Surgical techniques for hypospadias
Reading File
Finding Sources
Searching PubMed
"hypospadias"[MeSH Terms] AND "surgical procedures"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"hypospadias"[MeSH Terms] AND repair
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have excellent, comprehensive content from Campbell-Walsh Urology with detailed surgical technique descriptions and images. I have enough to write a thorough answer covering all major techniques.
Surgical Techniques for Hypospadias
Sources: Campbell-Walsh-Wein Urology (11e), Bailey & Love's Short Practice of Surgery (28e), Smith & Tanagho's General Urology (19e)
Classification - The Basis for Surgical Planning
Before choosing a technique, the meatal position must be classified, as this directly governs the approach:
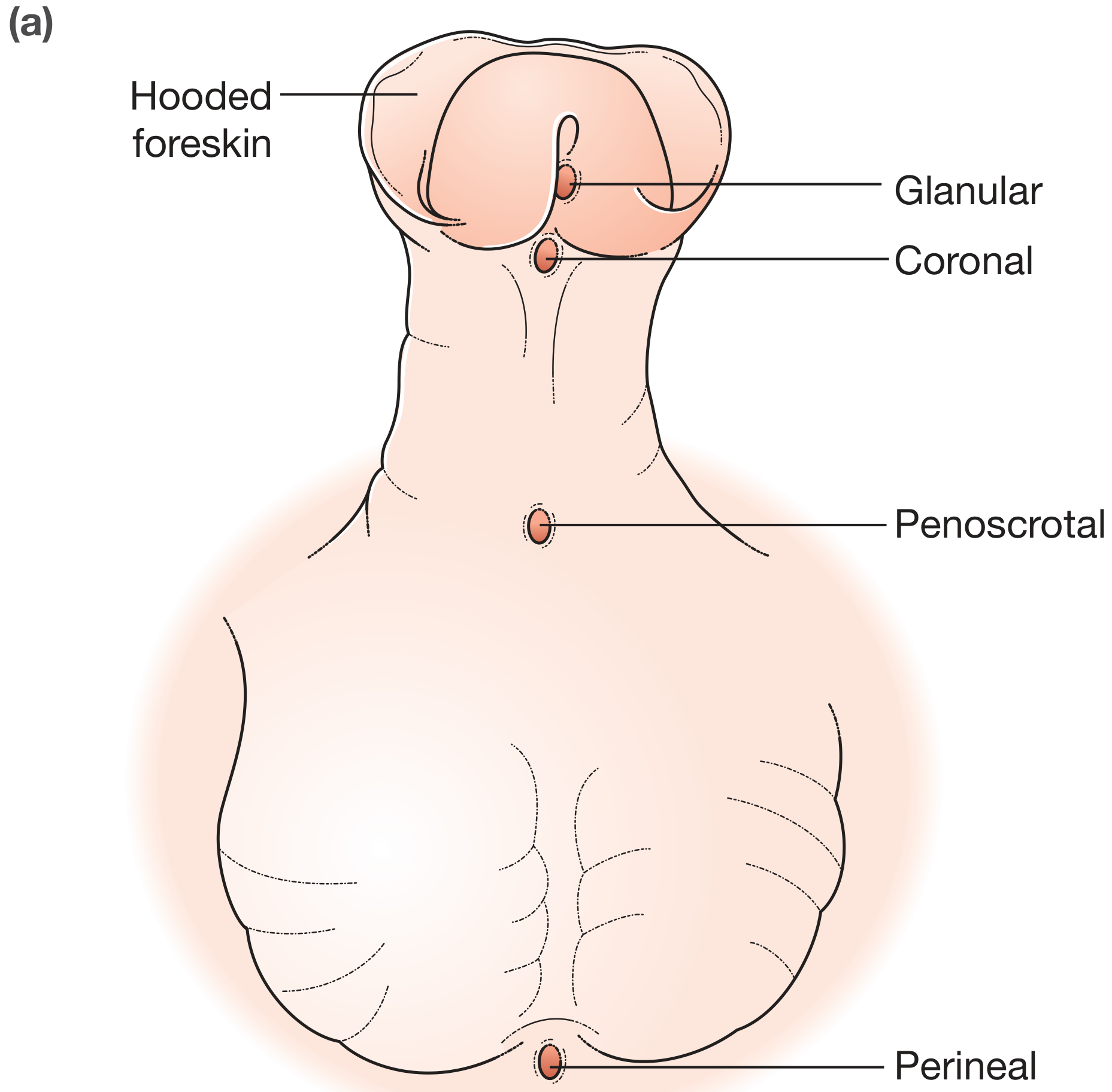
Fig. 45.2a: Classification of hypospadias by meatal position - Bailey & Love's Surgery 28e
| Type | Meatal Position | Usual Surgical Approach |
|---|---|---|
| Glanular | On glans, proximal to normal meatus | Urethromeatoplasty / MAGP |
| Coronal | Coronal sulcus | MAGP, GAP, or TIP |
| Penile (distal-midshaft) | Penile shaft | TIP (Snodgrass) - most common |
| Penoscrotal | Penoscrotal junction | OIF or Two-stage repair |
| Perineal | Between scrotal halves (bifid scrotum) | Two-stage + consider DSD workup |
Key preoperative principle: Circumcision must be avoided - preputial skin is potentially needed for repair or revision.
