CVST work up
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive CVST workup based on authoritative textbook sources:
Cerebral Venous Sinus Thrombosis (CVST) — Workup
When to Suspect CVST
Consider CVST in any patient with:
- New headache (progressive over days–weeks, or thunderclap) — especially without a clear etiology
- Signs of elevated ICP: papilledema, nausea/vomiting
- Seizures (present in ~40%)
- Focal neurologic deficits not following an arterial territory
- Altered mental status or coma (14%)
- Unexplained stroke symptoms in a young female under 50
- Elevated LP opening pressure without another explanation
High-risk presentations: female gender, peripartum state, OCP use, recent head/neck surgery, hypercoagulable state.
— Rosen's Emergency Medicine, p. Cerebral Venous Thrombosis section; Tintinalli's Emergency Medicine, p. 1293
Risk Factors to Elicit on History
| Category | Examples |
|---|---|
| Hormonal | OCP, HRT, pregnancy/peripartum |
| Thrombophilia | Factor V Leiden, protein C/S deficiency, antithrombin III deficiency, lupus anticoagulant |
| Infection/local | Sinusitis, otitis media, mastoiditis, oropharyngeal infection |
| Systemic disease | SLE, IBD, malignancy, nephrotic syndrome, sickle cell disease |
| Drugs | Asparaginase, estrogen, cocaine |
| Other | Dehydration, trauma, recent surgery |
— Harriet Lane Handbook, p. 726; Grainger & Allison's Diagnostic Radiology, p. 1453–1454
Laboratory Workup
Send on all suspected CVST:
| Test | Purpose |
|---|---|
| CBC | Polycythemia, thrombocytosis, hematologic disorder |
| PT/INR, PTT | Coagulopathy baseline; guides anticoagulation |
| BMP/Electrolytes, BUN, Cr | Metabolic contributors, dehydration |
| ESR, CRP | Inflammatory/infectious cause |
| D-dimer | A normal D-dimer can exclude CVT in low-risk patients (no thromboembolic risk factors, normal neuro exam, no papilledema) |
| Pregnancy test | Women of childbearing age |
| Antithrombin III activity | Thrombophilia |
Thrombophilia screen (ideally after acute anticoagulation phase or before starting):
- Protein C and S activity
- Antithrombin III
- Factor V Leiden (PCR)
- Prothrombin gene mutation (G20210A)
- Lupus anticoagulant / antiphospholipid antibodies
- JAK2 mutation (if polycythemia/essential thrombocythemia suspected)
Note: thrombophilia screening in the acute phase or while on anticoagulation may yield false results; can be deferred but should still be ordered.
— Rosen's Emergency Medicine, p. Diagnostic Testing; Harriet Lane Handbook, p. 726
Imaging Workup
Step 1 — Non-contrast CT Head (initial screen)
- Often normal or non-specific — insensitive alone
- May show:
- Hyperdense sinus/vein (hyperdense cord sign for cortical vein, dense triangle sign for SSS)
- Infarct, hemorrhage, or edema — often not conforming to an arterial territory
- Parasagittal hemorrhagic infarcts (superior sagittal sinus thrombosis)
- Does NOT rule out CVST
Step 2 — MRI Brain + MR Venography (MRV) ← Gold Standard
- MRI: loss of normal flow void in the sinus; T1/T2 hyperintensity in thrombosed vessel; parenchymal edema, hemorrhagic infarct
