Write a short notes on hypoxia easy word
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Now I have enough rich content from authoritative textbooks. Here is a clear, easy-to-read short note on hypoxia:
Short Notes on Hypoxia
What is Hypoxia?
Hypoxia means reduced oxygen delivery to the tissues. The body's cells need a steady supply of oxygen to produce energy. When that supply falls short, cells start to malfunction - and if severe or prolonged, they begin to die.
Simply put: not enough oxygen reaches where it is needed.
How Does Oxygen Normally Reach the Tissues?
Oxygen is carried from the lungs to the tissues by two forces working together:
- Cardiac output - how much blood the heart pumps per minute.
- Oxygen content of blood - mainly how much oxygen is bound to hemoglobin (the protein in red blood cells that carries O2).
If either one drops significantly, hypoxia results.
Types of Hypoxia
There are four main types:
| Type | Simple Meaning | Common Causes |
|---|---|---|
| Hypoxic Hypoxia | Not enough O2 entering the blood | High altitude, lung disease, hypoventilation |
| Anemic Hypoxia | Blood can't carry enough O2 | Anemia, carbon monoxide (CO) poisoning |
| Ischemic (Circulatory) Hypoxia | Blood flow to tissues is too low | Heart failure, shock, arterial blockage |
| Histotoxic Hypoxia | Cells can't use O2 even when available | Cyanide poisoning |
A quick note on each:
- Hypoxic hypoxia - the arterial PO2 (oxygen pressure in blood) is actually low. The lungs are not getting enough oxygen in, or cannot transfer it properly into the blood. This is the most common type.
- Anemic hypoxia - PO2 in the blood is normal, but there is not enough hemoglobin to carry sufficient oxygen. In CO poisoning, hemoglobin is "hijacked" by carbon monoxide and cannot bind oxygen.
- Ischemic hypoxia - oxygen content of blood may be fine, but poor blood flow means tissues never receive it. This is the most dangerous for the brain.
- Histotoxic hypoxia - oxygen is delivered normally, but the cell's machinery (mitochondria) is blocked and cannot use it. Cyanide is the classic example.
Signs and Symptoms
When the brain is deprived of oxygen, symptoms appear quickly:
- Mild: Headache, dizziness, confusion, poor concentration
- Moderate: Drowsiness, visual changes, rapid breathing, rapid heart rate
- Severe: Loss of consciousness, seizures, coma
The skin may appear bluish - this is called cyanosis, and it happens when more than 5 g/dL of deoxygenated hemoglobin is present in the blood. (Note: anemic patients may not show cyanosis even when severely hypoxic, simply because there is not enough hemoglobin to turn blue.)
Compensation - How the Body Fights Back
The body has automatic responses to hypoxia:
- Increased breathing rate - to pull in more oxygen
- Increased heart rate - to pump blood faster
- Cerebral vasodilation - brain blood vessels widen to increase flow (can roughly double)
- Increased red blood cell production - in chronic hypoxia (e.g., living at high altitude)
These compensations work well for mild or moderate hypoxia, but fail when the lack of oxygen is severe.
Oxygen Therapy - Does It Help?
The value of giving extra oxygen depends on the type:
- Hypoxic hypoxia - Excellent response. Extra O2 corrects the low alveolar oxygen directly.
- Diffusion/hypoventilation hypoxia - Very helpful. O2 therapy can raise the driving pressure for O2 to cross into the blood by over 800%.
- Anemic/circulatory hypoxia - Limited help. The problem is in transport, not in alveolar O2 levels. A small extra amount dissolves in plasma and can still be life-saving.
- Histotoxic hypoxia (cyanide) - No benefit. The cells cannot use oxygen regardless of how much is delivered.
Key Differences: Hypoxia vs. Hypoxemia
| Term | Meaning |
|---|---|
| Hypoxemia | Low oxygen in the blood (low PaO2) |
| Hypoxia | Low oxygen in the tissues |
Hypoxemia often causes hypoxia, but not always. For example, in CO poisoning, PaO2 is normal but oxygen content is low - so you can have hypoxia without hypoxemia.
Summary
- Hypoxia = tissues not getting enough oxygen
- Four types: hypoxic, anemic, ischemic, histotoxic
- Brain is the most sensitive organ - symptoms appear within seconds to minutes
- Oxygen therapy is most effective in hypoxic/diffusion hypoxia, less so in circulatory/anemic, and useless in histotoxic
- Always identify the type before treating
Sources: Costanzo Physiology 7th Edition, p. 247 | Guyton and Hall Textbook of Medical Physiology | Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 377
Synapse short notes in simple. Words
Finding Sources
Reading File
Reading File
Reading File
I have rich content from Neuroscience (Exploring the Brain), Guyton & Hall, and Katzung's Pharmacology. Let me now compile a clear, simple short note.