Optimal surgical age is before 18 months. More than 200 techniques have been described, but the vast majority are variants of a small set of established approaches.
The Three Fundamental Objectives of Any Repair
- Correct penile curvature (chordee) - via degloving, dorsal plication, or corporal grafting
- Urethroplasty - advance or reconstruct the urethra to a glanular, slit-like meatus
- Glansplasty and skin closure - with or without preputioplasty
Urethroplasty Techniques: Three Broad Categories
| Category | Techniques |
|---|---|
| Tubularization of local tissue | Thiersch-Duplay, GAP, TIP (Snodgrass) |
| Flaps from local/preputial skin | MAGP, OIF, TPIF (Duckett tube), Byars flap |
| Free grafts | Buccal mucosal graft (Bracka), inner preputial skin |
Distal Hypospadias Techniques
1. Urethromeatoplasty (Heineke-Mikulicz Principle)
Reserved for the most distal glanular meatus with minimal curvature. A longitudinal vertical incision through the ectopic meatus is closed in a horizontal direction, flattening the posterior urethral plate and advancing the meatus. Particularly useful for a stenotic distal meatus with a blind-ending pit in a closed glans. No tubularization is required.
2. MAGP - Meatal Advancement and Glanuloplasty
- A mucosal collar is marked and holding sutures placed
- The penis is partially degloved
- The meatus is advanced distally (Heineke-Mikulicz rearrangement)
- Glanular spongiosum is exposed after excision of glans edges
- Glans approximation is performed in two layers with a mucosal collar
- Suitable for glanular/coronal meatus with no significant chordee
3. GAP - Glans Approximation Procedure
Designed for proximal glanular/coronal hypospadias with a wide, deep glanular groove and a non-compliant "fish-mouth" meatus (common in the megameatus intact prepuce [MIP] variant). The deep glanular groove allows the glans wings to be approximated in a tension-free manner. A modification of the Thiersch-Duplay repair with deeper glans incision, two-layer running neourethral closure, and dartos flap barrier. The Pyramid procedure is essentially the GAP with an intact prepuce.
4. TIP - Tubularized Incised Plate (Snodgrass) - THE DOMINANT TECHNIQUE
Surveyed pediatric urologists use TIP >90% of the time for distal repairs and ~80% for midshaft repairs.
Steps:
- Circumferential incision around the hypospadiac meatus
- The urethral plate is preserved and a longitudinal midline incision is made along it - this is the key maneuver that relaxes the plate, allows tubularization without tension, and creates a slit-like meatus
- The plate is tubularized (Thiersch-Duplay principle) over a stenting catheter with a two-layer running closure
- Glansplasty is performed with approximation of glans wings
- A dartos flap barrier layer (de-epithelialized Byars flap or tunica vaginalis flap) is interposed between the urethroplasty and skin to reduce fistula risk
- Skin coverage
The midline relaxing incision is what allows TIP to succeed where simple tubularization would produce tension and stricture.
Proximal Hypospadias: One-Stage vs. Two-Stage Repair
Managing Chordee (Penile Curvature) First
For proximal variants, curvature correction must be addressed:
- Dorsal plication - shortens the dorsal tunica albuginea to straighten the penis (simpler, preserves length less)
- Ventral corporotomies with grafting - lengthens the short ventral surface using a dermal, tunica vaginalis, or small intestinal submucosa (SIS) graft
One-Stage Techniques for Proximal Hypospadias
OIF - Onlay Island Flap (Duckett)
- After degloving, if curvature corrects and the urethral plate is adequate, a prepucial island flap is transposed ventrally
- Parallel incisions are made along the urethral plate into the glans
- The prepucial flap is onlaid over the preserved plate (combined width of plate + flap must be ≤12 mm to prevent diverticulum)
- The native meatus is spatulated; the pedicle is carefully draped over the suture line
- Glans wings are brought over the urethroplasty
- Advantages: more pliable tissue gives better urodynamics than rigid TIP tubularization (lower resistance per Poiseuille's law)
TPIF - Transverse Prepucial Island Flap (Duckett Tube)
- Harvested from the inner prepuce, tubularized into a substitution urethroplasty (full-length new urethra)
- The left side of the flap is anchored to the ventral penile shaft, then the flap is closed in the midline with interrupted Lembert sutures
- Pedicle is placed over the suture line; glans wings closed over it
- Indicates for severe curvature corrected after skin dissection when the urethral plate is divided
- Higher complication rate led Duckett to prefer OIF even for severe hypospadias
- Risk: oval (not slit-like) meatus due to bulky tissue in the glans
Two-Stage Techniques (Now Favored for Most Proximal Repairs)
The current trend strongly favors staged repair for proximal hypospadias, especially when corporal lengthening is needed, because combining corporotomy grafting with urethroplasty in one stage significantly raises failure risk.
