral interventions
(Bradley and Daroff's Neurology in Clinical Practice; Kaplan & Sadock's Comprehensive Textbook of Psychiatry)
5. Summary Table: Differential Features of Major Dementias
| Feature | AD | VaD | DLB | FTD |
|---|---|---|---|---|
| Onset | Insidious | Acute/stepwise or gradual | Insidious | Insidious |
| Progression | Gradual, continuous | Stepwise or fluctuating | Fluctuating | Gradual |
| Early memory | Severely impaired | Relatively preserved | Variable | Preserved |
| Executive function | Impaired late | Impaired early | Impaired | Severely impaired early |
| Language | Anomia, paraphasia | Relatively spared | Relatively spared | PPA variants |
| Visuospatial | Impaired | Relatively spared | Impaired | Preserved |
| Behavior/personality | Anosognosia, late changes | Apathy, depression | Hallucinations, delusions | Disinhibition, social breakdown |
| Motor | Late | Focal deficits (post-stroke) | Parkinsonism | Late (in motor neuron disease variant) |
| Imaging | Temporoparietal atrophy; PET hypometabolism | Infarcts, WMH | Dopamine deficit on SPECT | Frontotemporal atrophy |
| Key Rx | AChEIs, memantine | Risk factor control, AChEIs | AChEIs (avoid antipsychotics) | Supportive only |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice (Chapters 42, 44)
- Harrison's Principles of Internal Medicine, 22nd Edition (Chapter 444 - Vascular Dementia)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (Chapters on Vascular NCD, Antidementia Drugs)
- Adams and Victor's Principles of Neurology, 12th Edition (Lewy Body Disease)
- Neuroanatomy through Clinical Cases, 3rd Edition (Chapter 19)
This is a shared conversation. Sign in to Orris to start your own chat.