Multiple sclerosis
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"multiple sclerosis" AND "clinical features" AND subtypes
Searching Images
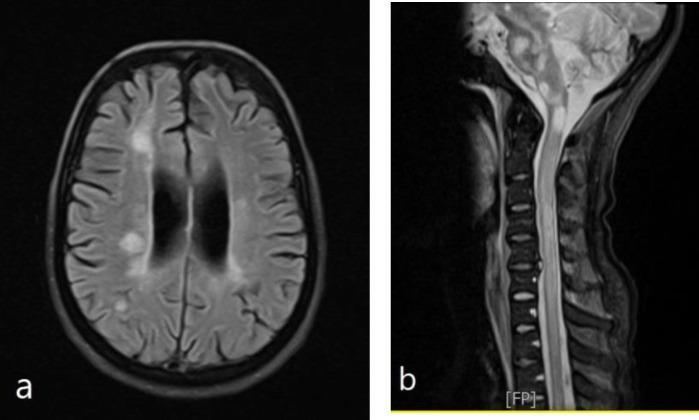
multiple sclerosis MRI lesions demyelination
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from both Bradley/Daroff Neurology and Harrison's to compile a thorough response on MS clinical features and subtypes. Let me compose the answer.
Multiple Sclerosis: Clinical Features & Subtypes
Overview
MS is a chronic immune-mediated demyelinating and neurodegenerative disorder of the CNS. The hallmark of its clinical presentation is variability — in mode of onset, relapse frequency and severity, disability accumulation, and course over time. The clinical features reflect the distribution of demyelinating plaques across the CNS, most characteristically in the optic nerves, brainstem, spinal cord, and periventricular white matter.
Disease Subtypes
The 2013 revised phenotypic classification recognizes the following subtypes:
1. Relapsing-Remitting MS (RRMS)
The most common form (~85% of patients at onset). Characterized by discrete attacks (relapses) with partial or complete recovery between episodes, during which neurologic function is stable. The female:male ratio is 2–3:1. Mean age of onset is ~30 years.
With highly effective disease-modifying therapies (DMTs), relapses can be largely abolished in most patients. However, "silent progression" — termed progression independent of relapsing activity (PIRA) — is now recognized as an important driver of disability even in the relapsing phase, occurring without clinical attacks.
2. Secondary Progressive MS (SPMS)
In the pretreatment era, ~80% of RRMS patients evolved to SPMS within 25 years (~3% per year). With modern therapy, this rate has fallen to <1% per year. SPMS is defined by a steady neurological decline following an initial relapsing course. Patients may still experience superimposed relapses (termed active SPMS). An EDSS ≥4 plus a motor FSS score ≥2 can support a diagnosis of SPMS. - Harrison's Principles of Internal Medicine 22E, p. 3623
3. Primary Progressive MS (PPMS)
Accounts for ~10% of cases. No discrete relapses — patients steadily decline from onset. Key distinguishing features:
- Near-equal sex distribution (unlike RRMS)
- Later onset (mean ~40 years)
- Faster disability accumulation relative to first symptom
- Despite these differences, PPMS appears to share the same underlying disease biology as RRMS/SPMS
- Some PPMS patients experience relapses; these are termed active progressive MS
4. Clinically Isolated Syndrome (CIS)
A first demyelinating episode that is clinically consistent with MS but does not yet satisfy McDonald criteria for dissemination in space and time. 70–80% of CIS patients with MRI abnormalities will develop clinically definite MS (CDMS) over 10–14 years; only ~20% of those with a normal brain MRI will develop MS. - Bradley and Daroff's Neurology in Clinical Practice, p. 1727
5. Radiologically Isolated Syndrome (RIS)
Incidental MRI findings typical of MS discovered without any clinical syndrome. RIS patients with enhancing lesions and spinal cord lesions are at higher risk for conversion to CIS/MS.