Stage 1: Correct curvature (dorsal plication ± ventral corporal grafting), divide the urethral plate, provide supple ventral shaft tissue
Stage 2 (≥6 months later): Tubularize the neourethra and perform glansplasty
Stage 2 (≥6 months later): Tubularize the neourethra and perform glansplasty
A. Bracka Two-Stage / STAG (Staged Tubularized Autograft) Repair
- Stage 1: Curvature correction + urethral plate division; a midline incision extended into the glans creates a receiving bed; a free graft (inner preputial skin or buccal mucosa) is placed and quilted to prevent hematoma and facilitate graft take
- Stage 2: U-shaped (Thiersch-Duplay-type) incision; the neo-urethra is tubularized, glansplasty performed, multilayer closure
Buccal mucosa (harvested from the inner cheek) is the preferred graft material for revision cases or when preputial skin is unavailable - it is moist, hairless, resilient, and has a good submucosa for vascularization.
B. Byars Flap Two-Stage Repair
- Stage 1: Redundant dorsal preputial skin is transposed ventrally with its vascular pedicle; skin halves can be joined at the midline ventral surface or left as bilateral halves to be joined at the second stage
- Stage 2: The transposed skin is tubularized to form the neourethra
This pedicled approach preserves blood supply and avoids free graft take concerns.
Belman De-epithelialized Flap (Barrier Layer Coverage)
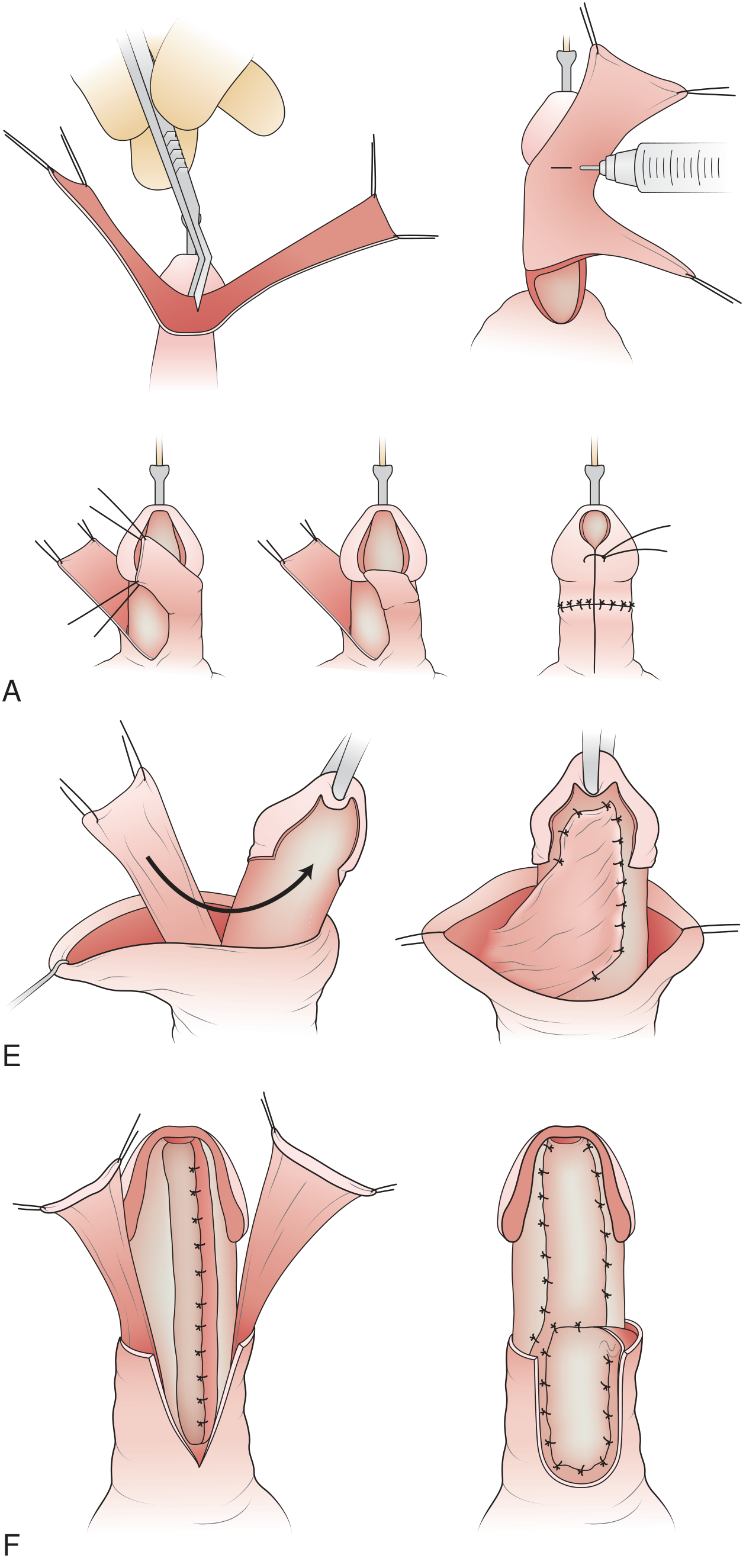
Fig. 45.12 from Campbell-Walsh: De-epithelialized Byars flap technique providing vascularized dartos barrier over urethroplasty, with tunica vaginalis flap as an alternative
This is not a standalone repair but a critical adjunct used with most modern techniques. The dorsal prepucial skin is incised, epithelium removed, and the well-vascularized dartos is rotated ventrally as a barrier layer between the urethroplasty suture line and the overlying skin. This reduces fistula risk by:
- Adding a vascular layer
- Offsetting suture lines
- Providing tissue bulk over the repair
Failed Hypospadias Repair (Redo Surgery)
Complications requiring re-operation include:
- Urethrocutaneous fistula - most common (~10% incidence); occurs at the original meatus site or coronal margin; repair is delayed 6 months; small fistulae may be closed primarily with multilayer closure; larger ones may require flap interposition
- Urethral stricture - risk proportional to neourethra length (Poiseuille's law); short TIP repairs have lower resistance than long proximal repairs
