Regulation of blood glucose
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks and two excellent diagrams. Let me compile the full answer.
Regulation of Blood Glucose
Blood glucose is maintained within a narrow range - 80-90 mg/dL (4.4-5.0 mmol/L) fasting, rising to 120-140 mg/dL in the first hour after a meal before being returned to baseline within 2 hours. This tight control is achieved through a coordinated network of hormones, the liver, and the autonomic nervous system.
Why Tight Regulation Matters
Glucose is the obligate fuel for the brain, retina, and germinal epithelium of the gonads - these tissues cannot effectively use fatty acids or amino acids as alternatives. Simultaneously, persistent hyperglycemia drives glycation of proteins and vascular damage. This dual pressure - avoid hypoglycemia AND hyperglycemia - explains the precision of the system.
- Guyton and Hall Textbook of Medical Physiology, p. 972
The Major Players
1. The Liver - The Primary Buffer
The liver acts as a glucose "buffer system." After a meal:
- Up to two-thirds of absorbed glucose is rapidly stored as glycogen in the liver (glycogenesis).
- As glucose and insulin levels fall in the hours after eating, the liver releases glucose back via glycogenolysis.
- This buffering alone reduces blood glucose fluctuations to about one-third of what they would be otherwise.
During prolonged fasting, the liver (and kidneys) generate glucose from non-carbohydrate substrates via gluconeogenesis - using lactate, pyruvate, alanine, glutamate (from muscle) and glycerol (from adipose lipolysis).
- Guyton and Hall Textbook of Medical Physiology, p. 972
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 1043
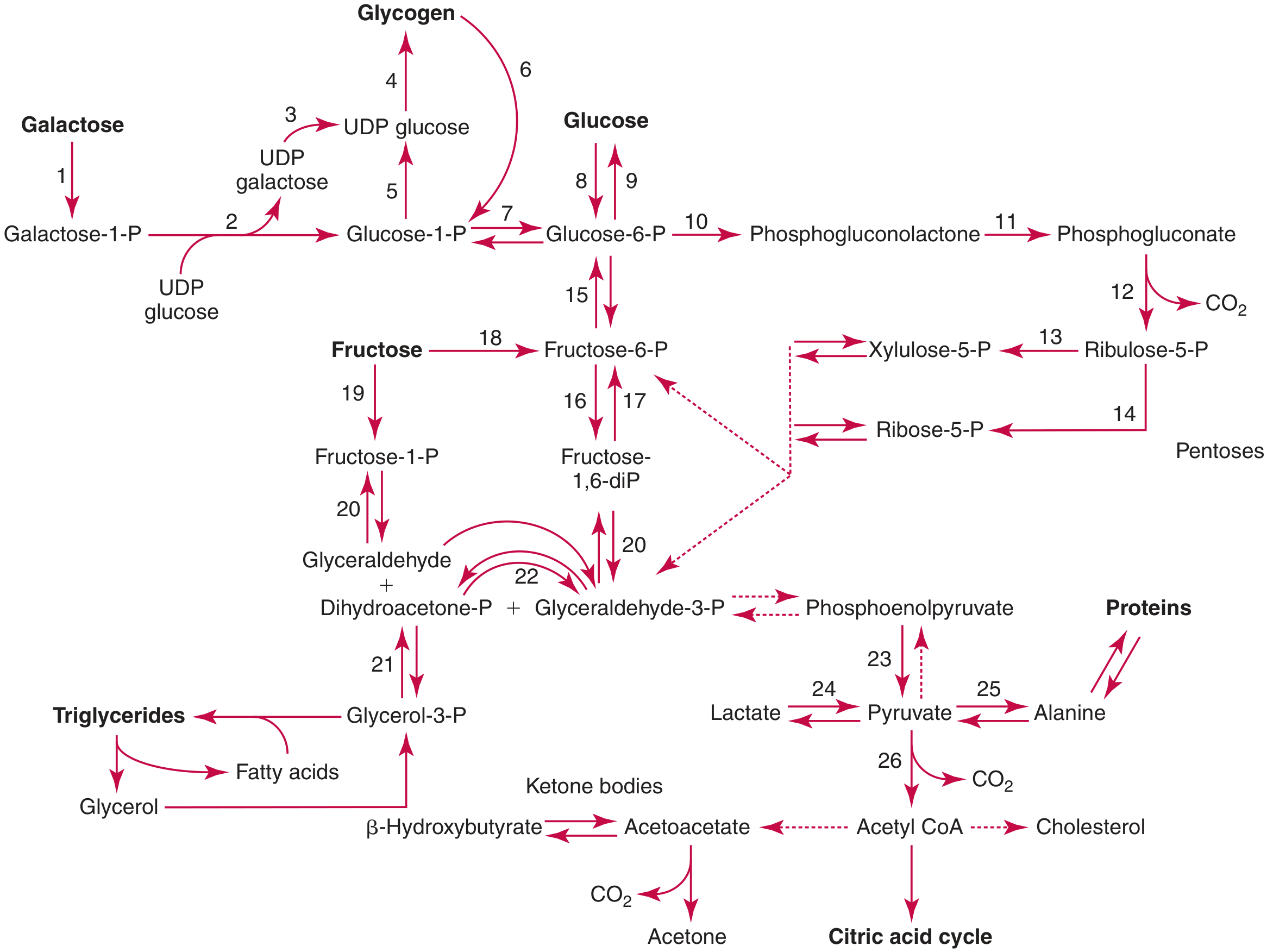
Major metabolic pathways of carbohydrate - Tietz Textbook of Laboratory Medicine
2. Insulin - The Key Anabolic Signal
Source: Pancreatic beta (β) cells of the islets of Langerhans.
