Enumerate the causes of hematuria
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have excellent, comprehensive data. Let me compile the full answer.
Causes of Hematuria
Hematuria is defined as >3-5 RBCs per high-power field on microscopy, or visibly red/brown urine (gross hematuria). Causes are best organized by anatomical origin: renal (intrarenal) vs. extrarenal, and further subdivided by mechanism.
First: Pseudo-hematuria (Red Urine Without RBCs)
Before listing true causes, these mimic hematuria on dipstick but show no RBCs on microscopy:
| Category | Examples |
|---|---|
| Medications | Rifampin, phenazopyridine, nitrofurantoin, doxorubicin, chloroquine, phenytoin |
| Foods | Beets, blackberries, food coloring, rhubarb |
| Metabolites | Hemoglobinuria (hemolysis), myoglobinuria (rhabdomyolysis), bilirubin, porphyrins, urates, melanin |
A. Renal (Intrarenal) Causes
1. Glomerular
These typically produce dysmorphic RBCs, RBC casts, and are often accompanied by proteinuria.
- IgA nephropathy - the most common glomerular cause of hematuria worldwide; classically episodic gross hematuria coinciding with mucosal infections
- Thin basement membrane nephropathy (TBMN) - most important differential for isolated microscopic hematuria in young adults
- Alport syndrome - X-linked hereditary nephritis with hematuria, proteinuria, sensorineural deafness, and ocular anomalies
- Postinfectious / post-streptococcal glomerulonephritis - follows throat or skin infection; low complement, ASO elevated
- Lupus nephritis (SLE) - immune complex deposition; ANA/anti-dsDNA positive
- Goodpasture syndrome - anti-GBM antibodies; pulmonary-renal syndrome
- IgA vasculitis (Henoch-Schonlein purpura) - palpable purpura, arthritis, abdominal pain + hematuria/proteinuria
- ANCA-associated vasculitides (GPA, MPA, EGPA) - pauci-immune crescentic GN
- Hemolytic uremic syndrome (HUS) - microangiopathic hemolytic anemia + thrombocytopenia + AKI
- Membranoproliferative GN - recurrent hematuria especially in children/young adults
- Crescentic (rapidly progressive) GN - any of the above progressing to nephritic emergency
2. Tubulointerstitial
- Nephrolithiasis (urolithiasis) - colicky flank pain radiating to groin; very common cause of gross hematuria; calcium oxalate most frequent
- Pyelonephritis - upper UTI with fever, costovertebral angle tenderness; WBC casts on UA
- Acute interstitial nephritis (AIN) - drug-induced (NSAIDs, penicillins, PPIs) or immune; eosinophiluria
- Acute tubular necrosis (ATN)
- Papillary necrosis - associated with sickle cell disease, analgesic nephropathy, diabetes, obstruction
- Polycystic kidney disease (PKD) - autosomal dominant; bilateral cystic kidneys
- Medullary sponge kidney - dilated collecting tubules; associated with nephrocalcinosis and recurrent stones
3. Neoplastic (Renal)
- Renal cell carcinoma - classic triad: hematuria, flank pain, palpable mass (only ~10% present with all three)
- Transitional cell carcinoma (urothelial carcinoma) of the renal pelvis
- Wilms tumor (nephroblastoma) - most common renal malignancy in children
- Benign renal masses - angiomyolipoma, oncocytoma
4. Vascular
- Renal artery embolism or thrombosis - sudden flank pain, hematuria, hypertension
- Renal vein thrombosis - associated with nephrotic syndrome, dehydration in infants
- Arteriovenous malformation (AVM) / arteriovenous fistula
- Nutcracker syndrome - compression of the left renal vein between the aorta and SMA; causes left-sided hematuria and flank pain
- Malignant hypertension
5. Metabolic
- Hypercalciuria - a common cause of hematuria, especially in children; check urine calcium
- Hyperuricosuria
6. Miscellaneous Renal
- Trauma - renal contusion or laceration
- Recurrent familial (benign) hematuria
- Exercise-induced hematuria - resolves within 72 hours of stopping exercise