- Urethral diverticulum - from uneven caliber or distal obstruction; the non-distensible glans creates back-pressure
- Persistent/recurrent chordee - residual or differential growth of hypoplastic tissue
- Meatal stenosis
Re-operative rates after planned two-stage proximal repair range from 25-75%, underscoring the difficulty of proximal hypospadias.
For redo cases, buccal mucosal grafting (two-stage Bracka approach) is the most widely used strategy when no local genital skin is available.
Postoperative Management
- Urinary diversion: Urethral stent/feeding tube (not always mandatory for distal repairs; nearly universal for proximal)
- Dressing: Compression dressing for 24-48 hours to reduce edema; some surgeons use silicone mesh or hydrocolloid
- Antibiotics: Prophylactic coverage for the duration of stenting
- Anticholinergics: Used by some centers to reduce bladder spasm
- Activity restriction: 2-4 weeks; no straddle toys
Long-Term Outcomes
- Distal repairs (especially TIP): ~90% success rate
- Proximal repairs: 25-75% eventually require re-operation
- Long-term concerns include: post-void dribbling (20-40%), spraying (40-50%), downward stream deflection (25%), erectile problems (~25%), ejaculatory dysfunction (37%), and infertility (~13% in isolated hypospadias)
- Regular adolescent follow-up is recommended for proximal/severe variants
Summary: Choosing a Technique
| Severity | First-Line Technique | Alternative |
|---|---|---|
| Glanular (MIP variant) | Urethromeatoplasty / GAP | MAGP |
| Distal / coronal | TIP (Snodgrass) | MAGP |
| Midshaft | TIP or OIF | TPIF |
| Proximal (curvature correctable) | OIF | One-stage TPIF |
| Proximal (severe curvature) | Two-stage (Bracka/STAG) | Byars flap two-stage |
| Redo / no local skin | Buccal mucosal graft (two-stage) | - |
Recent PubMed evidence (2023-2026): A systematic review and meta-analysis (PMID 38974407) examined the benefit of tissue sealants on urethroplasty in hypospadias, suggesting adjunctive sealants may reduce fistula rates - though overall evidence quality remains limited. A 2023 review by Snodgrass & Bush (PMID 37385706) emphasizes that adult outcomes data are reshaping how pediatric urologists approach primary repair decisions.
- Campbell-Walsh-Wein Urology 11e, Chapter 45 (Hypospadias), pp. 1181-1199
- Bailey & Love's Short Practice of Surgery 28e, Chapter 85, pp. 1560-1561
This is a shared conversation. Sign in to Orris to start your own chat.