please show me amyloidosis based images referring from Robbins and Cotran pathology derived from inciet pyqs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
All 5 images are now retrieved. Let me compile the comprehensive, image-rich answer.
Amyloidosis - Robbins & Cotran Pathologic Basis of Disease
Here are all the key Robbins images for amyloidosis, organized by concept - highly relevant for INICET/PG entrance exam preparation.
IMAGE 1 - Mechanism of Amyloid Deposition (Fig. 6.44 / Robbins & Cotran)
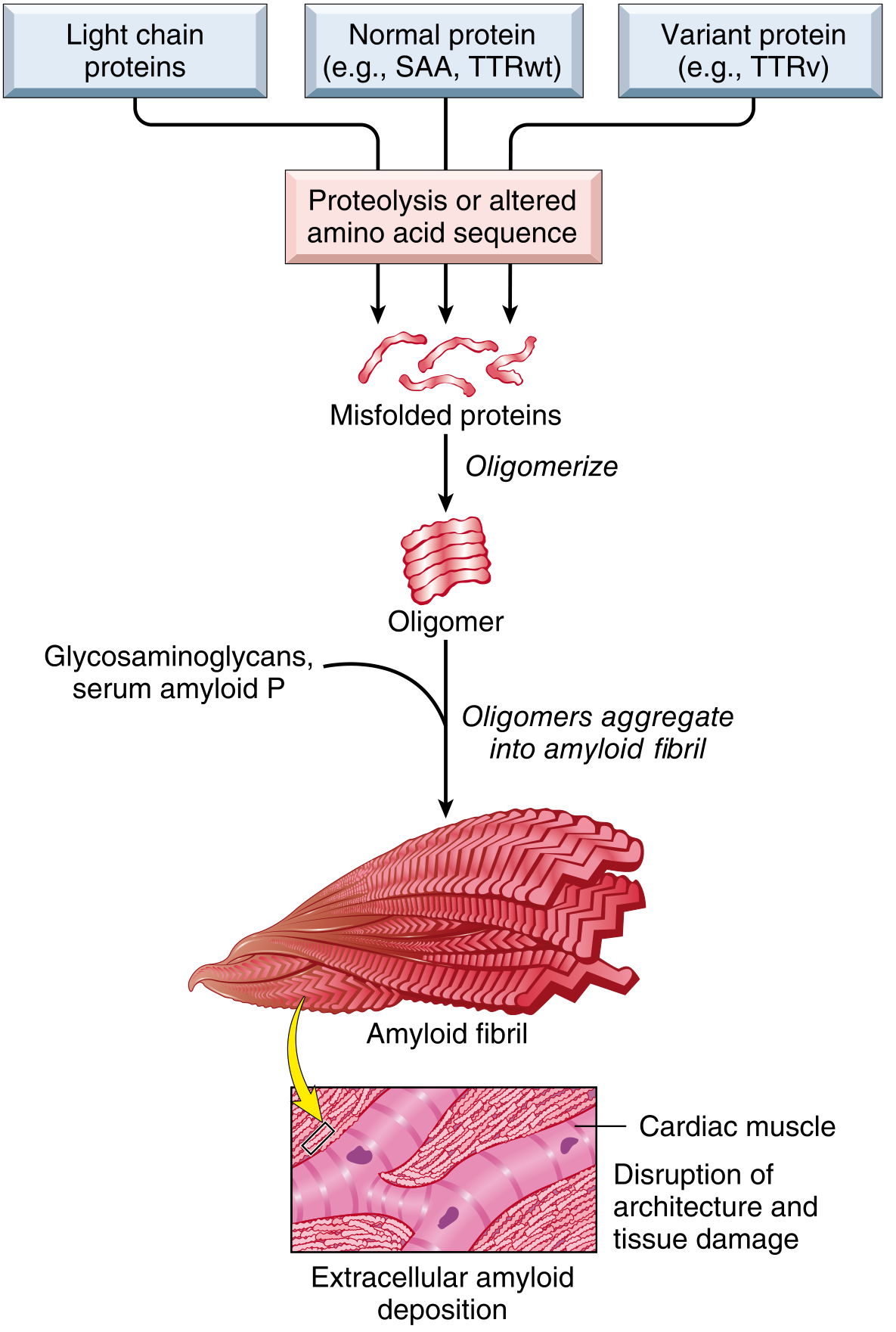
What this shows: Light chain proteins, normal proteins (SAA, TTRwt), and variant proteins (TTRv) all undergo proteolysis or altered amino acid sequence → produce misfolded proteins → oligomerize → aggregate into amyloid fibrils → deposit extracellularly in tissues (shown in cardiac muscle) → disruption of architecture and tissue damage.
