angiosarcoma
Reading File
Finding Sources
Searching PubMed
angiosarcoma
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive material from multiple authoritative textbooks plus histology images. Let me compile the full answer.
Angiosarcoma
Definition
Angiosarcoma is a malignant neoplasm arising from the endothelial lining of blood (or lymphatic) vessels. It is one of the most aggressive soft-tissue sarcomas (STS), accounting for approximately 2% of all STS. Histology ranges from well-differentiated tumors that mimic hemangiomas to profoundly anaplastic, poorly differentiated lesions.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 493
- Sabiston Textbook of Surgery, 14e
Epidemiology
- Peak incidence in the 7th and 8th decades; older adults predominate
- Male:female ratio ~2:1 for cutaneous head-and-neck form
- Most common sites (decreasing order): skin > soft tissue > breast > liver > spleen
- ~20% of patients present with distant metastasis at diagnosis
- ~40% of all angiosarcomas are radiation-associated
Pathogenesis and Risk Factors
Angiosarcoma arises in four distinct clinical settings:
| Setting | Key Feature |
|---|---|
| Sporadic (de novo) | Head/neck skin in elderly men; most common type |
| Chronic lymphedema | Post-mastectomy upper arm - "Stewart-Treves syndrome"; occurs ~11-12 years post-surgery in ~0.45% of patients; 5-year survival 6-14% |
| Post-irradiation | Latency ~23 years (benign condition) or ~12 years (prior malignancy) |
| Chemical/hepatic | Arsenic, Thorotrast (radioactive contrast agent), polyvinyl chloride - all classic hepatic angiosarcoma carcinogens with long latency |
Molecular Biology
- MYC amplification is the molecular hallmark of secondary (post-radiation and post-lymphedema) angiosarcoma - it is absent in primary cutaneous angiosarcoma and in atypical vascular lesions (AVL), making it a key discriminator
- KDR (VEGFR2) activating mutations have been identified in human angiosarcomas
- High Ki-67 proliferation index is characteristic
Pathology
Gross
- Ill-defined, dark-brown/hemorrhagic mass; often multifocal