Primary stimulus: Rising plasma glucose. At fasting glucose levels (80-100 mg/dL), insulin secretion is at basal rates. Above this threshold, insulin release rises steeply - reaching 10 to 25 times the basal rate at glucose concentrations of 400-600 mg/dL.
Biphasic secretion pattern:
- First phase (within 3-5 min): rapid release of preformed insulin from storage granules.
- Second phase (15 min onwards, peaking at 2-3 hours): additional preformed release plus newly synthesized insulin.
Additional stimuli for insulin secretion:
| Stimulus | Mechanism |
|---|---|
| Amino acids (arginine, lysine) | Potentiate glucose-driven secretion; double the rate when glucose is also elevated |
| GLP-1 and GIP (incretins) | Released from gut after eating; anticipatory feed-forward boost of insulin before glucose peaks |
| Glucagon (paracrine) | Potent insulin secretagogue |
| GH, cortisol, estrogen, progesterone | Potentiate glucose stimulus |
| Sympathetic nervous system | Pre-meal neural signals prime secretion |
Actions of insulin on glucose regulation:
- Increases GLUT-4 mediated glucose uptake in muscle and adipose tissue.
- Promotes hepatic glycogenesis (glucose → glycogen storage).
- Promotes glycolysis and inhibits gluconeogenesis and glycogenolysis in the liver.
- Promotes lipogenesis; inhibits lipolysis (reducing gluconeogenic substrate supply).
- Promotes protein synthesis (reduces amino acid availability for gluconeogenesis).
The feedback loop is rapid: glucose rises → insulin secretion increases → glucose uptake and storage increase → glucose returns to normal. Turnoff of insulin secretion occurs within 3-5 minutes of glucose returning to fasting levels.
- Guyton and Hall Textbook of Medical Physiology, p. 967-970
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 1043
3. Glucagon - The Catabolic Counter-Hormone
Source: Pancreatic alpha (α) cells.
Stimuli for glucagon secretion:
- Amino acids (major physiological stimulus - particularly after a protein meal)
- Falling blood glucose (hypoglycemia)
- Inhibited by: rising glucose and GLP-1
Actions on the liver (primary target):
- Stimulates glycogenolysis (rapid glucose release from glycogen).
- Stimulates gluconeogenesis (new glucose synthesis from lactate, alanine, glycerol).
- Stimulates ketogenesis during prolonged fasting.
- Acts via cAMP-dependent protein kinase A pathway.
At pharmacological concentrations glucagon also causes glycogenolysis in cardiac and skeletal muscle, lipolysis in adipose tissue, and proteolysis - but at physiological levels the liver is the dominant target.
Glucagon and insulin function as a paired feedback system: when glucose rises, insulin dominates; when glucose falls, glucagon dominates. The insulin feedback mechanism is more important under normal day-to-day conditions, but glucagon becomes indispensable during starvation, intense exercise, or stress.
- Medical Physiology (Boron & Boulpaep), p. 1541
4. The Incretin System (Gut-Pancreas Axis)
Two hormones released from the gut mucosa after nutrient ingestion play a key anticipatory role:
- GLP-1 (glucagon-like peptide-1) - from intestinal L cells
- GIP (glucose-dependent insulinotropic polypeptide) - from K cells
Both are released in proportion to the ingested nutrient load and amplify the β-cell insulin response before blood glucose even peaks (feed-forward mechanism). GLP-1 also suppresses glucagon from α cells, providing dual control. These are targets of major drug classes (GLP-1 receptor agonists, DPP-4 inhibitors).
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 1043-1044
5. Somatostatin - The Modulator
Source: Delta (δ) cells of the islets of Langerhans.