B. Extrarenal Causes
1. Ureteral
- Mass: benign polyp or urothelial malignancy
- Ureteral stone / calculus
- Stricture
2. Bladder
- Transitional cell (urothelial) carcinoma of the bladder - most common cause of gross hematuria in adults >50; painless hematuria
- Squamous cell carcinoma - associated with chronic schistosomiasis, chronic catheterization
- Infectious cystitis (UTI) - most common cause of hematuria overall; dysuria, frequency, urgency
- Noninfectious cystitis:
- Hemorrhagic cystitis - from cyclophosphamide or ifosfamide (acrolein metabolite)
- Radiation cystitis - after pelvic radiation
- Bladder trauma or foreign body
3. Prostate / Urethra
- Benign prostatic hyperplasia (BPH) - common in older men; can cause gross hematuria
- Prostate carcinoma
- Prostatitis
- Urethritis - gonorrheal, chlamydial, or non-specific
- Meatal stenosis / posterior urethral valves - in children
- Urethral stricture
- Urethral caruncle - in postmenopausal women
4. Systemic / Other
- Bleeding diatheses - thrombocytopenia, hemophilia, anticoagulant therapy (warfarin, heparin, DOACs)
- Sickle cell disease / hemoglobinopathy - papillary necrosis, sickling in renal medulla
- Endocarditis - embolic or immune complex nephritis
- Mononucleosis (EBV)
- Schistosomiasis - S. haematobium infects bladder wall; classic cause in endemic areas
- Tuberculosis - sterile pyuria + hematuria; "putty kidney" calcifications
5. Spurious / Contamination
- Menstrual blood contamination
- Rectal bleeding (especially in children)
- Sexual intercourse (transient)
Key Distinguishing Points
| Feature | Glomerular Hematuria | Non-glomerular Hematuria |
|---|---|---|
| RBC morphology | Dysmorphic (acanthocytes) | Eumorphic (normal shape) |
| RBC casts | Present | Absent |
| Proteinuria | Often significant | Absent or mild |
| Clots in urine | Never | May be present |
| Hypertension/edema | Common | Absent unless advanced |
Blood clots in urine are never from a glomerular source and always indicate a lower urinary tract or vascular lesion. - Symptom to Diagnosis: An Evidence-Based Guide, 4th ed.
Macroscopic hematuria is typically due to bladder or urethral damage, whereas microscopic hematuria is more commonly from glomerular or tubular damage. - Rosen's Emergency Medicine
Investigation algorithm in a 55-year-old man presenting with painless haematuria.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative data from Campbell Walsh Urology and Symptom to Diagnosis. Let me compile a full, well-structured answer.
Investigation Algorithm: Painless Hematuria in a 55-Year-Old Man
Why This Presentation Demands Urgent Attention
Painless hematuria in a man over 40 is bladder urothelial carcinoma until proven otherwise. In patients presenting to hematuria clinics with gross hematuria:
- 20-25% have bladder cancer
- 1.3-10% have prostate cancer
- 0.6-2% have renal cell carcinoma
- ~21% have stones
- 12-13% have BPH
The overall risk of malignancy in gross hematuria is 20.4%. Even a single episode of gross hematuria must be fully evaluated - do not be reassured by a negative subsequent urinalysis. Anticoagulant therapy does not eliminate the need for full workup. - Campbell Walsh Wein Urology
Step 1 - Confirm True Hematuria
Urine dipstick is sensitive (91-100%) but poorly specific (65%) due to cross-reactivity with hemoglobin and myoglobin. It must always be confirmed with:
- Microscopic urinalysis (UA with microscopy): the gold standard. Confirms hematuria as ≥3 RBCs/hpf. A single positive microscopic UA is sufficient to prompt full evaluation.
- If dipstick is positive but no RBCs on microscopy, consider myoglobinuria (rhabdomyolysis) or hemoglobinuria (hemolysis).
- If urine is red/brown but UA is normal, consider pigmenturia: beets, rifampin, phenazopyridine, porphyrins.
