Define semiformal ' discuss it's ethology, clinical features, investigation and treatment
Reading File
Asking for Preferences
Could you please type the correct medical term you meant? For example, was it:
- Scarlet fever
- Scrofuloderma
- Seminal vesiculitis
- Sarcoidosis
- Something else entirely?
Please share the correct spelling or describe the condition briefly and I'll give you a full breakdown right away.
Define seminoma , discuss its ethiology ' clinical features, investment gabion and treatment
Finding Sources
Finding Sources
Searching PubMed
seminoma testicular germ cell tumor
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive, authoritative information from multiple textbooks plus excellent images. Here is the full answer:
Seminoma
Definition
A seminoma is a malignant germ cell tumor (GCT) arising from the germinal epithelium of the testis. It is the most common testicular GCT, accounting for approximately 50% of all germ cell tumors. It is highly radiosensitive, chemosensitive, and carries an excellent prognosis, especially when detected early. - Bailey and Love's Short Practice of Surgery 28th Ed.
Etiology / Risk Factors
The exact cause is unknown, but both congenital and acquired factors are implicated. - Smith and Tanagho's General Urology, 19th Ed.
1. Germ Cell Neoplasia In Situ (GCNIS)
- Formerly called Intratubular Germ Cell Neoplasia (ITGCN), this is the most important precursor lesion
- Consists of undifferentiated germ cells located basally within seminiferous tubules that morphologically resemble seminoma cells
- Approximately 50% of men with GCNIS will develop a germ cell tumor within 5 years
- Seminoma is thought to arise directly from GCNIS, which also acts as the common precursor for non-seminomatous subtypes - Campbell Walsh Wein Urology
2. Cryptorchidism (Undescended Testis)
- The strongest known risk factor - approximately 7-10% of testicular tumors develop in patients with a history of cryptorchidism
- Seminoma is the most common tumor type arising in cryptorchid testes
- Risk is highest for the intra-abdominal testis (1 in 20) and lower for the inguinal testis (1 in 80)
- Even the contralateral normally descended testis carries a 5-10% risk
- Orchiopexy performed before age 13 significantly lowers the malignancy risk