Somatostatin inhibits both insulin and glucagon secretion. Its proposed role is to extend the time window over which absorbed nutrients enter the bloodstream, preventing both excessively rapid glucose uptake (that could cause hypoglycemia) and excessively fast nutrient exhaustion. It is identical to hypothalamic GHRH-inhibiting hormone (growth hormone inhibitory hormone).
6. Counterregulatory Hormones - Defence Against Hypoglycemia
When blood glucose falls below normal, a hierarchy of defenses is activated in sequence:
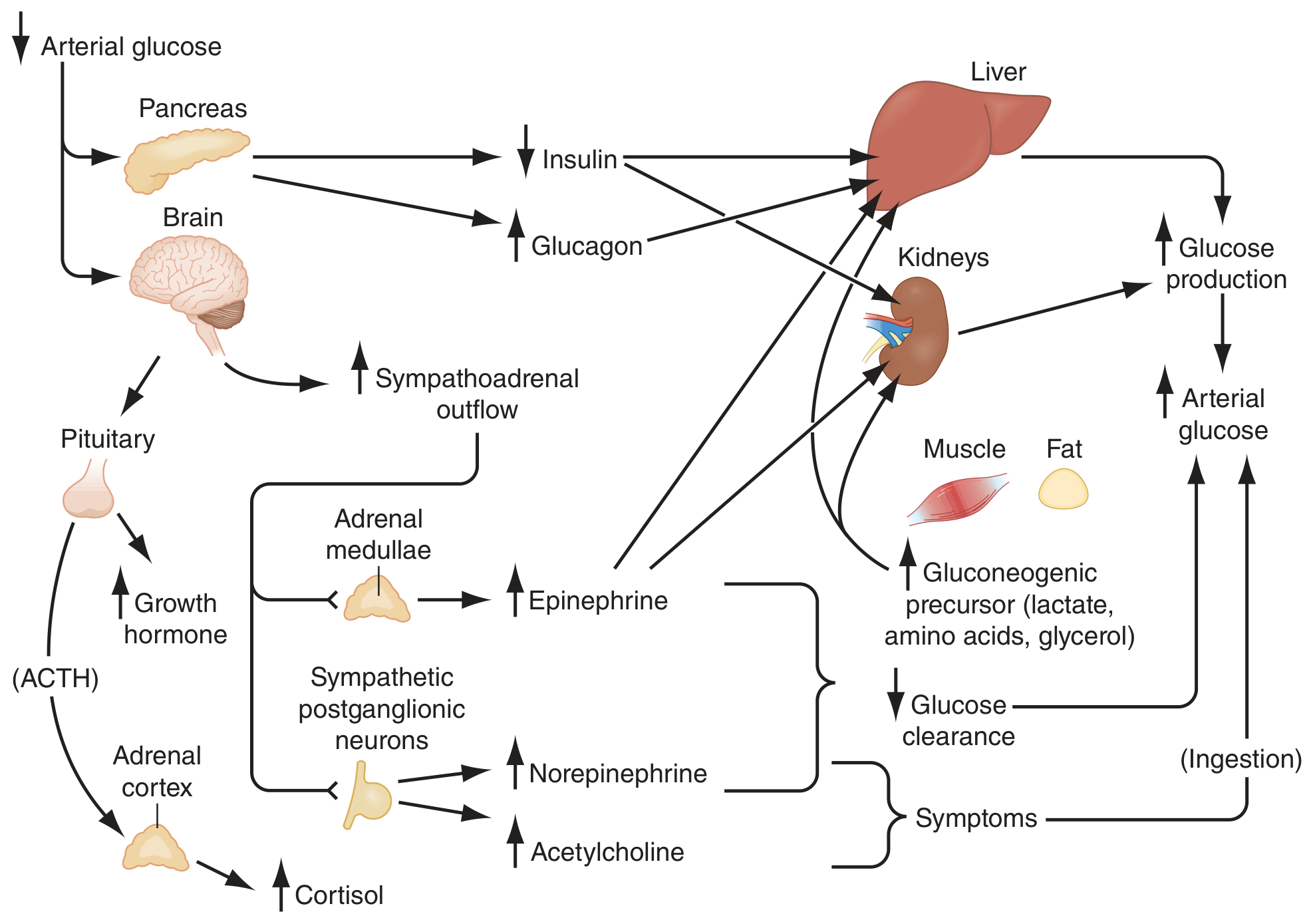
Physiology of glucose counterregulation - Harrison's Principles of Internal Medicine 22e
| Glucose threshold | Response | Mechanism |
|---|---|---|
| 4.4-4.7 mmol/L (80-85 mg/dL) | ↓ Insulin | 1st defense - releases brake on hepatic glucose output and peripheral uptake |
| 3.6-3.9 mmol/L (65-70 mg/dL) | ↑ Glucagon | Stimulates hepatic glycogenolysis + gluconeogenesis (primary counterregulatory hormone) |
| 3.6-3.9 mmol/L (65-70 mg/dL) | ↑ Epinephrine | Stimulates hepatic + renal gluconeogenesis; limits peripheral glucose uptake; stimulates lipolysis releasing glycerol + FFAs; becomes critical when glucagon is deficient |
| ~3.0 mmol/L (55 mg/dL) | ↑ Growth hormone | Decreases peripheral glucose utilization; shifts to fat oxidation |
| ~3.0 mmol/L (55 mg/dL) | ↑ Cortisol | Same as GH; acts over hours-days |
| Severe hypoglycemia | Sympathetic activation | Hypothalamus → sympathoadrenal outflow → adrenal medulla → epinephrine burst; also causes symptoms (tremor, sweating, tachycardia) that prompt eating |
Note: Cortisol and GH are not significant defenses against acute hypoglycemia (their effects are reduced ~80% vs. epinephrine) - they matter in prolonged hypoglycemia over hours.
- Harrison's Principles of Internal Medicine 22e, p. 3275
- Basic Medical Biochemistry - A Clinical Approach, 6e
Key Metabolic Pathways Involved
| Pathway | Direction | Regulation |
|---|---|---|
| Glycogenesis | Glucose → Glycogen | Stimulated by insulin (activates glycogen synthase) |
| Glycogenolysis | Glycogen → Glucose | Stimulated by glucagon/epinephrine (activate phosphorylase via cAMP) |
| Glycolysis | Glucose → Pyruvate | Stimulated by insulin; inhibited in fasting |
| Gluconeogenesis | Lactate/amino acids/glycerol → Glucose | Stimulated by glucagon/cortisol; inhibited by insulin |
| Lipolysis | Triglycerides → FA + Glycerol | Stimulated by glucagon, GH, cortisol, epinephrine; inhibited by insulin |
| Ketogenesis | Acetyl-CoA → Ketone bodies | Active in prolonged fasting/insulin deficiency |
| Pentose phosphate pathway | Glucose → NADPH + pentoses | Insulin-responsive; provides reductive power |
Two key kinases regulate the switch between anabolic (fed) and catabolic (fasting) states:
-
cAMP-dependent protein kinase A (PKA) - activated by glucagon/epinephrine; shifts liver toward glucose output
-
AMP-activated protein kinase (AMPK) - activated by low energy states; promotes fat oxidation, inhibits glucose-consuming pathways
-
Basic Medical Biochemistry - A Clinical Approach, 6e, p. 1582
-
Tietz Textbook of Laboratory Medicine, 7th ed., p. 1131
Summary: Fed vs. Fasting State
| State | Dominant hormone | Liver | Muscle/Fat |
|---|---|---|---|
| Fed (postprandial) | Insulin | Glycogenesis, glycolysis, lipogenesis, ↓ gluconeogenesis | Glucose uptake (GLUT-4), glycogen storage, protein synthesis, lipogenesis |
| Fasting (overnight) | Glucagon/↓Insulin | Glycogenolysis → gluconeogenesis as glycogen depletes | Lipolysis, fatty acid oxidation, proteolysis (releases gluconeogenic AAs) |
| Prolonged fasting/starvation | Glucagon + cortisol + GH | Sustained gluconeogenesis, ketogenesis | Fat becomes dominant fuel; protein catabolism accelerates |
The brain is protected throughout - it receives glucose from the liver during fasting, and can switch partially to ketone bodies after several days of starvation.