Exam point: All amyloid proteins converge on the same final common pathway - misfolded protein → β-pleated fibril → extracellular deposition.
IMAGE 2 - Pathogenesis of Amyloidosis (Fig. 6.45 / Robbins & Cotran)
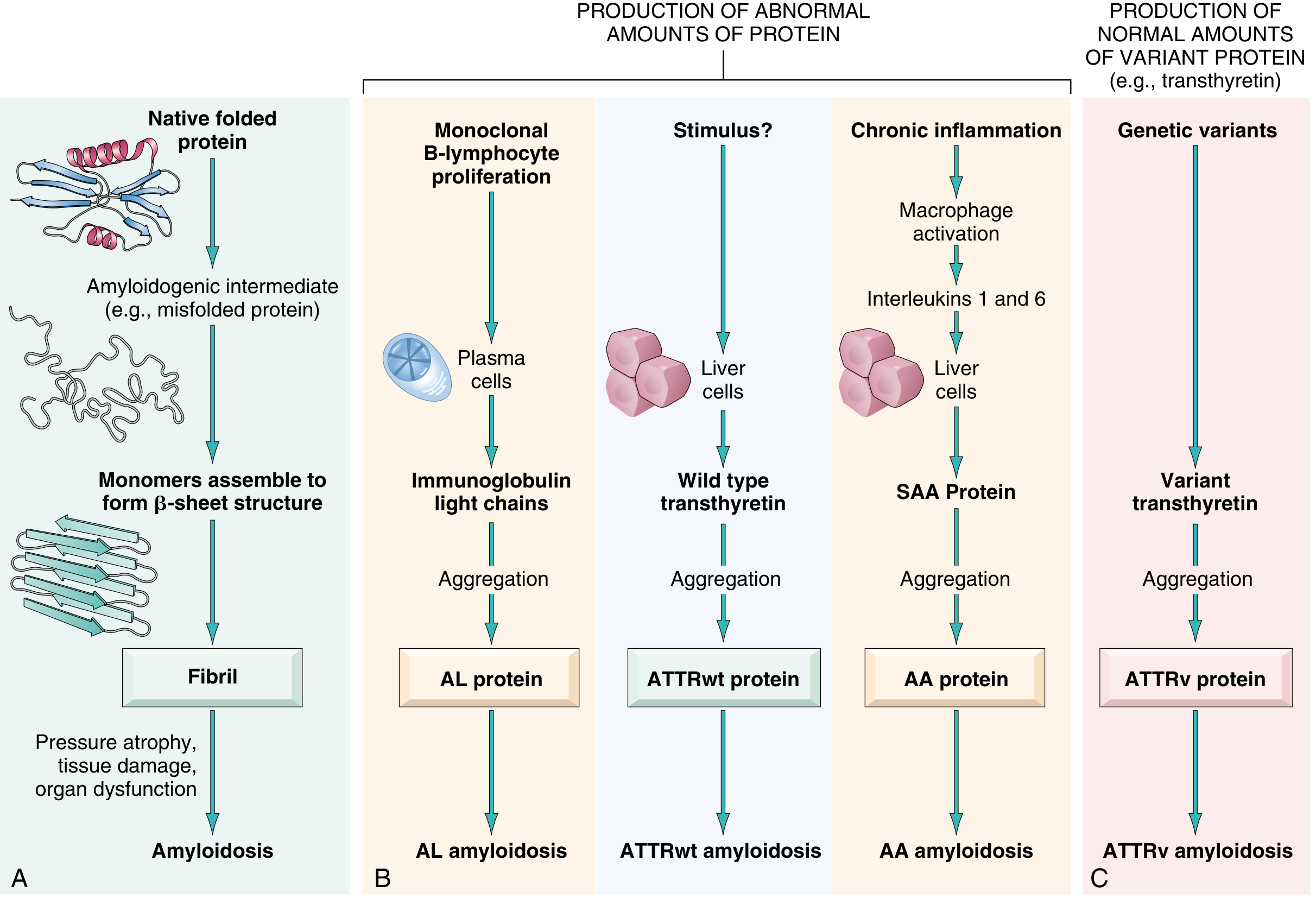
What this shows: A comprehensive pathogenesis diagram with 4 pathways:
| Pathway | Source | Protein | Type |
|---|---|---|---|
| Monoclonal B-cell/plasma cell proliferation | Plasma cells | Immunoglobulin light chains | AL amyloidosis |
| Aging/unknown stimulus | Liver cells (wild-type) | Wild-type transthyretin | ATTRwt amyloidosis |
| Chronic inflammation (macrophage activation → IL-1, IL-6) | Liver cells | SAA protein | AA amyloidosis |
| Genetic variants | Liver cells (variant TTR) | Variant transthyretin | ATTRv amyloidosis |
The left panel shows the general mechanism: native folded protein → amyloidogenic intermediate → monomers assemble into β-sheet structure → fibril → pressure atrophy, tissue damage, organ dysfunction.