3. Demographic and Genetic Factors
- Predominantly affects Caucasian males; incidence in African-Americans is ~one-quarter that of Caucasians
- Slightly more common on the right side (paralleling the increased right-sided cryptorchidism rate)
- Higher incidence in Scandinavian countries; lower in Japan
- Higher socioeconomic class doubles the risk compared to lower classes
4. Maternal Estrogen Exposure
- Exogenous estrogen given to the mother during pregnancy is associated with a relative risk of 2.8 to 5.3 for testicular tumors in the fetus
5. Other Factors
- Trauma and infection-related testicular atrophy have been associated, though a causal relationship has not been established
- Bilateral tumors occur in 1-2% of cases; ~50% of these men have a history of cryptorchidism
Histological Subtypes and Pathology
Three histologic subtypes are recognized (though subtype has no prognostic significance stage for stage):
| Subtype | Frequency | Key Features | Peak Age |
|---|---|---|---|
| Classic seminoma | 85% | Coalescing gray nodules; sheets of large cells with clear cytoplasm and densely staining nuclei; fibrovascular septae with lymphocytes | 4th decade |
| Anaplastic seminoma | 5-10% | ≥3 mitoses per high-power field; higher nuclear pleomorphism; tends to present at higher stage | Earlier than classic |
| Spermatocytic tumor | ~1% | Cells vary in size; densely staining cytoplasm; renamed "spermatocytic tumor" in 2016 WHO classification; NOT associated with cryptorchidism or GCNIS; essentially benign | >50 years |
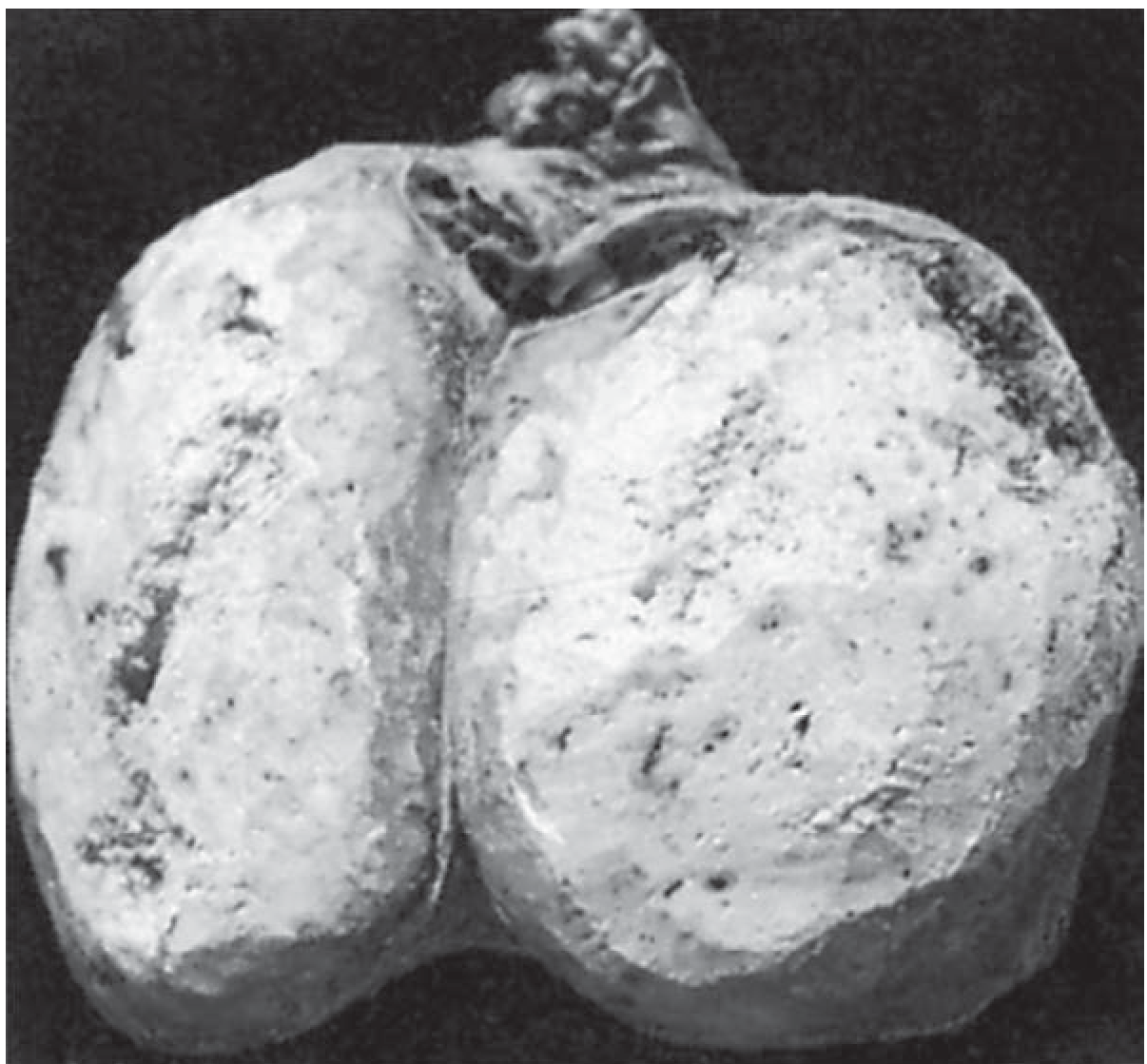
Gross appearance: Soft, tan-to-white diffuse or multinodular mass with homogeneous pinkish-cream cut surface. - Bailey and Love's
Microscopy: Monotonous sheets of large polygonal cells with clear cytoplasm and prominent acidophilic nucleoli. Cells are divided into nests by fibrovascular septae containing lymphocytes. Active lymphocytic infiltration suggests a good host immune response. Syncytiotrophoblastic elements (hCG-positive) are seen in ~15% of cases.
Immunohistochemistry: Seminomas are:
- Positive: CD117, PLAP (placental alkaline phosphatase), OCT3/4
- Negative: CD30, AFP
Clinical Features
Typical Presentation
- Age: Most commonly the 4th or 5th decade (older than NSGCTs). Rare in childhood and patients over 70.