Regulation of blood glucose biochemistry
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Regulation of Blood Glucose - Biochemistry
Blood glucose is maintained between 70-140 mg/dL (3.9-7.8 mmol/L) through a tightly integrated network of biochemical mechanisms operating at three levels: glucose transport into cells, enzymatic regulation of metabolic pathways, and hormonal signaling cascades. These work across a spectrum of speed - from millisecond allosteric changes to hours-long transcriptional responses.
1. Glucose Entry into Cells - The GLUT Transporters
Glucose crosses cell membranes via facilitated diffusion through a family of 14 GLUT (glucose transporter) isoforms - monomeric proteins with 12 transmembrane alpha-helices that alternate between two conformations to carry glucose down its concentration gradient (no energy required).
| Transporter | Location | Km (mM) | Key Feature |
|---|---|---|---|
| GLUT-1 | Most tissues, RBCs, blood-brain barrier | 1 | High affinity; basal, constitutive uptake |
| GLUT-2 | Liver, kidneys, pancreatic β cells | 15-20 | Low affinity, high capacity; functions as a glucose sensor |
| GLUT-3 | Brain (neurons) | 1 | High affinity; ensures neuronal glucose supply |
| GLUT-4 | Skeletal muscle, adipose, cardiac muscle | 5 | Insulin-sensitive - translocates from intracellular vesicles to plasma membrane in response to insulin |
| GLUT-5 | Small intestine, testes | 10 | Primarily a fructose transporter |
The GLUT-2/glucokinase system is central to glucose sensing:
-
GLUT-2 has a high Km (15-20 mM), so glucose enters the β cell in proportion to blood glucose concentration.
-
Once inside, glucokinase (hexokinase IV) phosphorylates glucose to glucose-6-phosphate. Unlike hexokinase I-III, glucokinase is not inhibited by its product (glucose-6-phosphate) and has a sigmoidal kinetics curve, meaning it is maximally responsive to changes around the physiological glucose range. This makes it the ideal glucose sensor.
-
The resulting ATP generated by glycolysis closes K_ATP channels → membrane depolarization → Ca²⁺ influx → insulin exocytosis.
-
Biochemistry, Lippincott Illustrated Reviews 8th ed, p. 295-296
-
Basic Medical Biochemistry - A Clinical Approach, 6th ed
2. The β Cell and Insulin Secretion - Biochemical Mechanism
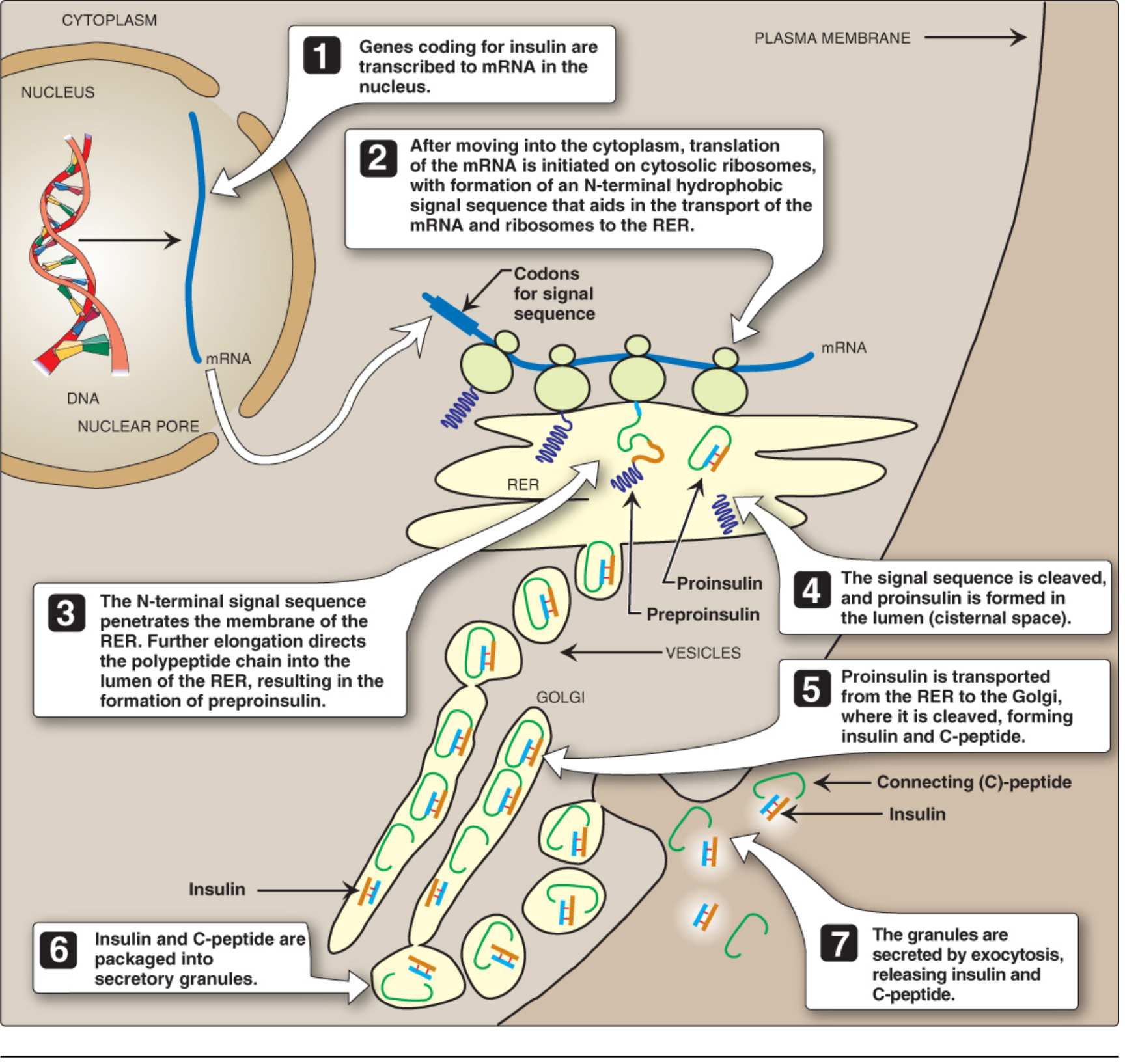
Intracellular movements of insulin and its precursors - Lippincott Biochemistry 8th ed
Synthesis: The insulin gene (chromosome 11) is transcribed to mRNA → translated as preproinsulin → signal sequence cleaved in RER → proinsulin → transported to Golgi → proteases cleave out C-peptide, yielding mature insulin (A + B chains linked by 2 disulfide bonds) + C-peptide. Both are co-secreted by exocytosis. C-peptide is used clinically to measure endogenous insulin production.