- In the heart/right ventricle: appears as a large, dark, infiltrating mass (see image A below)
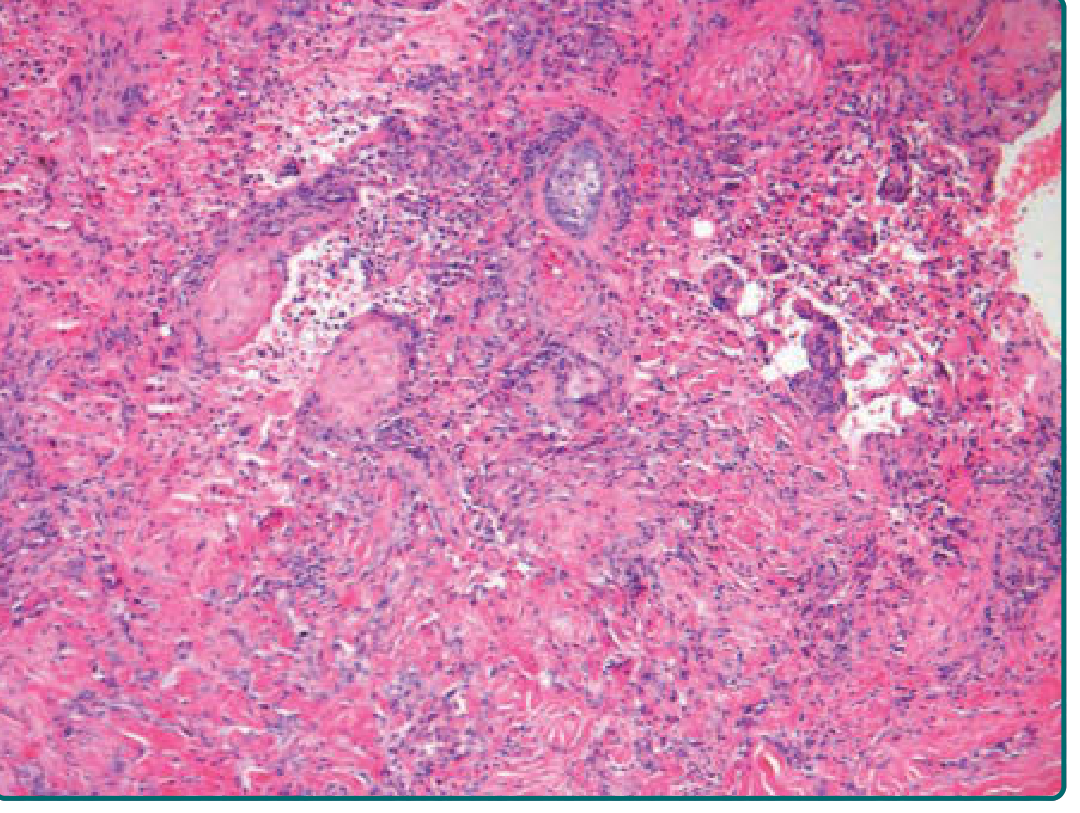
Histology
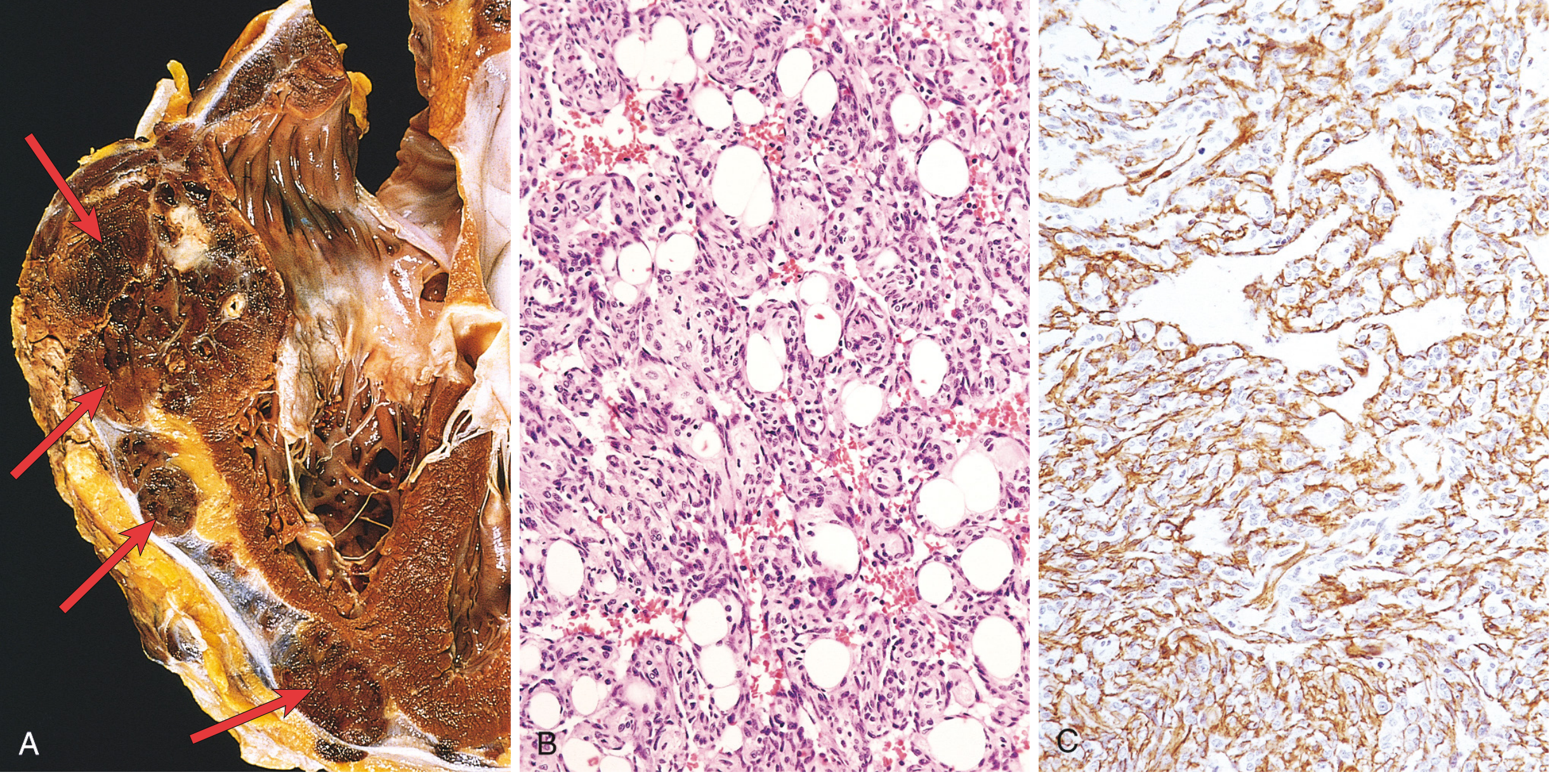
Fig. 11.32 - Robbins, Cotran & Kumar Pathologic Basis of Disease
- Well-differentiated: irregular vascular channels in dermis lined by atypical endothelial cells with enlarged, pleomorphic nuclei
- Poorly differentiated: solid sheets of epithelioid cells, increased cellularity, nuclear atypia, high mitotic activity; subtle infiltration between collagen bundles producing "crack-like" spaces with hyperchromatic nuclei
Fitzpatrick's Dermatology
Immunohistochemistry (IHC)
The following markers confirm endothelial origin:
- CD31 - most consistent and specific
- CD34
- FLI-1 (transcription factor)
- ERG (endothelial transcription factor)
- Podoplanin (D2-40) - positive in most malignant vascular tumors
- Ulex europaeus lectin
- c-MYC nuclear staining - helps distinguish radiation-induced angiosarcoma from AVL
Clinical Presentation
Cutaneous (Head/Neck - most common)
- Poorly defined bluish macule on the scalp/face of elderly men - easily mistaken for a bruise
- Distinguishing features: peripheral erythematous ring, satellite nodules, spontaneous bleeding, intratumoral hemorrhage
- Progressive asymmetric enlargement with indurated bluish nodules/plaques
- Sudden thrombocytopenia may herald metastasis or rapid tumor expansion
- Multicentricity and early metastasis are hallmarks; most patients die within 2 years
- Prognosis worse in men >70
Stewart-Treves Syndrome
- Angiosarcoma in chronic lymphedematous upper arm after mastectomy
- Mean survival 19-31 months; 5-year survival ~6-14%
- Lung metastases are the most frequent cause of death
- Early amputation offers the best prognosis
Spread and Prognosis
- Locally invasive with early hematogenous metastasis
- Lung is the most common metastatic site; breast angiosarcoma may spread to liver
- Overall 5-year survival: 10-30% (Robbins)
- 5-year disease-specific survival for resectable disease: ~53% (Sabiston)
- Stage IV median survival: 8-12 months
Management
Surgery
- Wide resection with negative margins (at least 2 cm of normal tissue) is the mainstay