Short Notes on Synapse
What is a Synapse?
A synapse is the tiny junction (connection point) between two nerve cells (neurons) where information is passed from one to the other.
Think of it like a bridge - one neuron sends a message, and the synapse carries it across to the next neuron.
The word synapse comes from Greek, meaning "to clasp together."
Parts of a Synapse
A synapse has three basic parts:
| Part | What It Is | Simple Meaning |
|---|---|---|
| Presynaptic terminal | The end of the sending neuron (axon terminal) | The "sender" side |
| Synaptic cleft | The tiny gap between the two neurons | The "bridge" / gap |
| Postsynaptic membrane | The surface of the receiving neuron (usually a dendrite or cell body) | The "receiver" side |
The synaptic cleft is extremely narrow - just about 20-40 nanometres wide (much thinner than a human hair).
How Does a Synapse Work?
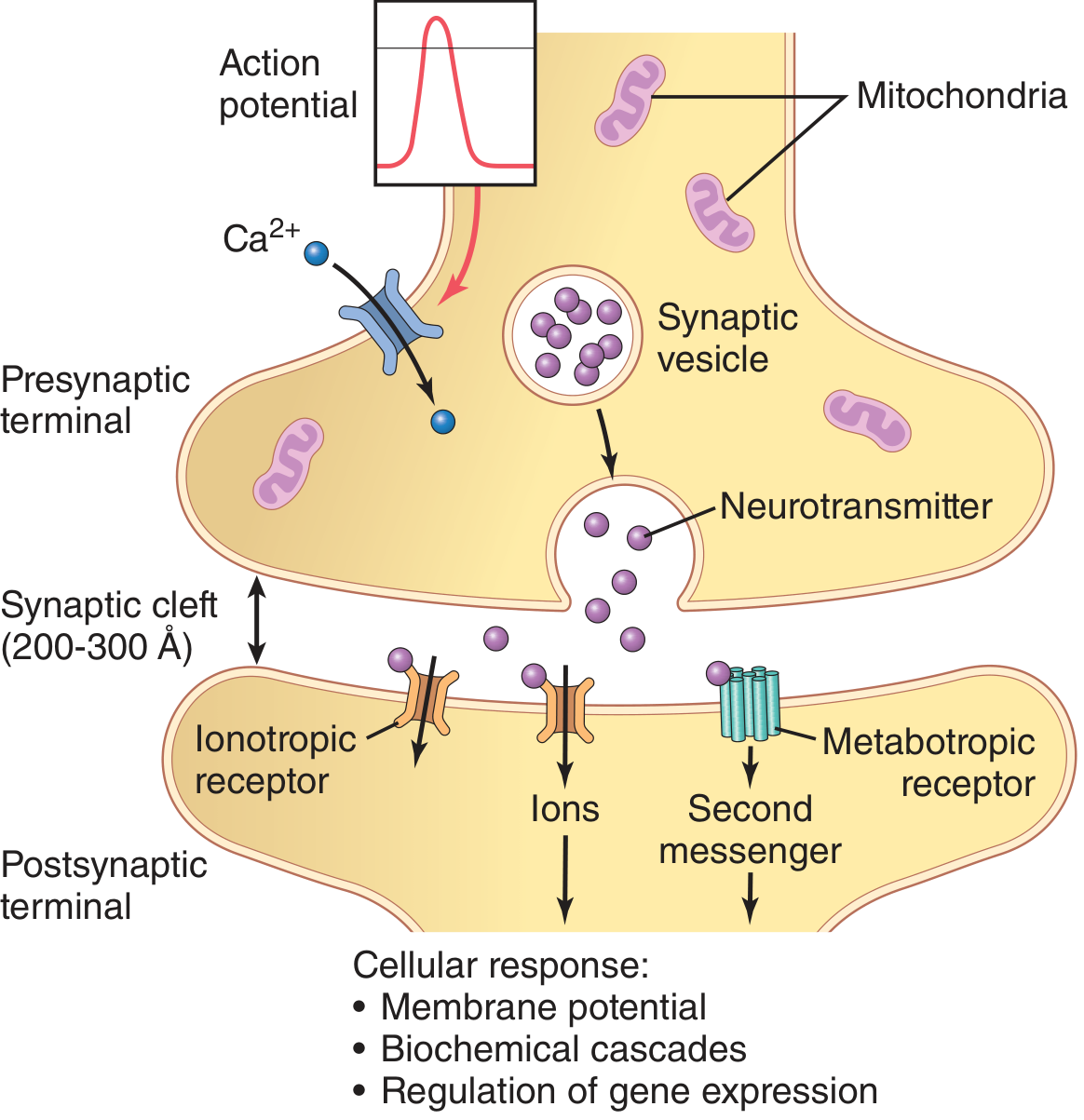
The process of passing information across a synapse is called synaptic transmission. Here is how it happens, step by step:
- Electrical signal arrives - An action potential (nerve impulse) travels down the axon and reaches the presynaptic terminal.