Exam point (INICET favourite): AA amyloidosis is the type associated with chronic inflammatory diseases (rheumatoid arthritis, tuberculosis, Crohn disease). The precursor protein is SAA (Serum Amyloid A), synthesized in the liver.
IMAGE 3 - Amyloid Structure (Fig. 5.35 / Robbins Basic Pathology)
Panel A - Amyloid fibril schematic:
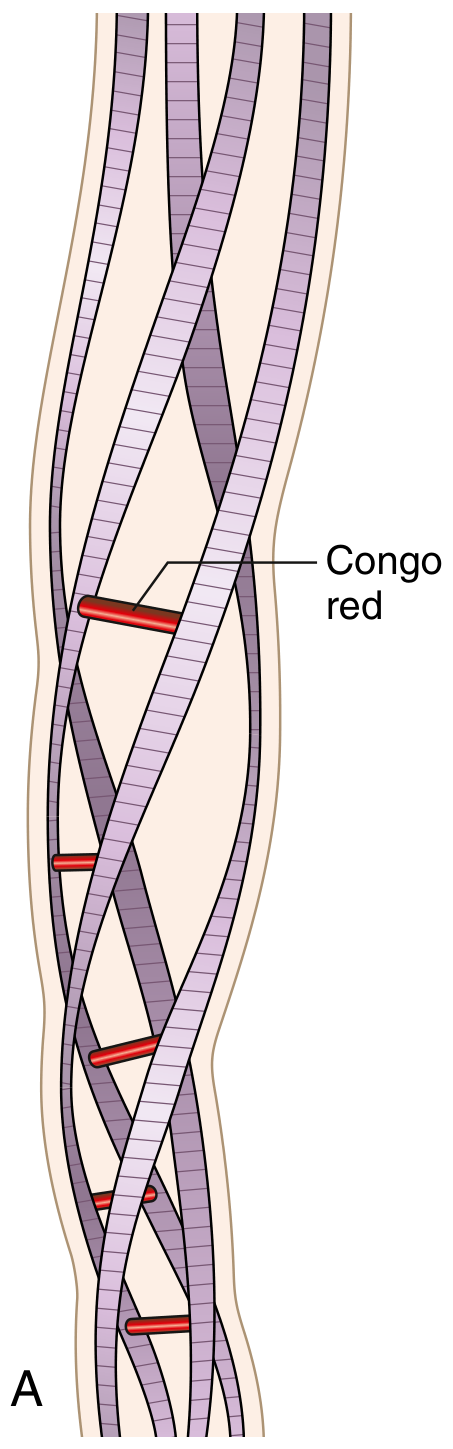
What this shows: Schematic of an amyloid fiber with four fibrils wound around one another. The Congo red dye (shown in red) binds at regularly spaced intervals along the β-pleated sheet conformation.
Panel B - Apple-green birefringence under polarized light:
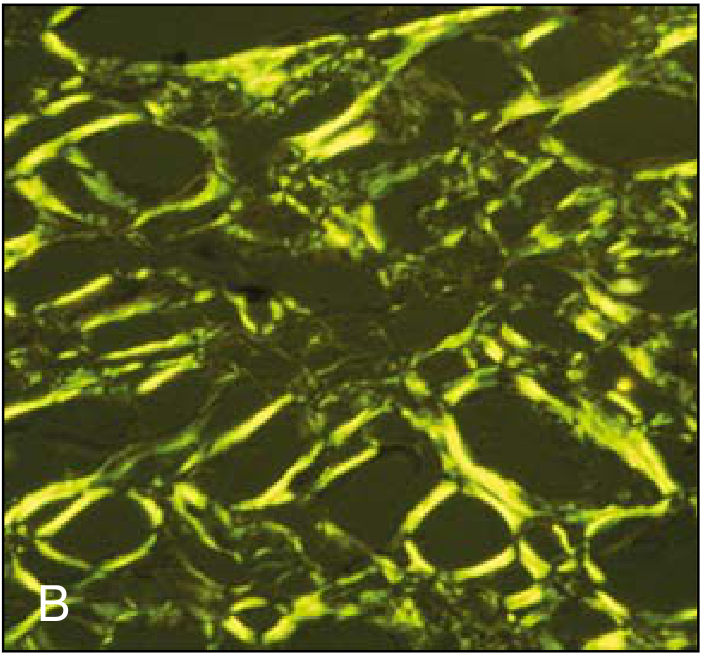
What this shows: Congo red stained amyloid viewed under polarized light - the pathognomonic apple-green (yellow-green) birefringence. This is the most specific diagnostic stain for amyloid.