- Tumors microscopically extend well beyond gross margins
- Radiation-associated breast angiosarcoma: mastectomy including all irradiated skin (vs. simple mastectomy - dramatically reduces local recurrence from 76% to 23% and improves 5-year DSS from 46% to 86%)
- Stewart-Treves: amputation
Radiation Therapy
- Adjuvant radiotherapy for head/neck and scalp angiosarcomas (high locoregional recurrence)
- Cannot use for radiation-induced tumors
Systemic Therapy (Palliative/Metastatic)
| Agent | Notes |
|---|---|
| Paclitaxel | First-line palliative for cutaneous angiosarcoma; ~56% objective response rate |
| Doxorubicin ± ifosfamide | Standard chemotherapy; modest response rate |
| Pazopanib | For taxane-resistant disease; controls progression especially in cutaneous angiosarcoma |
| Sirolimus | Shows promise for scalp/facial angiosarcomas |
| Interferon (IFN) | Shows promise for scalp/facial angiosarcomas |
Key Points to Remember
- Malignant endothelial neoplasm - arises from blood/lymphatic vessel endothelium
- Four clinical settings: sporadic head/neck, Stewart-Treves (lymphedema), post-irradiation, chemical (hepatic)
- MYC amplification = molecular hallmark of secondary (radiation/lymphedema-associated) angiosarcoma
- IHC: CD31 + CD34 + FLI-1 + ERG (confirm endothelial origin); c-MYC distinguishes radiation-induced from AVL
- Paclitaxel is first-line systemic therapy; doxorubicin and pazopanib are alternatives
- Overall poor prognosis: 5-year survival 10-30%; stage IV median survival 8-12 months
- Wide surgical margins critical - tumors extend microscopically well beyond gross disease
Recent Literature: A 2025 systematic review (PMID 40666093) in Frontiers in Oncology reviewed biomarkers in angiosarcoma diagnosis, prognosis, and therapeutics - consistent with the molecular data above. No major updates contradict current textbook guidance.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Sabiston Textbook of Surgery, 14e | Andrews' Diseases of the Skin, 12e | Fitzpatrick's Dermatology, 9e
This is a shared conversation. Sign in to Orris to start your own chat.