- Calcium enters - The arriving signal opens special calcium channels. Calcium flows into the terminal.
- Neurotransmitter released - Calcium causes tiny packages called synaptic vesicles (which hold chemical messengers) to fuse with the membrane and release their contents into the synaptic cleft.
- Chemical crosses the gap - The chemical messenger, called a neurotransmitter, drifts across the cleft.
- Receiver responds - The neurotransmitter binds to receptors on the postsynaptic membrane, which triggers a new electrical signal in the next neuron.
So the signal goes: Electrical → Chemical → Electrical
This whole process takes only about 0.5 milliseconds (half a thousandth of a second).
Types of Synapses
1. Chemical Synapse (Most Common)
- Uses a chemical (neurotransmitter) to carry the signal across the gap
- Transmission is one-way only - from pre to post
- Slower but more flexible and controllable
- Examples: synapses using acetylcholine, dopamine, serotonin, GABA
2. Electrical Synapse (Less Common)
- The two neurons are physically connected by gap junction channels
- Electrical current flows directly from one neuron to the next
- Transmission can go both ways
- Much faster than chemical synapses
- Helps groups of neurons fire at the same time (synchronization)
- Found in the hypothalamus and some areas needing very fast, coordinated responses
Types of Signals at Chemical Synapses
When a neurotransmitter acts on the postsynaptic cell, it produces one of two effects:
| Effect | Name | What Happens |
|---|---|---|
| Excitatory | EPSP (Excitatory Postsynaptic Potential) | The next neuron is pushed closer to firing - it becomes more likely to send a signal |
| Inhibitory | IPSP (Inhibitory Postsynaptic Potential) | The next neuron is pushed away from firing - it becomes less likely to send a signal |
A neuron receives thousands of inputs at once, some excitatory and some inhibitory. It adds them all up - if the total excitation exceeds a threshold, it fires. This is called summation.
Key Features of Synaptic Transmission
- One-way flow (chemical synapses) - signals only go pre → post, not backward. This allows precise, directed communication.
- Delay - There is a tiny delay (~0.5 ms) at each synapse. Long pathways with many synapses have more total delay.
- Modulation - Synaptic strength can increase or decrease based on use, learning, or drugs. This is the basis of memory and learning.
- Drug target - Most psychoactive drugs (antidepressants, anaesthetics, painkillers) and many toxins act by interfering with synaptic transmission.
Common Neurotransmitters
| Neurotransmitter | Main Action |
|---|---|
| Acetylcholine | Excites muscles; key in memory |
| Dopamine | Reward, movement, mood |
| Serotonin | Mood, sleep, appetite |
| GABA | Main inhibitory transmitter in the brain |
| Glutamate | Main excitatory transmitter in the brain |
| Norepinephrine | Alertness, arousal |
Why Are Synapses Important?
- Every thought, movement, feeling, and memory depends on synaptic transmission
- Diseases like Alzheimer's, Parkinson's, depression, epilepsy, and schizophrenia all involve synaptic dysfunction
- Most CNS drugs work by modifying what happens at synapses - blocking receptors, preventing neurotransmitter breakdown, or affecting vesicle release
Summary in One Paragraph
A synapse is the junction between two neurons. The sending neuron releases a chemical (neurotransmitter) into the tiny gap (synaptic cleft), which binds to the receiving neuron and either excites or inhibits it. Chemical synapses are one-way and slow but very precise. Electrical synapses are bidirectional and fast. The synapse is where the brain does its computing - and where most neurological drugs act.
Sources: Neuroscience - Exploring the Brain 5th Ed. | Guyton and Hall Textbook of Medical Physiology | Katzung's Basic and Clinical Pharmacology 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.