Clinical Features
Presenting Symptoms (Frequency at Onset)
| Symptom | % of cases |
|---|---|
| Sensory loss | 37% |
| Optic neuritis | 36% |
| Weakness | 35% |
| Paresthesias | 24% |
| Diplopia | 15% |
| Ataxia | 11% |
| Vertigo | 6% |
| Bladder symptoms | 4% |
| Paroxysmal attacks | 4% |
Source: Harrison's Principles of Internal Medicine 22E, citing Swingler & Compston, 1992
Cranial Nerve & Visual Dysfunction
Optic neuritis (ON) is a frequent presenting symptom. It manifests as:
- Acute/subacute unilateral visual loss with periorbital pain worsened by eye movement
- Relative afferent pupillary defect (Marcus Gunn pupil)
- Central or cecocentral scotoma
- 90% of patients regain normal or near-normal vision within 2–6 months
- Bilateral simultaneous ON is rare in MS and should prompt consideration of neuromyelitis optica (NMOSD), anti-MOG antibody disease, or Leber hereditary optic neuropathy
Internuclear ophthalmoplegia (INO) is highly characteristic of MS. It results from a medial longitudinal fasciculus (MLF) lesion and presents with:
- Impaired adduction of the ipsilateral eye
- Horizontal nystagmus in the abducting eye
- Preserved convergence
- Bilateral INO is virtually pathognomonic of MS
Other ocular motor findings: acquired pendular nystagmus (oscillopsia), horizontal gaze palsy, "one-and-a-half" syndrome (gaze palsy + INO). - Bradley and Daroff's Neurology in Clinical Practice, p. 1715
Motor & Pyramidal Dysfunction
Weakness is upper motor neuron (UMN) in character, accompanied by:
- Spasticity, hyperreflexia, extensor plantar responses
- Exercise-induced weakness — characteristic of MS
- Spastic paraparesis is a common late manifestation of spinal cord involvement
- Occasionally a reflex may appear depressed if a plaque disrupts afferent fibers in the dorsal cord, mimicking a peripheral lesion
Spasticity is common and may cause painful flexor/extensor spasms. Paradoxically, some patients rely on spasticity for weight-bearing support, so treatment must be individualized.
Sensory Dysfunction
Sensory symptoms are the most common presenting complaint. They include:
- Numbness, tingling, paresthesias — often in a hemibody or ascending "cape" distribution
- Decreased proprioception and vibration sense (posterior column involvement)
- Lhermitte's symptom: electric shock-like sensation radiating down the spine into legs, triggered by neck flexion — indicates a cervical cord lesion
Cerebellar & Brainstem Dysfunction
- Ataxia and intention tremor (cerebellar tremors, Chap. 450)
- Scanning (cerebellar) dysarthria — slow, irregular speech
- Vertigo from brainstem lesions may mimic acute labyrinthitis
- Trigeminal neuralgia in MS is characteristically bilateral or in a patient <50 years old — atypical features prompt MS workup
- Facial myokymia — rhythmic flickering of facial muscles from corticobulbar/brainstem lesion
Autonomic & Urological Dysfunction
Bladder symptoms are ultimately present in most MS patients:
- Detrusor hyperreflexia (impaired suprasegmental inhibition) → urgency, frequency, nocturia, incontinence
- Detrusor-sphincter dyssynergia → hesitancy, retention, overflow incontinence, recurrent UTIs
- Constipation is common; fecal incontinence less so but socially debilitating
- Sexual dysfunction: impotence in men, decreased libido, diminished vaginal lubrication or adductor spasms in women - Harrison's, p. 3622
Cognitive & Psychiatric Features
- Cognitive dysfunction in ~50% of patients (often mild): impaired attention, memory loss, slowed information processing, executive dysfunction
- Frank dementia sufficient to impair ADLs is rare
- Depression affects ~50% of patients; risk of suicide is 2–7× higher than the general population
- Euphoria and pseudobulbar affect (once considered characteristic) are actually relatively uncommon
- Fatigue is a strong predictor of depression in MS
Paroxysmal Phenomena
Paroxysmal symptoms are brief (10 seconds to 2 minutes), high-frequency (5–40 episodes/day), self-limited, and lack altered consciousness. They likely arise from spontaneous discharges at plaque edges. Examples:
- Tonic seizures (tonic contractions of a limb or trunk)
- Paroxysmal dysarthria and ataxia
- Paroxysmal sensory disturbances
Uhthoff's Phenomenon (Heat Sensitivity)
Transient worsening of neurologic symptoms with elevated core temperature (hot shower, exercise, fever). Results from conduction block in demyelinated axons. Not a true relapse — symptoms resolve with cooling.
Prognostic Factors
| Feature | Favorable | Unfavorable |
|---|---|---|
| Sex | Female | Male |
| Age at onset | Young (<30) | Older (>40) |
| Initial course | Relapsing | Progressive |
| Initial symptoms | Sensory, ON | Motor, cerebellar |
| MRI lesion burden | Low | High |
| Relapse frequency | Low | High (short inter-attack interval) |
Bradley and Daroff's Neurology, p. 1727
Representative MRI Findings
MS lesions on MRI show characteristic distributions:

Sources:
- Bradley and Daroff's Neurology in Clinical Practice — Ch. 80 (MS Clinical Features, Course & Prognosis)
- Harrison's Principles of Internal Medicine 22E — Ch. 455 (Multiple Sclerosis)
This is a shared conversation. Sign in to Orris to start your own chat.