Step 2 - Initial Assessment (History, Exam, Basic Labs)
History - risk stratification for malignancy:
| Risk Factor | Significance |
|---|---|
| Age >40, male sex | High-risk demographic for bladder cancer |
| Smoking (current or former) | Single most important modifiable risk factor for bladder cancer |
| Occupational exposures | Aromatic amines, aniline dyes, rubber, leather, mining; 10-20 year latency |
| Cyclophosphamide/ifosfamide use | Hemorrhagic cystitis |
| Pelvic radiation history | Radiation cystitis |
| Analgesic abuse | Papillary necrosis |
| LUTS (frequency, urgency, nocturia) | BPH, prostatitis, or CIS of bladder |
| Flank pain | Calculus, RCC, obstruction |
| Family history of kidney disease | Hereditary nephritis, PKD |
| Medications | Anticoagulants, NSAIDs, cyclophosphamide |
Physical examination:
- Abdominal mass / renal ballottement (RCC, PKD)
- Digital rectal exam (DRE) - prostate size, nodularity, tenderness
- Bimanual exam if bladder tumor suspected
- Blood pressure (hypertension - glomerular disease, RCC)
- Signs of systemic disease (rash, arthritis, edema)
Basic blood tests:
- Full blood count
- Renal function (creatinine, eGFR, electrolytes)
- Coagulation screen (PT/INR, APTT)
- PSA - discuss with patient; ~10% of men with recurrent gross hematuria have prostate cancer - Campbell Walsh Wein Urology
Step 3 - Urine Studies
| Test | Indication | Notes |
|---|---|---|
| Urine microscopy | All patients | RBC morphology: dysmorphic RBCs / acanthocytes + casts = glomerular origin |
| Urine culture (MSU) | All patients | Exclude UTI before proceeding - treat if positive and repeat UA |
| Urine cytology | Gross hematuria | ~50% sensitivity for high-grade bladder cancer; adjunct to cystoscopy; not recommended for routine microhematuria workup |
| Urine biomarkers (NMP22, BladderChek, UroVysion FISH) | Gross hematuria | Higher sensitivity than cytology for low-grade tumors; used adjunctively |
| Protein:creatinine ratio | If proteinuria present | Points toward glomerular disease |
Key decision point on UA microscopy:
- Dysmorphic RBCs + RBC casts + proteinuria → glomerular hematuria pathway → nephrology referral (± renal biopsy)
- Normal RBC morphology, no casts, no significant proteinuria → non-glomerular / lower urinary tract pathway → urological workup
Step 4 - Imaging
For gross hematuria in a 55-year-old man:
CT Urogram (CTU) - First-Line Imaging
- Multi-phase CT scan: non-contrast phase + nephrographic phase + excretory/delayed phase (opacifies the pelvicalyceal system, ureters, and bladder)
- Sensitivity 92-100% and specificity 94-97% for renal masses, urinary tract stones, and urothelial carcinomas
- Has largely replaced IVP (intravenous pyelogram), plain renal ultrasound alone, and conventional CT for hematuria workup
- Radiation dose is significant - justified in high-risk patients
- If CTU is done first, it may improve the sensitivity of subsequent cystoscopy
Note: Renal/bladder ultrasound alone may suffice for asymptomatic microhematuria in lower-risk patients, but for gross hematuria in a 55-year-old man, CTU is the standard.
Step 5 - Cystoscopy