- MRV: loss of flow signal / nonvisualization of sinus
- SWI/GRE: "blooming" hypointensity in thrombosed sinus; prominent engorged draining veins (venous congestion pattern)
- DWI + FLAIR also recommended to characterize parenchymal injury
- MRI/MRV is the test of choice when available
Step 3 — CT Venography (CTV) — Alternative if MRI contraindicated
- At least as sensitive as MRV for major dural sinus thrombosis
- Shows "delta sign" (hypodense thrombus + peripheral rim enhancement) on contrast CT
- Faster; less susceptible to motion artifact
Step 4 — Digital Subtraction Angiography (DSA)
- Now rarely required for diagnosis
- Reserved for: equivocal MRI/MRV/CTV, prelude to endovascular therapy if deteriorating despite anticoagulation
Parenchymal lesion patterns by sinus involved:
| Sinus Thrombosed | Parenchymal Lesion Location |
|---|---|
| Superior sagittal sinus | Bilateral parasagittal cortical/subcortical (often asymmetric) |
| Internal cerebral veins / straight sinus | Bilateral thalami ± basal ganglia |
| Vein of Labbé / lateral sinus | Posterolateral temporal lobe, inferior parietal |
— Grainger & Allison's Diagnostic Radiology, p. 1453–1454; Rosen's Emergency Medicine, p. Diagnostic Testing; Bradley & Daroff's Neurology, p. MRV section
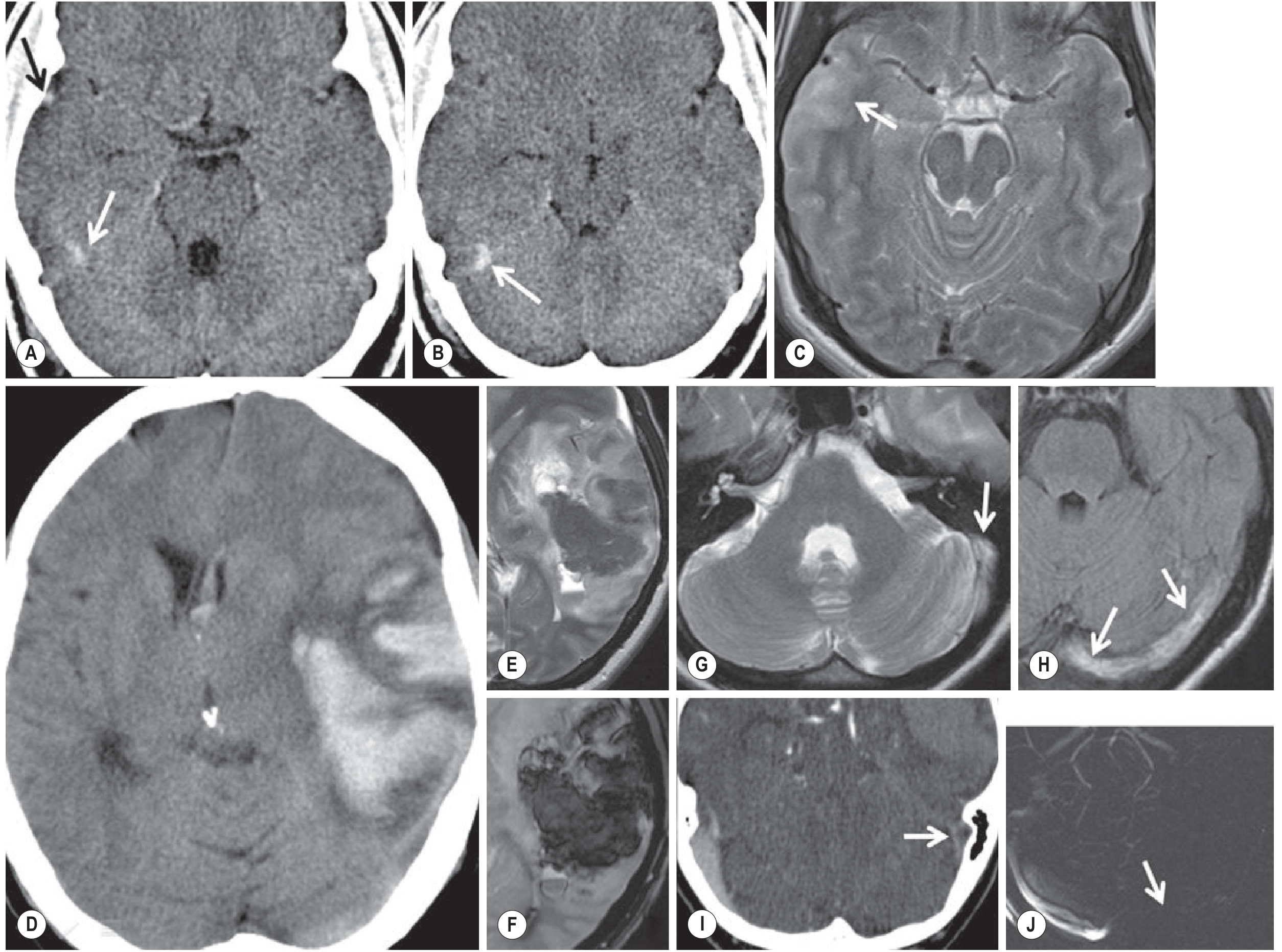
Fig. 56.28 — Cerebral Venous Thrombosis. CT (A, B, D) and MRI (C, E–J) demonstrating hemorrhagic infarcts, venous congestion, and parenchymal edema/signal abnormalities from Grainger & Allison's Diagnostic Radiology.
Lumbar Puncture
- Can be performed safely in CVST (no contraindication)
- Elevated opening pressure in the setting of a new headache type should raise suspicion and prompt MRV
- CSF may show elevated RBCs or protein; results are non-specific
- Useful if infection (meningitis) is in the differential
Workup Summary (Quick Reference)
Suspected CVST
│
├── Labs: CBC, BMP, PT/PTT, ESR, CRP, D-dimer, pregnancy test
│ Thrombophilia panel (antithrombin III, protein C/S,
│ factor V Leiden, prothrombin mutation, lupus anticoag)
│
├── Imaging:
│ 1. Non-contrast CT head (initial; can miss CVST)
│ 2. MRI brain + MRV ← Gold standard
│ (DWI, FLAIR, SWI/GRE, T1, T2)
│ OR CTV if MRI contraindicated
│ 3. DSA if equivocal or endovascular planned
│
└── LP if opening pressure elevated or infection suspected
Differential Diagnosis
- Idiopathic intracranial hypertension (IIH) — early CVST mimics IIH
- Brain tumor
- Ischemic or hemorrhagic arterial stroke
- Meningitis / encephalitis / brain abscess
- SAH (thunderclap presentation)
- PRES, RCVS
- SLE, sarcoidosis
— Rosen's Emergency Medicine, p. Differential Diagnoses
Initial Management (ED)
- Anticoagulation — LMWH preferred over UFH (weak recommendation); start regardless of intracranial hemorrhage
- Antiepileptics (levetiracetam or phenytoin) if seizures
- Admission to stroke unit
- Thrombectomy/thrombolysis in refractory, deteriorating cases at expert centers
This is a shared conversation. Sign in to Orris to start your own chat.