- Painless testicular swelling - the classic and most common presentation
- A firm, non-tender scrotal mass that does not transilluminate
- Sensation of heaviness or dragging in the scrotum
Less Common Presentations
- Dull ache or pain in the testis (in ~30-40%)
- Epididymo-orchitis - may mimic infection, delaying diagnosis
- Gynaecomastia - due to syncytiotrophoblast hCG secretion (~15%)
- Hydrocele may coexist and mask the underlying mass
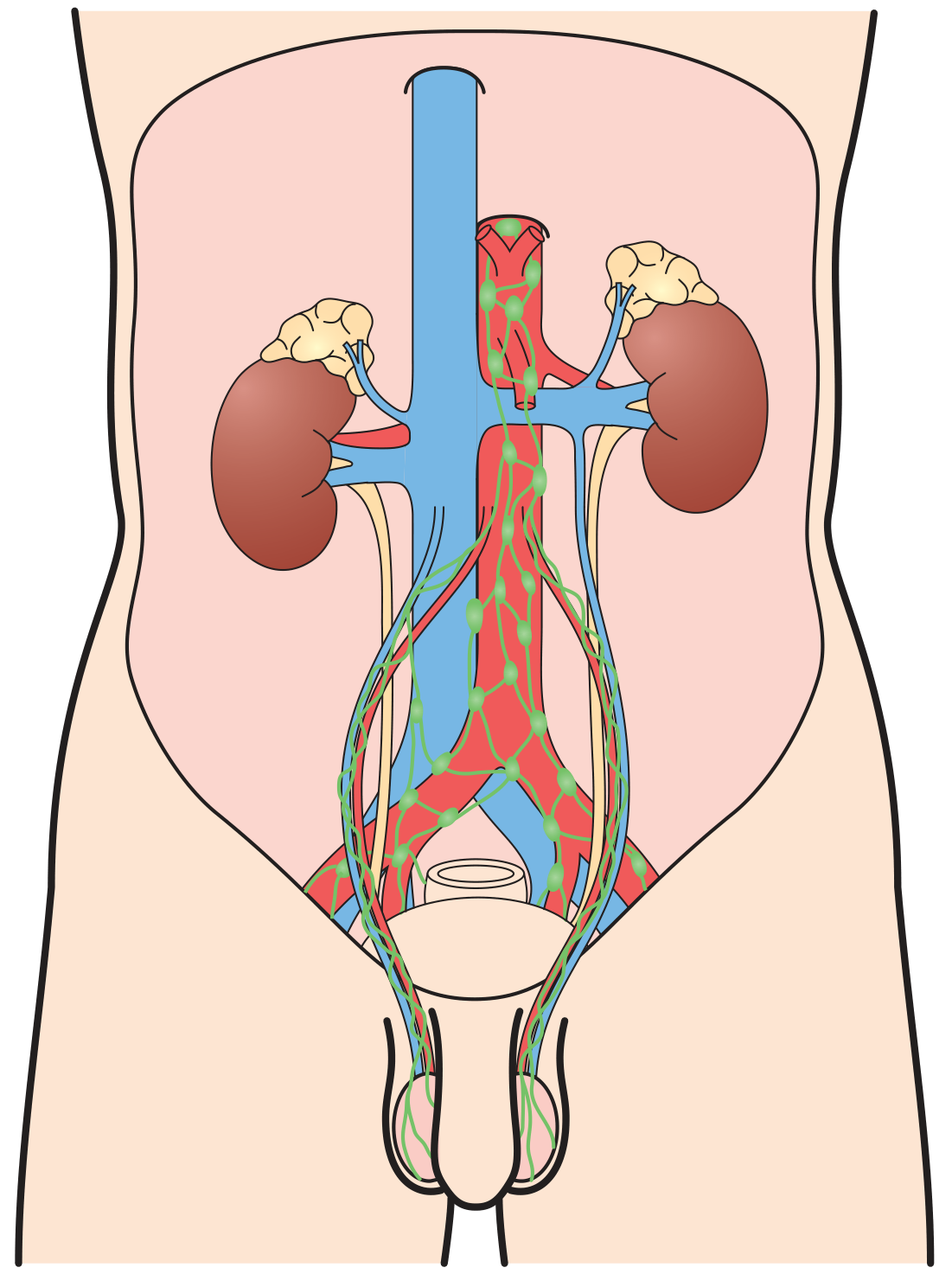
Features of Metastatic Disease
- Seminoma spreads primarily via lymphatics to the para-aortic lymph nodes (near origin of gonadal vessels) - see lymphatic drainage diagram below
- Inguinal lymph nodes are affected only if scrotal skin is involved
- Haematogenous spread is uncommon in pure seminoma
- Symptoms may include: back pain (retroperitoneal LN), respiratory symptoms (lung mets), abdominal mass
Investigations
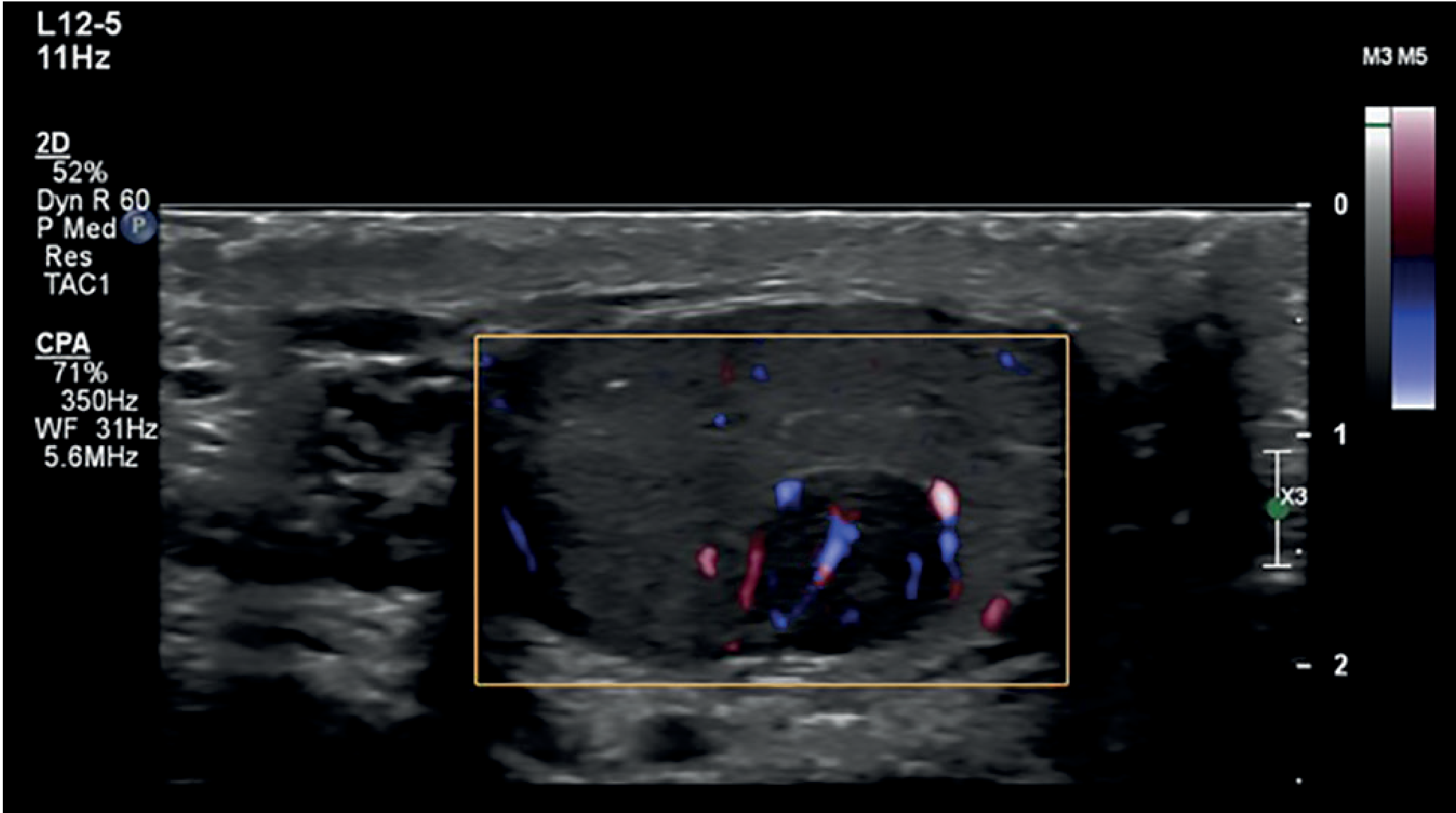
1. Ultrasound (First-Line Investigation)
- Scrotal ultrasound is the first and most important investigation
- Reveals a hypoechoic intratesticular mass with increased vascularity on Doppler
- Can detect small tumors with minimal distortion of tunica albuginea
- Sensitivity approaches 100% for intratesticular lesions
2. Serum Tumor Markers
These are measured before and after orchidectomy to assess response and detect residual disease:
| Marker | Pure Seminoma | Notes |
|---|---|---|
| AFP (Alpha-fetoprotein) | Negative / Normal | AFP elevation suggests NSGCT component - critical point |
| β-hCG | Mildly elevated in ~15% | Due to syncytiotrophoblast cells |
| LDH (Lactate dehydrogenase) | May be elevated | Correlates with tumor bulk |
| PLAP | Elevated | Less clinically used |
Key point: Pure seminoma does NOT produce AFP. Any AFP elevation should prompt reclassification as NSGCT and treatment accordingly.