Post-meal glucose/insulin/glucagon dynamics:
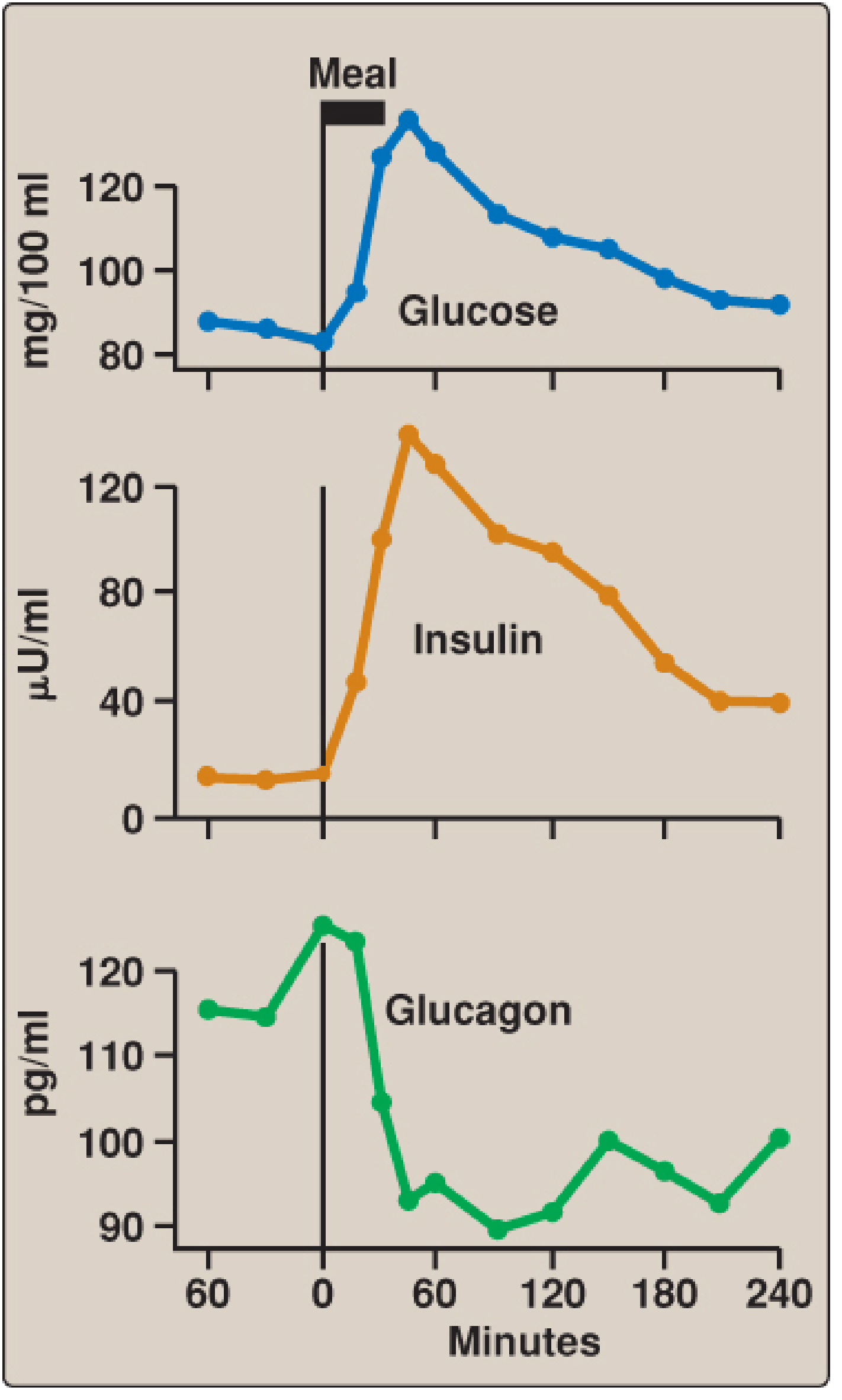
Post-meal hormone changes - Lippincott Biochemistry 8th ed
Note glucagon drops promptly after a carbohydrate meal (suppressed by rising glucose and GLP-1), then recovers as glucose normalizes.
