Carotid sinus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have a comprehensive set of information. Let me compile the full answer:
Carotid Sinus
Anatomy
The carotid sinus is a localized dilation (widening) of the internal carotid artery, situated just above the bifurcation of the common carotid artery at the level of the superior margin of the thyroid cartilage. It lies within the carotid sheath (which also encloses the internal jugular vein laterally and the vagus nerve posteriorly), deep to the anterior border of the sternocleidomastoid muscle. The carotid body - a chemoreceptor - sits at the bifurcation itself, distinct from the sinus.
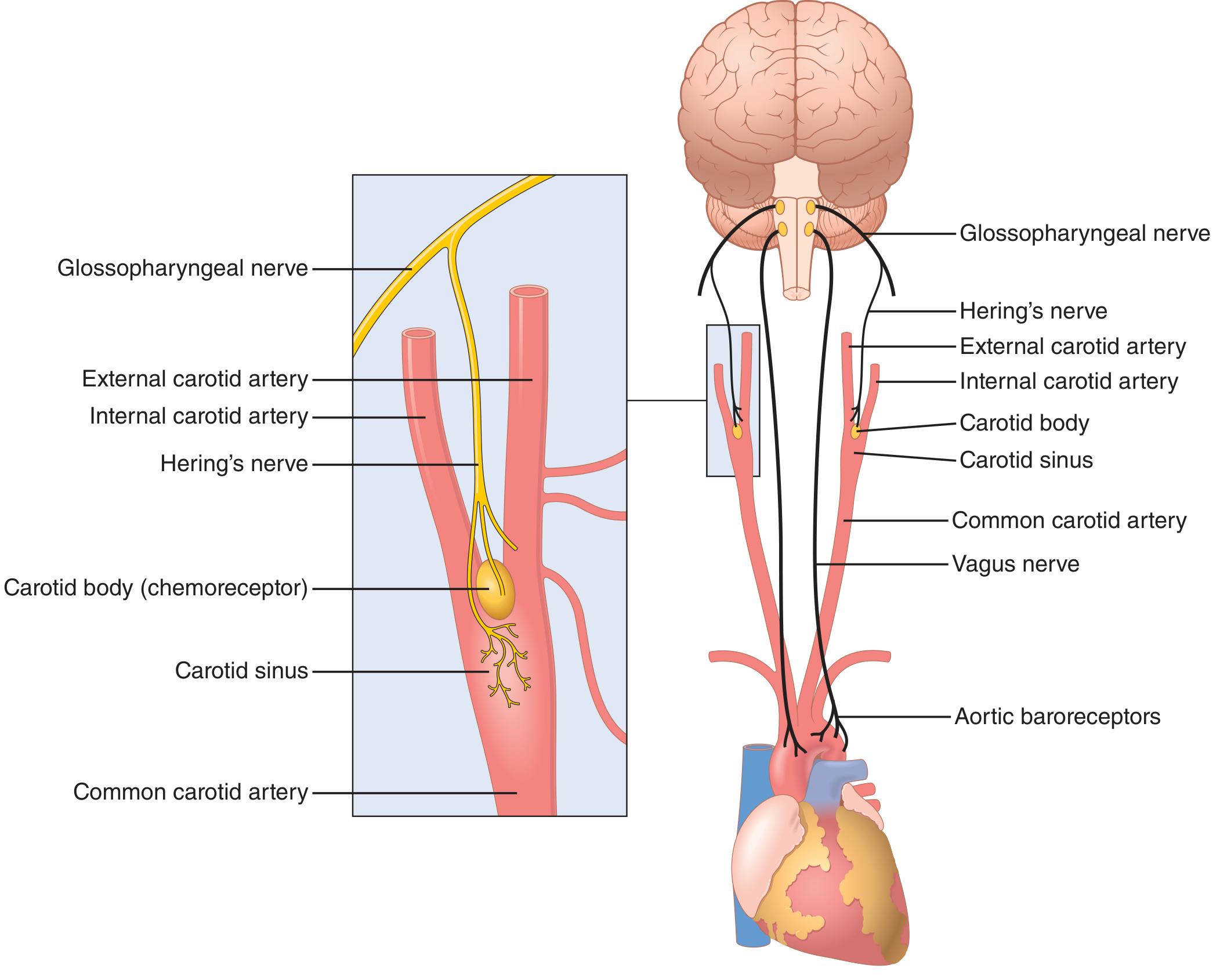
Figure 18.5 - Baroreceptor system for controlling arterial pressure. Guyton and Hall Textbook of Medical Physiology
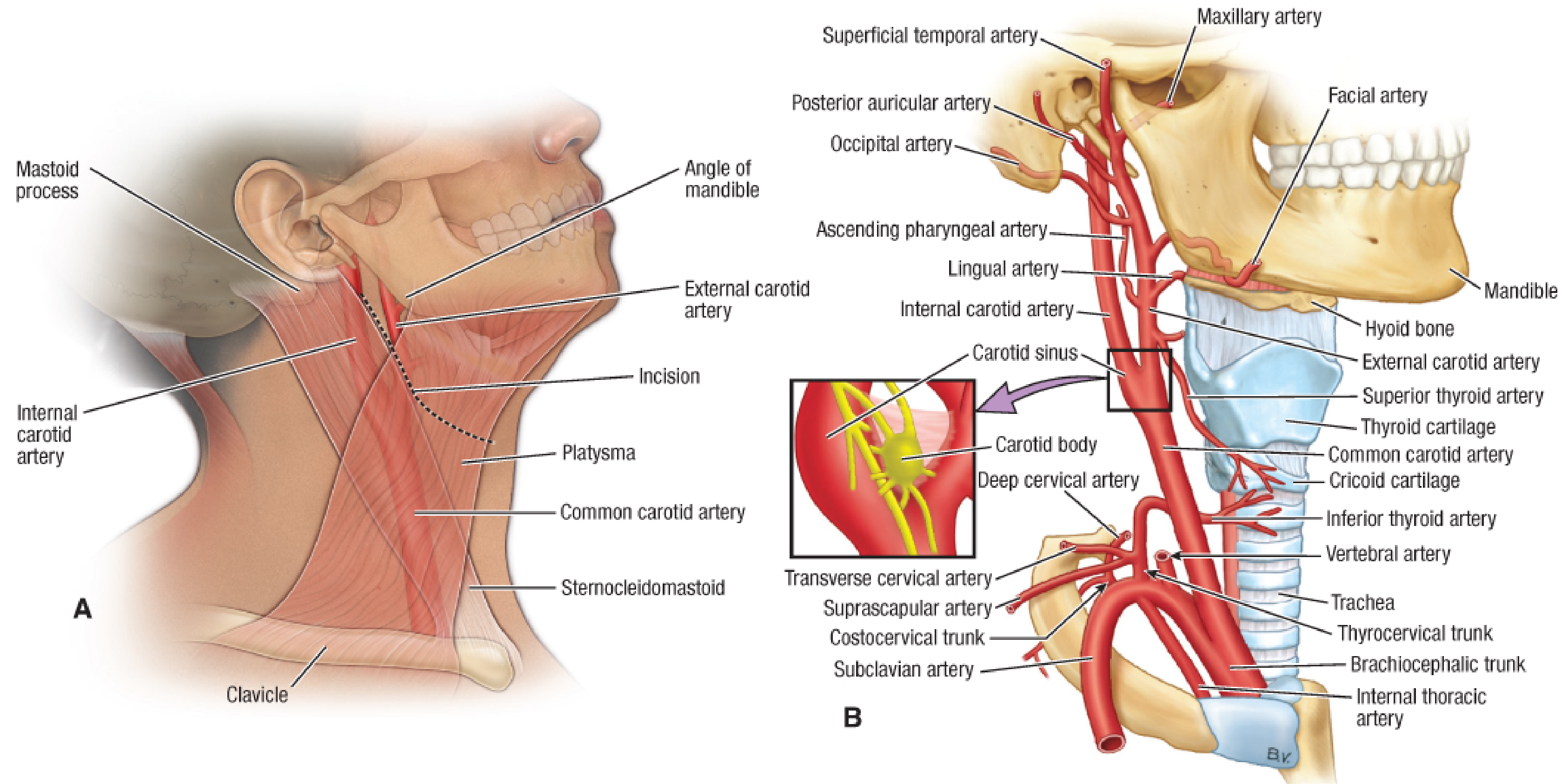
Figure 231.1 - Carotid arteries: regional anatomy and overview. Fischer's Mastery of Surgery, 8th ed.
Physiology: Baroreceptor Function
The carotid sinus wall contains baroreceptors - spray-type mechanoreceptive nerve endings that fire in response to stretch of the arterial wall, which directly reflects arterial pressure.