Top INICET exam point: Congo red stain → pink/red under ordinary light; apple-green birefringence under polarized light - this is diagnostic. The birefringence is due to the cross β-pleated sheet configuration of amyloid fibrils.
IMAGE 4 - Histology: Congo Red Stain + Renal Amyloidosis (Fig. 6.46 / Robbins & Cotran; also Fig. 5.37 / Robbins Basic Pathology)
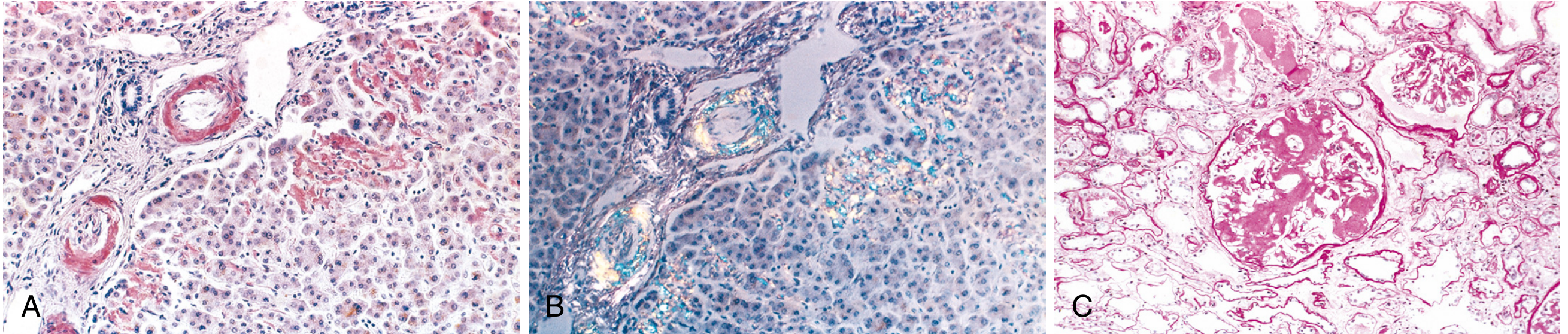
Panel A - Liver section stained with Congo red: pink-red amyloid deposits in walls of blood vessels and along sinusoids (space of Disse).
Panel B - Same field under polarizing microscope: yellow-green birefringence of the Congo red-stained deposits. This is the gold standard for amyloid diagnosis.
Panel C - Kidney amyloidosis: The glomerular architecture is almost totally obliterated by massive accumulation of amyloid (pink homogeneous material). The capillary loops are obliterated by confluent amyloid masses.