3. Glycolysis - Biochemical Regulation
Glycolysis converts glucose to pyruvate, yielding a net 2 ATP. Three irreversible, regulated steps are the primary control points:
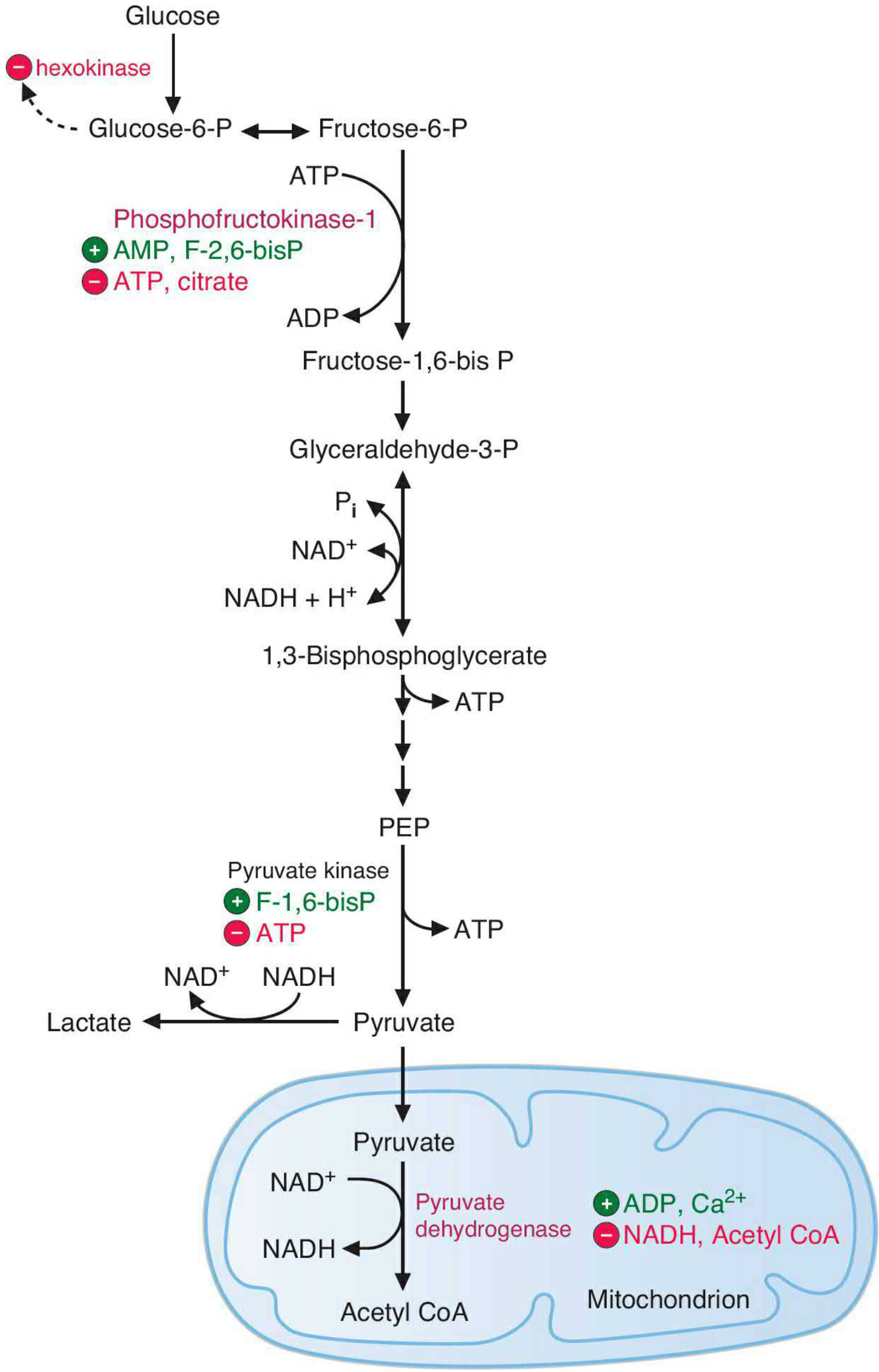
Major regulatory sites in the glycolytic pathway - Basic Medical Biochemistry 6th ed
Step 1: Hexokinase / Glucokinase (Glucose → Glucose-6-phosphate)
- Hexokinase (tissues): product-inhibited by glucose-6-P. Ensures glucose is only phosphorylated if the cell needs it.
- Glucokinase (liver, β cells): not inhibited by glucose-6-P; high Km means activity rises in proportion to blood glucose. Acts as a glucose "buffer" in the liver.
Step 2: Phosphofructokinase-1 (PFK-1) - the key rate-limiting step
PFK-1 catalyzes: Fructose-6-P + ATP → Fructose-1,6-bisphosphate + ADP
| Allosteric Activators | Allosteric Inhibitors |
|---|---|
| AMP (low energy signal) | ATP (product inhibition) |
| Fructose-2,6-bisphosphate (F-2,6-BP) | Citrate (signals TCA is replete) |
| ADP | H⁺ (acidosis) |
Step 3: Pyruvate Kinase (PEP → Pyruvate)
-
Activated by fructose-1,6-bisphosphate (feedforward activation)
-
Inhibited by ATP, alanine
-
Inhibited by cAMP-dependent phosphorylation (glucagon → PKA → PK inactivation in liver)
-
Basic Medical Biochemistry - A Clinical Approach, 6th ed, p. 809
-
Medical Physiology (Boron & Boulpaep)
4. The Master Switch: Fructose-2,6-Bisphosphate (F-2,6-BP)
F-2,6-BP is the most potent regulator of the glycolysis/gluconeogenesis balance in the liver. It is not a glycolytic intermediate - it is a regulatory molecule synthesized and degraded by a bifunctional enzyme: PFK-2/FBPase-2.