Firing characteristics (Guyton & Hall):
- No firing below ~50-60 mmHg
- Firing rate rises progressively up to ~180 mmHg (sigmoid curve)
- The normal operating range (~100 mmHg) is where the reflex is most sensitive - even small pressure changes evoke strong baroreceptor responses
- Dynamic response: fires more rapidly during a rapidly rising pressure than at the same static pressure; encodes pulse pressure information
- Different units begin firing at different pressures, allowing graded recruitment up to saturation at ~200 mmHg
- The carotid sinus has a lower threshold (~50 mmHg static) than the aortic arch (~110 mmHg), and changes in carotid sinus pressure exert a greater effect on systemic arterial pressure
Afferent pathway:
Signals travel via Hering's nerve (a branch of the glossopharyngeal nerve, CN IX) to the nucleus tractus solitarius (NTS) in the medulla. Aortic arch baroreceptors send signals via the vagus nerve (CN X) to the same nucleus.
Reflex arc (response to HIGH pressure):
- Increased stretch → increased baroreceptor firing
- NTS activates cardiovagal efferents (parasympathetic) → increased parasympathetic output to heart → bradycardia, reduced cardiac output
- NTS simultaneously inhibits the intermediolateral cell column → decreased sympathetic outflow to heart and peripheral vasculature → vasodilation, reduced SVR
- Net result: blood pressure falls back toward normal
Reflex arc (response to LOW pressure):
The reverse: reduced baroreceptor firing → inhibition of parasympathetic output, activation of sympathetic division → increased HR, contractility, vasoconstriction → blood pressure rises.
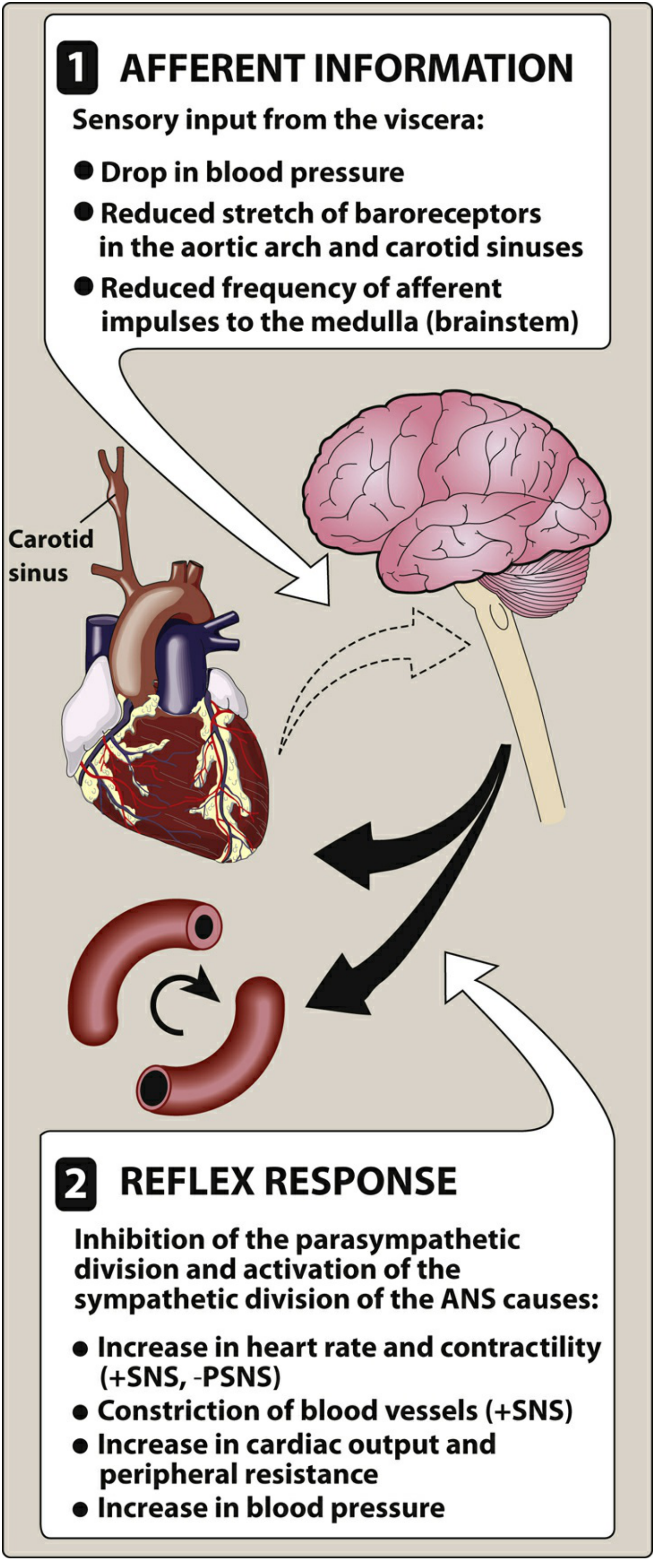
Figure 3.6 - Baroreceptor reflex arc. Lippincott Illustrated Reviews: Pharmacology
Carotid sinus vs. aortic arch:
| Feature | Carotid Sinus | Aortic Arch |
|---|---|---|
| Afferent nerve | Hering's nerve → CN IX | CN X (vagus) |
| Static threshold | ~50 mmHg | ~110 mmHg |
| Dynamic threshold | Lower | Higher |
| Effect on systemic BP | Greater | Less |
Carotid Sinus Hypersensitivity (CSH)
Definition: An exaggerated baroreceptor response to carotid sinus stimulation, diagnosed by:
- Asystole >3 seconds (cardioinhibitory type), or
- Systolic BP drop >50 mmHg without significant bradycardia (vasodepressor type), or
- Both (mixed type)
...during carotid sinus massage (CSM) that reproduces clinical syncope.