White-light flexible cystoscopy is the gold standard for diagnosing bladder cancer. It is mandatory in any adult with gross hematuria not explained by infection.
- Direct visualisation of the entire bladder urothelium and urethra
- Random cold-cup biopsies taken to detect carcinoma in situ (CIS), which is flat and not visible to the naked eye
- Hexaminolevulinate (HAL) fluorescence cystoscopy ("blue light" cystoscopy): photosensitiser instilled intravesically; cancer cells fluoresce red under blue light - improves CIS detection
- If bladder tumour found, transurethral resection of bladder tumour (TURBT) is performed for diagnosis and staging
- Bimanual examination under anaesthesia at time of TURBT assesses for muscle invasion
Diagnostic Algorithm Summary
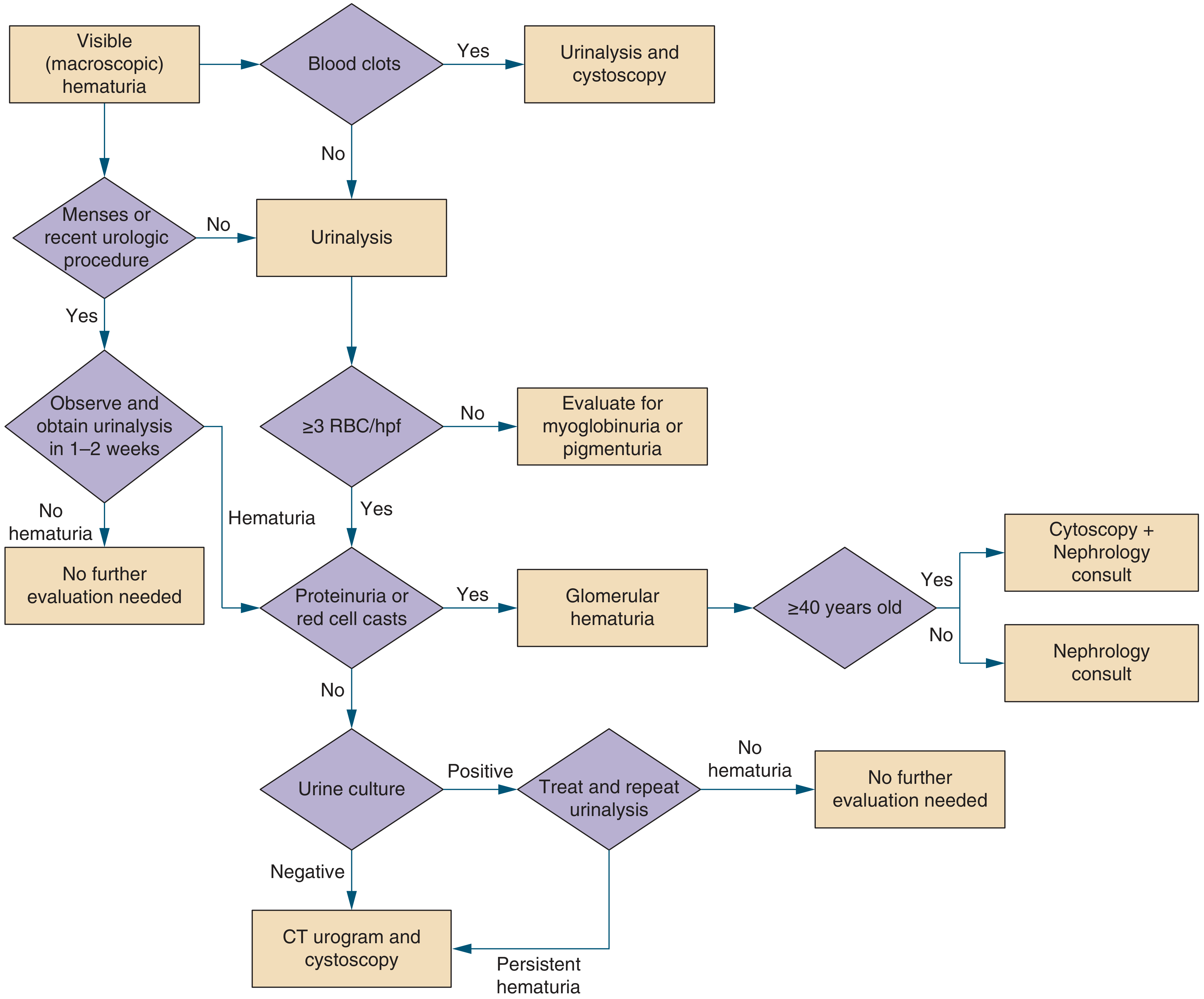
Figure: Diagnostic approach to visible (gross) hematuria - Symptom to Diagnosis, 4th ed.
Adapted for a 55-year-old man with painless hematuria:
Painless gross hematuria
│
▼
Confirm with UA microscopy (≥3 RBCs/hpf)
│
├─── Dipstick+ but no RBCs → Myoglobinuria / Hemoglobinuria
│
▼
Urine culture (MSU)
│
├─── Positive → Treat UTI → Repeat UA → if resolved, stop
│ if persistent → full workup
│
▼
Check UA for proteinuria / RBC casts / dysmorphic RBCs
│
├─── Yes (glomerular features) → Nephrology referral
│ ± Renal biopsy
│
▼ (No glomerular features)
UROLOGY WORKUP (Simultaneous)
┌─────────────────────────┐
│ CT Urogram │ ← Upper tract + bladder imaging
│ Flexible Cystoscopy │ ← Lower tract, gold standard
│ Urine Cytology │ ← Adjunct for urothelial cancer
│ PSA │ ← Prostate cancer
│ DRE │ ← Prostate assessment
└─────────────────────────┘
│
├─── Bladder tumour → TURBT (diagnostic + therapeutic)
├─── Renal mass → Staging CT chest/abdomen/pelvis → Urology/Oncology
├─── Calculus → Urology (stone management)
├─── BPH → Urology management
├─── Prostate cancer → Urology/Oncology staging
└─── No cause found → Repeat evaluation at 3-5 years
Differential Diagnosis Table (55-Year-Old Male, Painless Hematuria)
| Diagnosis | Key Clues | Primary Test |
|---|---|---|
| Bladder cancer (leading) | Age >40, male, smoker, painless | Cystoscopy + CTU |
| Stone disease | Can be painless if not obstructing | Non-contrast CT |
| BPH | LUTS, elderly male | DRE, flow studies |
| Prostate cancer | Painless, abnormal DRE | PSA, DRE, biopsy |
| Renal cell carcinoma | Painless mass, weight loss | CT abdomen |
| Urothelial carcinoma of renal pelvis/ureter | Upper tract filling defect | CTU, ureteroscopy |
| Prostatitis | Pain, fever, tender prostate | DRE, MSU |
Key Principles
- Never attribute gross hematuria to anticoagulation alone - the underlying cause still requires exclusion
- Any single episode of gross hematuria in a man >40 requires full urological workup, even if the next UA is clear
- Urothelial cancer is a must-not-miss diagnosis in gross hematuria not due to infection - Symptom to Diagnosis, 4th ed.
- Glomerular features (dysmorphic RBCs, casts, heavy proteinuria) divert the workup toward nephrology
- If a full workup is negative, the risk of malignancy within 6 years is near zero; repeat evaluation can be deferred 3-5 years - Campbell Walsh Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.