Actions:
- Activates PFK-1 (glycolysis) by relieving ATP inhibition and increasing affinity for fructose-6-P
- Inhibits fructose-1,6-bisphosphatase (gluconeogenesis) by increasing its Km for substrate
Hormonal control of F-2,6-BP concentration:
| Hormone | Signal | Effect on bifunctional enzyme | F-2,6-BP level | Result |
|---|---|---|---|---|
| Insulin (fed state) | ↑ glucose | Activates PFK-2 (kinase activity) | High | Glycolysis active, gluconeogenesis suppressed |
| Glucagon (fasting) | ↑ cAMP → PKA | Phosphorylates bifunctional enzyme → activates FBPase-2, inactivates PFK-2 | Low | Glycolysis inhibited, gluconeogenesis active |
This is the biochemical switch that toggles the liver between glucose-consuming (fed) and glucose-producing (fasting) states.
- Harper's Illustrated Biochemistry 32nd ed, p. 196
- Medical Physiology (Boron & Boulpaep)
5. Gluconeogenesis - Biochemical Regulation
Gluconeogenesis regenerates glucose from:
- Lactate (Cori cycle from anaerobic muscle)
- Alanine (glucose-alanine cycle from muscle)
- Glycerol (from adipose lipolysis)
- Oxaloacetate precursors (from TCA intermediates)
The pathway bypasses the three irreversible steps of glycolysis using four unique enzymes:
| Glycolytic enzyme (irreversible) | Gluconeogenic bypass enzyme | Activated by |
|---|---|---|
| Pyruvate kinase | Pyruvate carboxylase (Pyr → OAA) + PEPCK (OAA → PEP) | Pyruvate carboxylase activated by Acetyl-CoA; PEPCK induced by glucagon/cortisol |
| PFK-1 | Fructose-1,6-bisphosphatase (FBPase-1) | Activated when F-2,6-BP is low; inhibited by AMP |
| Hexokinase/Glucokinase | Glucose-6-phosphatase | Expressed only in liver and kidney; induced by glucagon/cortisol |
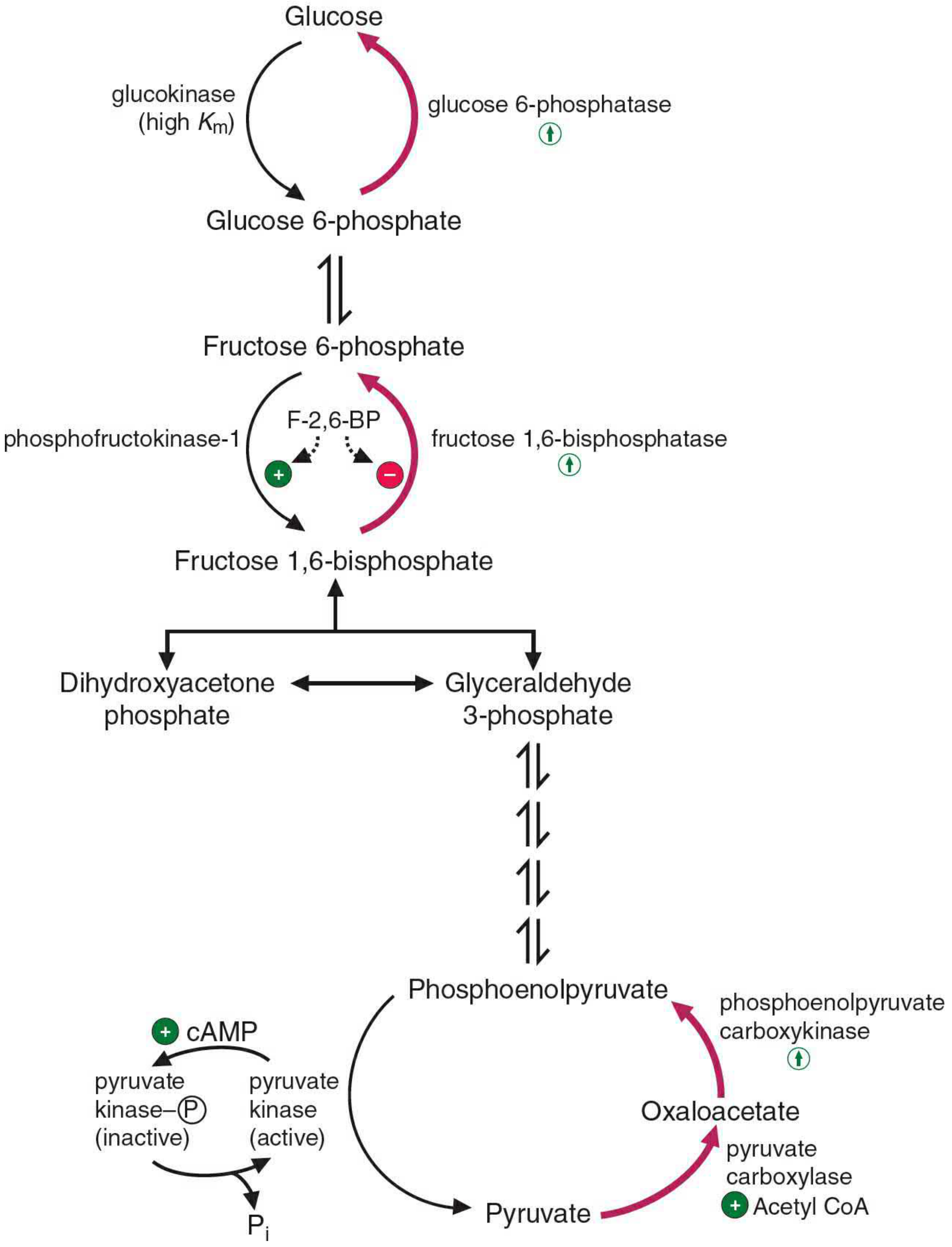
Regulation of gluconeogenesis (red) and glycolysis during fasting - Basic Medical Biochemistry 6th ed
Allosteric regulation summary:
- Acetyl-CoA activates pyruvate carboxylase - when fat is being oxidized (fasting), Acetyl-CoA signals that gluconeogenesis should proceed
- AMP inhibits FBPase-1 - when energy is low (AMP high), stop wasting ATP on futile gluconeogenesis
- Citrate activates FBPase-1 - signals TCA cycle intermediates are available for gluconeogenesis
- High ATP + alanine inhibit pyruvate kinase - prevent re-entry of gluconeogenic substrate into glycolysis
Transcriptional regulation (hours):
-
Glucagon → cAMP → PKA → CREB phosphorylation: CREB transcription factor directly induces PEPCK and G6Pase genes, and also induces PGC-1α (a transcriptional coactivator that amplifies gluconeogenic gene expression)
-
Glucagon suppresses FOXO1 phosphorylation (in contrast to insulin, which phosphorylates FOXO1, exporting it from the nucleus and silencing gluconeogenic genes)
-
Cortisol mobilizes amino acids from muscle proteins → provides gluconeogenic substrate; also induces PEPCK
-
Medical Physiology (Boron & Boulpaep), p. 946-949
-
Basic Medical Biochemistry - A Clinical Approach, 6th ed, p. 1270-1271
-
Guyton and Hall Textbook of Medical Physiology, p. 840
6. Glycogen Metabolism - Biochemical Regulation
Glycogen is the primary short-term glucose storage polymer, primarily in liver (glycogen maintains blood glucose) and muscle (for local use only).
Glycogenolysis (glycogen → glucose-1-P → glucose)
Activated by the glucagon/epinephrine → cAMP cascade:
- Glucagon or epinephrine binds → adenylate cyclase → ↑ cAMP
- cAMP → activates protein kinase A (PKA)
- PKA phosphorylates phosphorylase kinase → activates it
- Phosphorylase kinase phosphorylates glycogen phosphorylase b → glycogen phosphorylase a (active)
- Glycogen phosphorylase a cleaves glycogen to glucose-1-phosphate
- Glucose-1-P → glucose-6-P → (via glucose-6-phosphatase in liver) → free glucose released into blood
Simultaneously: PKA phosphorylates and inactivates glycogen synthase, preventing futile re-synthesis.
- Basic Medical Biochemistry - A Clinical Approach, 6th ed, p. 1270
Glycogenesis (glucose → glycogen)
Activated by insulin:
- Insulin → PI3K → Akt → inactivates glycogen synthase kinase-3 (GSK-3) → allows protein phosphatase to dephosphorylate and activate glycogen synthase
- Glucose-6-P also allosterically activates glycogen synthase (substrate availability signal)
Calcium (epinephrine/muscle contraction) also activates phosphorylase kinase via CaM (calmodulin) - this accounts for the rapid increase in muscle glycogenolysis during exercise independent of cAMP.
7. Levels of Metabolic Regulation - Summary
Regulation of blood glucose occurs across three timescales:
| Level | Timescale | Mechanism | Example |
|---|---|---|---|
| Allosteric | Milliseconds - seconds | Non-covalent binding of effector changes enzyme conformation | AMP activates PFK-1; ATP inhibits it |
| Covalent modification | Seconds - minutes | Phosphorylation/dephosphorylation by kinases and phosphatases | PKA phosphorylates glycogen phosphorylase kinase; insulin activates protein phosphatase |
| Transcriptional | Hours - days | Hormones induce/repress enzyme synthesis | Glucagon/cortisol induce PEPCK and G6Pase; insulin suppresses PEPCK via FOXO1 |
Key regulatory principles (Basic Medical Biochemistry 6th ed):
- Regulation occurs at the rate-limiting (slowest) step of a pathway
- Regulation occurs at the first committed step and at branch points
- Irreversible reactions are the regulatory control points - these also differ between synthetic and degradative pathways
- Many pathways use feedback inhibition (end product inhibits early enzyme)
- Compartmentation controls substrate access (e.g., glucose-6-phosphatase is ER-membrane bound; gluconeogenesis uses cytoplasm AND mitochondria)
- Hormones integrate multi-tissue responses via phosphorylation, enzyme induction/repression, or effector concentration changes
8. Fed vs. Fasting - The Biochemical Switch
| State | Insulin/Glucagon ratio | F-2,6-BP | cAMP | Active pathways | Suppressed pathways |
|---|---|---|---|---|---|
| Fed | High | High | Low | Glycolysis, glycogenesis, lipogenesis | Gluconeogenesis, glycogenolysis, lipolysis |
| Fasting | Low | Low | High | Gluconeogenesis, glycogenolysis, lipolysis, ketogenesis | Glycolysis, glycogenesis, lipogenesis |
The insulin/glucagon molar ratio (not absolute levels) is the biochemical signal that the liver reads to decide which metabolic mode to adopt. In the fed state this ratio is ~30:1; in fasting it falls to ~2:1 or lower.
- Medical Physiology (Boron & Boulpaep), p. 936-949
- Harper's Illustrated Biochemistry 32nd ed, p. 196-197
- Lippincott Biochemistry 8th ed, p. 866-867
This is a shared conversation. Sign in to Orris to start your own chat.