Epidemiology: Detected in approximately one-third of older adults evaluated for syncope or falls. Present in ~35-100 per million per year. Importantly, it can also be found in asymptomatic older individuals, so it must be interpreted in clinical context. More common in older men.
Triggers (clinical history may reveal):
- Wearing a tight collar
- Turning the head
- Shaving
- Swallowing
- Head rotation, neck tumors
Carotid Sinus Syndrome (CSS)
CSS = symptomatic carotid sinus hypersensitivity. Defined as recurrent syncope caused by spontaneous carotid sinus stimulation (not just a positive test).
- ~25% of patients with CSH have true CSS with spontaneous symptoms
- Consider in older patients with recurrent syncope and negative cardiac workup
Weiss-Baker syndrome refers to a rare variant with neurological symptoms (headache, dizziness, vertigo, hemiplegia, hemianopsia) without measurable BP or HR changes - likely reflects a migrainous or ischemic mechanism.
Carotid Sinus Massage (CSM): Procedure
Indications: Diagnosis of carotid sinus hypersensitivity; vagal termination of SVT (AVNRT, AVRT).
Technique:
- Place patient on cardiac monitor; start IV; have defibrillator and antiarrhythmics ready
- Auscultate for carotid bruits on both sides - bruit is a contraindication
- Head tilted backward, slightly to the opposite side
- Palpate carotid pulse just below the angle of the mandible, at the upper level of the thyroid cartilage, anterior to the SCM
- Apply fingertip pressure posteromedially toward the vertebral column for 5 seconds
- If no response, repeat after 1 minute; may try the opposite side
- Can combine with Valsalva maneuver for enhanced vagal effect
Normal response: Pause <3 seconds
Diagnostic: Asystole >3 seconds or >50 mmHg systolic drop
Contraindications:
- Carotid bruit
- Recent TIA or stroke
- Prior carotid surgery
- Active atherosclerotic disease (risk of plaque embolism)
Complications:
- Stroke (dislodgement of atherosclerotic plaque/thrombus) - the most feared complication; Bradley & Daroff recommend carotid ultrasound before CSM in patients >age [threshold not specified in text, implied older adults]
- Asystole, VT, or VF (especially in patients on digoxin - associated with more prolonged AV block)
- Normal pause <3 sec is physiological; longer pause may indicate CSS
Management
Cardioinhibitory or mixed CSH/CSS:
- Dual-chamber pacemaker implantation is recommended (Class IIA, LOE B-R - Braunwald's) for recurrent syncope or falls
- CSS with asystole >3 sec is a Class I pacemaker indication; without clear provocative events, it is Class IIA
Vasodepressor type:
- No proven pharmacologic therapy; some benefit with fludrocortisone, midodrine, or compression stockings (for orthostatic component)
- Surgical denervation of the carotid sinus in refractory cases (some patients)
SVT termination via CSM:
- Effective for AVNRT and AVRT (slows or blocks the AV node)
- Can combine with Valsalva maneuver for additive effect
- If unsuccessful, adenosine, verapamil, or beta-blockers can be used as alternatives
Sources: Guyton and Hall Textbook of Medical Physiology; Braunwald's Heart Disease, 12th ed.; Goldman-Cecil Medicine; Bradley and Daroff's Neurology in Clinical Practice; Fischer's Mastery of Surgery, 8th ed.; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Lippincott Illustrated Reviews: Pharmacology; Harrison's Principles of Internal Medicine 22E (2025); Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.