Exam points from this image:
- Kidney is the most common and most serious organ involved in systemic amyloidosis
- Amyloid begins in the mesangium and along the glomerular basement membrane
- Leads to nephrotic syndrome → renal failure → most common cause of death in amyloidosis
- In liver: amyloid first appears in the space of Disse (between hepatocytes and sinusoids)
Classification Table (Table 6.17 / Robbins & Cotran)
| Category | Associated Disease | Fibril Protein | Precursor |
|---|---|---|---|
| AL amyloidosis | Multiple myeloma, monoclonal plasma cell proliferation | AL | Ig light chains (chiefly λ) |
| ATTRwt amyloidosis | Aging (males >70 years) - senile systemic amyloidosis | ATTRwt | Wild-type transthyretin |
| AA amyloidosis | Chronic inflammation (RA, Crohn, TB) | AA | SAA protein |
| ATTRv amyloidosis | Familial amyloidotic neuropathy, cardiac amyloidosis | ATTRv | Variant transthyretin |
| Aβ | Alzheimer disease (senile plaques) | Aβ | APP (amyloid precursor protein) |
| Endocrine | Type 2 DM (islets), medullary thyroid carcinoma | AIAPP / ACal | Islet amyloid peptide / Calcitonin |
Key INICET Exam Points - Amyloidosis
| Feature | Detail |
|---|---|
| Staining | Congo red → pink-red (light); apple-green birefringence (polarized) |
| Fibril diameter | ~8-10 nm, non-branching, β-pleated sheet conformation |
| ~95% composition | Fibril proteins; 5% = serum amyloid P (SAP) + glycoproteins |
| Most common type | AL amyloidosis (~2000-3000 new cases/year in USA) |
| Sago spleen | Amyloid limited to splenic follicles (white pulp) |
| Lardaceous spleen | Amyloid in splenic sinuses (red pulp) - maplike areas |
| Most common cause of death | Renal failure (kidneys most commonly and seriously involved) |
| Cardiac amyloidosis presents as | Restrictive cardiomyopathy + arrhythmias |
| Diagnosis | Rectal biopsy / abdominal fat aspirate stained with Congo red; abdominal fat most specific |
| Endocrine amyloid in medullary thyroid Ca | Derived from calcitonin - a helpful diagnostic feature |
| β₂-microglobulin amyloid | Old complication of dialysis (now rare with improved membranes) - carpal tunnel syndrome |
| Macroglossia | AL amyloidosis involving tongue (tumour-forming amyloid) |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (ISBN 9780443264528), Figs. 6.44, 6.45, 6.46; Robbins & Kumar Basic Pathology (ISBN 9780323790185), Figs. 5.35, 5.37
bio film catheter meaning
Reading File
Searching the Web
biofilm catheter definition formation clinical significance
Finding Sources
Reading File
Reading File
Loading Image
Biofilm on a Catheter
What is a Biofilm?
A biofilm is a structured, organized community of microorganisms that adhere to a surface (like a catheter) and surround themselves in a self-produced extracellular matrix made of polysaccharides, proteins, and host components. Think of it as bacteria building their own protected "fortress" on the catheter surface.
Scanning Electron Microscopy - S. epidermidis Biofilm on Catheter
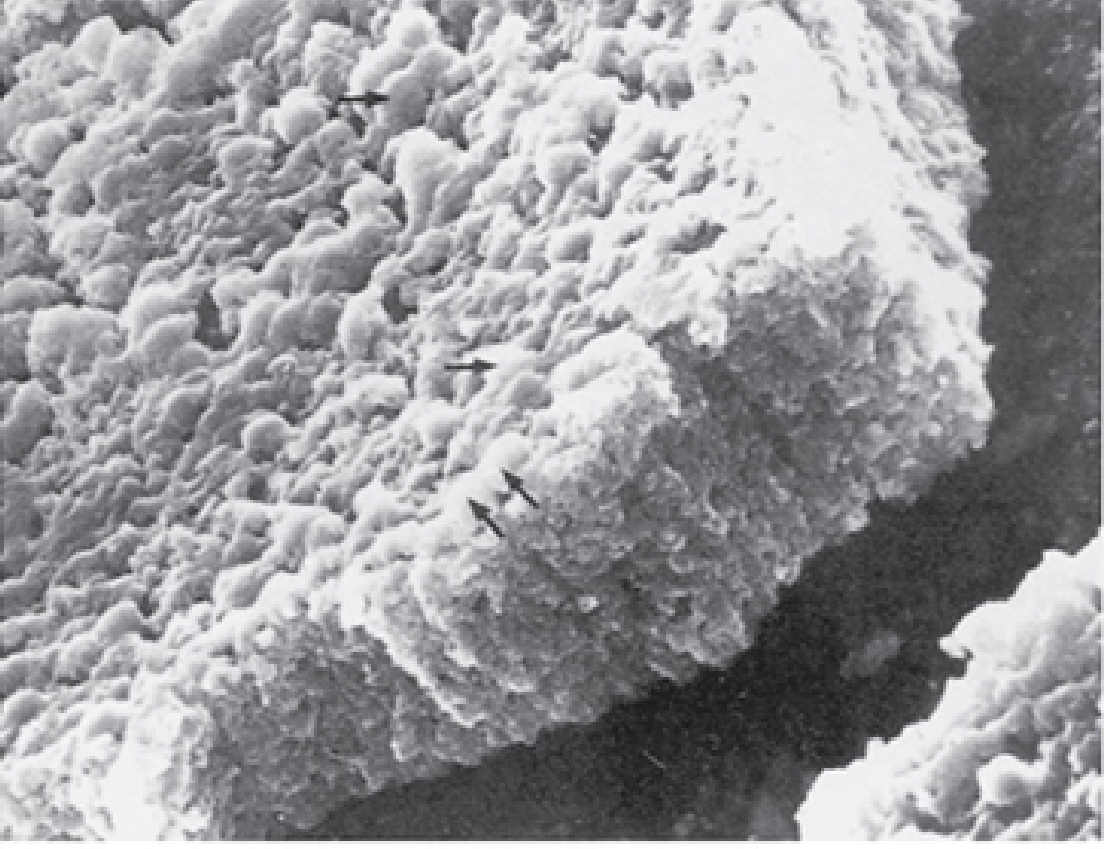
This scanning electron micrograph shows Staphylococcus epidermidis cocci fully embedded in the slime glycocalyx (biofilm) on a plastic catheter surface after 48 hours. The arrows point to individual cocci beneath the polysaccharide slime.