3. CT Scanning
- CT chest, abdomen, and pelvis is essential for staging
- Identifies retroperitoneal lymphadenopathy, visceral metastases
- CT is also used to diagnose mediastinal seminoma (where tissue biopsy and testicular examination are also required to exclude a gonadal primary)
4. Histological Confirmation
- Radical inguinal orchidectomy - this is both diagnostic and the primary surgical treatment
- The testis is never biopsied via a scrotal approach (risk of altering lymphatic drainage and seeding inguinal nodes)
5. Staging (Royal Marsden / TNM)
| Stage | Description |
|---|---|
| I | Tumor confined to testis; no lymph node or distant spread (~80% of seminomas) |
| IIA | Retroperitoneal LN ≤2 cm |
| IIB | Retroperitoneal LN 2-5 cm |
| IIC | Retroperitoneal LN >5 cm |
| III | Supradiaphragmatic / distant metastases |
Treatment
Step 1: Radical Inguinal Orchidectomy (for all stages)
- First step in both diagnosis and treatment
- Performed via inguinal approach - never scrotal (to preserve lymphatic drainage integrity)
- Provides definitive histology and local disease control
Stage I Seminoma (~80% of cases)
Three accepted options exist; all achieve near-100% long-term cancer-specific survival. - Campbell Walsh Wein Urology
Option A: Active Surveillance (preferred at most centers)
- Most patients with CS I seminoma can be managed with surveillance alone after orchidectomy
- Relapse rate is ~15-20%, but virtually all relapses are salvaged with chemotherapy or radiotherapy
- Avoids toxicity of adjuvant treatment in ~80% who are already cured
- Requires regular CT scans and tumor markers
Option B: Adjuvant Radiotherapy
- Radiation to retroperitoneum and ipsilateral pelvis ("dog-leg" field)
- Dose: 25-35 Gy in 15-20 daily fractions
- Progression-free rate: 95-97%
- Long-term cancer-specific survival approaches 100%
- Risk: Secondary malignant neoplasms (estimated 18% at 25 years), late cardiovascular toxicity, radiation scatter to contralateral testis (oligospermia in ~8%)
Option C: Adjuvant Single-Agent Carboplatin Chemotherapy
- 1-2 cycles of carboplatin (AUC 7)
- Equivalent efficacy to radiotherapy for stage I
- Less neurotoxicity, nephrotoxicity, and ototoxicity than cisplatin
- Long-term cardiovascular and secondary cancer risks still under evaluation
Stage II Seminoma
- IIA/IIB: Radiotherapy remains effective; BEP chemotherapy is an alternative
- IIB/IIC: BEP chemotherapy (Bleomycin + Etoposide + Cisplatin) - standard 3-4 cycles
- Carboplatin-based regimens for stage II are less well-established
Stage III / Metastatic Seminoma
- Standard chemotherapy: BEP (Bleomycin, Etoposide, Cisplatin) - the backbone of treatment
- For mediastinal seminoma: BEP chemotherapy is the standard of care; surgical management is largely limited to biopsy
- Radiotherapy (RT) is reserved for patients with contraindications to chemotherapy (e.g., constrictive pericarditis, valvular disease where bleomycin pulmonary toxicity is a concern)
- Residual masses post-chemotherapy are often necrotic tissue; small residual masses may be followed up radiologically
- 5-year survival with treatment: ~90% - Current Surgical Therapy 14th Ed.
Relapsed Seminoma
- Most relapses after surveillance are salvaged with first-line BEP chemotherapy
- Isolated inguinal relapse may be salvaged with radiotherapy or surgical resection
- High-dose chemotherapy with stem cell rescue may be used in platinum-refractory disease
Summary Table
| Feature | Seminoma |
|---|---|
| Cell of origin | Germ cells (from GCNIS) |
| Peak age | 4th-5th decade |
| AFP | Always normal (pure seminoma) |
| hCG | Mildly elevated in ~15% |
| Spread | Lymphatic (para-aortic nodes) |
| Radiosensitivity | High |
| Chemosensitivity | High |
| Stage I treatment | Surveillance / RT / Carboplatin |
| Advanced treatment | BEP chemotherapy |
| 5-year survival | >90% |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Campbell Walsh Wein Urology | Smith and Tanagho's General Urology 19th Ed. | Current Surgical Therapy 14th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.