How a Catheter Biofilm Forms - Step by Step
| Step | What Happens |
|---|---|
| 1. Conditioning layer | Immediately after catheter insertion, host proteins (fibronectin, Tamm-Horsfall protein, Mg²⁺, Ca²⁺ ions) coat the catheter surface |
| 2. Initial adhesion | Bacteria adhere to this conditioning layer via surface adhesins |
| 3. Microcolony formation | Adherent bacteria multiply and cluster together |
| 4. Biofilm maturation | Bacteria produce extracellular polysaccharide (EPS) - the slime/glycocalyx - encasing the whole colony |
| 5. Dispersal | Pieces of biofilm detach and spread to new surfaces, seeding infection elsewhere |
Why Biofilms are Clinically Dangerous
- Antibiotic resistance: The EPS matrix acts as a physical barrier that prevents antibiotics from penetrating and reaching bacteria. Organisms in biofilms can be 100-1000x more resistant to antibiotics than free-floating (planktonic) bacteria.
- Immune evasion: Protected from neutrophils, complement, and host immune defenses.
- Slow growth: Bacteria in biofilms often grow slowly, making antibiotics (which target active metabolism) even less effective.
- Persistent seeding: Biofilm acts as a chronic reservoir - bacteria shed from the biofilm cause repeated episodes of bacteremia or UTI.
- Device-associated infection: Removal of the contaminated device is often the only sure way to eliminate infection.
Organisms Commonly Forming Catheter Biofilms
| Organism | Catheter Type | Notes |
|---|---|---|
| S. epidermidis (CoNS) | IV catheters, CVCs | #1 colonizer of IV devices; produces slime (polysaccharide intercellular adhesin) |
| S. aureus | Any device | Less common but more aggressive; metastatic infections |
| E. coli / Gram-negatives | Urinary catheters | Most common in CAUTI |
| Proteus mirabilis | Urinary catheters | Produces urease → alkaline pH → crystalline biofilm → catheter obstruction (~80% of blocked catheters) |
| Candida spp. | IV/urinary catheters | Fungal biofilm; common in immunocompromised/diabetics |
Types of Catheter Biofilm Infection
1. Catheter-Associated UTI (CAUTI)
- Bacteria enter at the urethral orifice or drainage bag, biofilm ascends the catheter
- Bacteriuria rate: 3-7% per day with indwelling urinary catheter
- Initially single organism; becomes polymicrobial in chronic catheters
- Proteus mirabilis causes crystalline biofilm → can obstruct the catheter
2. Central Line-Associated Bloodstream Infection (CLABSI)
- Biofilm forms on inner lumen of central venous catheters (CVCs)
- Common in ICU patients - a major cause of nosocomial sepsis
3. Hemodialysis Catheter Infection
- Biofilm forms on tunneled HD catheters; thrombus inside catheter acts as a nidus for biofilm
- Management: antibiotic lock therapy ± catheter exchange over guidewire
Key Clinical Points
- "Low-grade fever" in a patient with an indwelling device = think biofilm infection until proven otherwise
- Diagnosis: blood cultures (for CLABSI) or urine culture (for CAUTI)
- Treatment: systemic antibiotics + device removal/exchange - antibiotics alone rarely cure biofilm infections
- Antibiotic lock therapy (instilling high-concentration antibiotic directly into catheter lumen) is used for catheter salvage in CLABSI
- Prevention: antimicrobial-coated catheters, minimizing catheter dwell time, aseptic technique
Sources: Sherris & Ryan's Medical Microbiology 8th Ed, Fig. 24-9; Goldman-Cecil Medicine; Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.