CVST work up
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a thorough CVST workup. Here is a complete, structured answer:
Cerebral Venous Sinus Thrombosis (CVST) — Workup
Clinical Suspicion: Who to Work Up
CVST accounts for 0.5–1% of all strokes. Consider it in any patient with:
- Progressive headache over days–weeks (most common symptom), or thunderclap headache
- Elevated ICP signs: papilledema, transient visual obscurations, vomiting
- Seizures (~40% of patients), focal neurological deficits, altered consciousness, or coma
- Hemorrhagic infarctions — especially multifocal, bilateral, involving gray matter and subcortical white matter simultaneously
- Presumed idiopathic intracranial hypertension (pseudotumor cerebri) — must rule out CVST first
- Any headache + elevated LP opening pressure without obvious explanation
High-risk groups: Women in the peripartum period; OCP/HRT users; patients with hypercoagulable states; patients post-surgery; those with active malignancy, head/neck infection, or inflammatory disease.
Step 1 — Initial Labs
| Test | Purpose |
|---|---|
| CBC with differential | Polycythemia, thrombocytosis, leukemia |
| BMP / CMP | Dehydration, metabolic causes |
| PT/INR, aPTT | Baseline coagulation prior to anticoagulation |
| D-dimer | A normal D-dimer has high NPV for CVST in low-probability cases; elevated D-dimer supports the diagnosis (not specific) |
| ESR, CRP | Septic/inflammatory etiology |
| Blood cultures | If septic thrombosis suspected (cavernous sinus, lateral sinus) |
| Pregnancy test | In women of childbearing age |
| Hemoglobin electrophoresis | If sickle cell suspected |
Step 2 — Thrombophilia Workup
All patients with CVST should be screened for underlying thrombophilia:
- Factor V Leiden (most common hereditary thrombophilia)
- Prothrombin G20210A mutation
- Protein C and Protein S levels
- Antithrombin III level
- Antiphospholipid antibodies (anticardiolipin IgG/IgM, anti-β2-glycoprotein I, lupus anticoagulant)
- Homocysteine level
- JAK2 V617F mutation (if myeloproliferative disorder suspected)
Note: Protein C, Protein S, and antithrombin III levels are affected by acute clot and anticoagulation — ideally recheck 3 months after stopping anticoagulation for definitive interpretation.
Step 3 — Neuroimaging
CT Head (Non-contrast) — First-Line in the ED
- Fast and widely available, but sensitivity for CVST alone is poor
- May show:
- Hyperdense sinus sign — direct visualization of thrombus in the superior sagittal sinus (SSS) or other dural sinuses
- Empty delta sign (on contrast CT) — filling defect within the sinus after contrast, pathognomonic but only present in ~30%
- Low-density areas of venous infarction, hemorrhagic transformation, small ventricles
- A normal CT does not exclude CVST
MRI Brain + MR Venography (MRV) — Gold Standard
- MRV has replaced conventional angiography for diagnosis of CVST
- MRI sequences to obtain:
- T1/T2: Abnormal signal within the sinus (variable by thrombus age)
- FLAIR: Venous infarction/edema
- DWI: Ischemic venous infarct (may have restricted diffusion)
- SWI or GRE (T2*): Blooming artifact from thrombus — highly sensitive for cortical vein thrombosis
- T1 post-contrast: Empty delta sign
- MRV (time-of-flight or phase-contrast): Non-visualization or filling defect in dural sinuses
Fig. 65.35 — Sagittal T1 MRI showing increased signal and enlargement of the superior sagittal sinus throughout most of its course, consistent with SSS thrombosis:
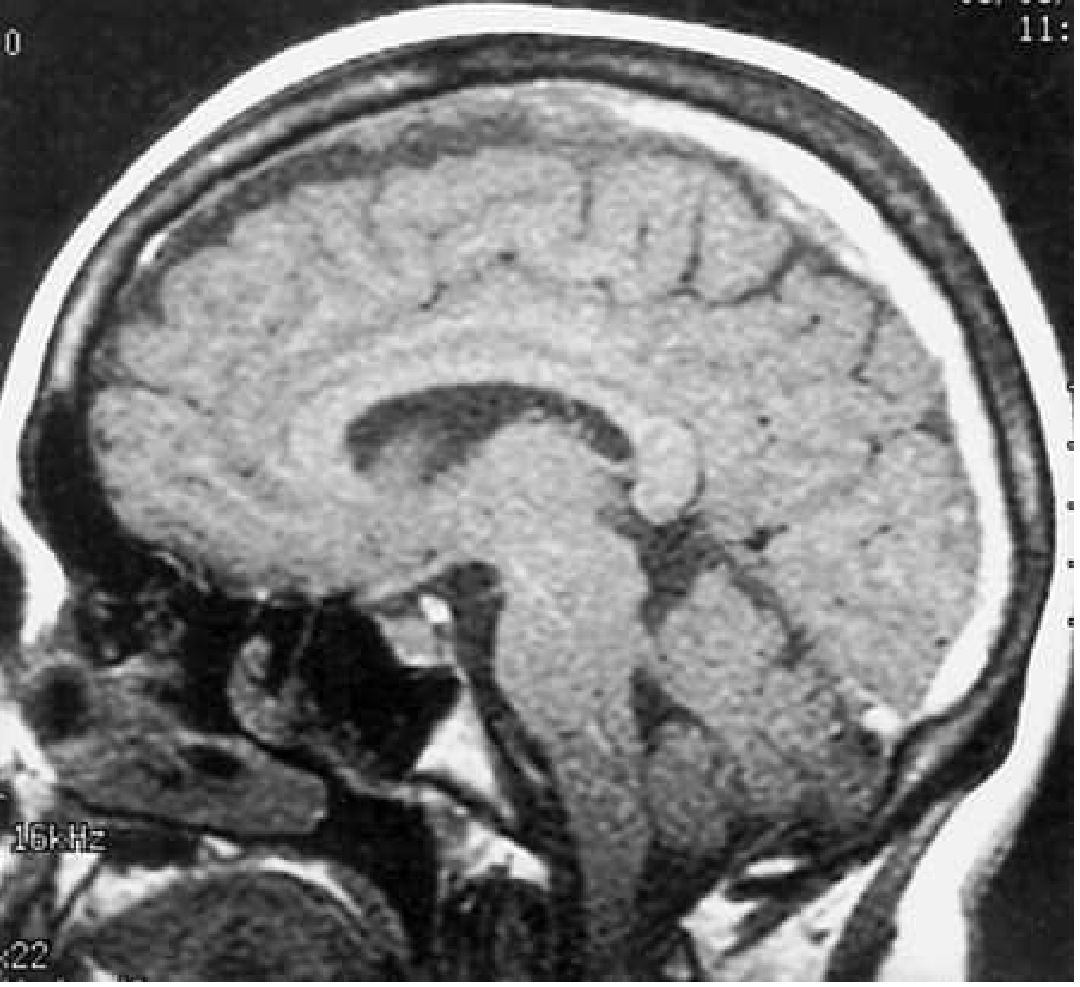
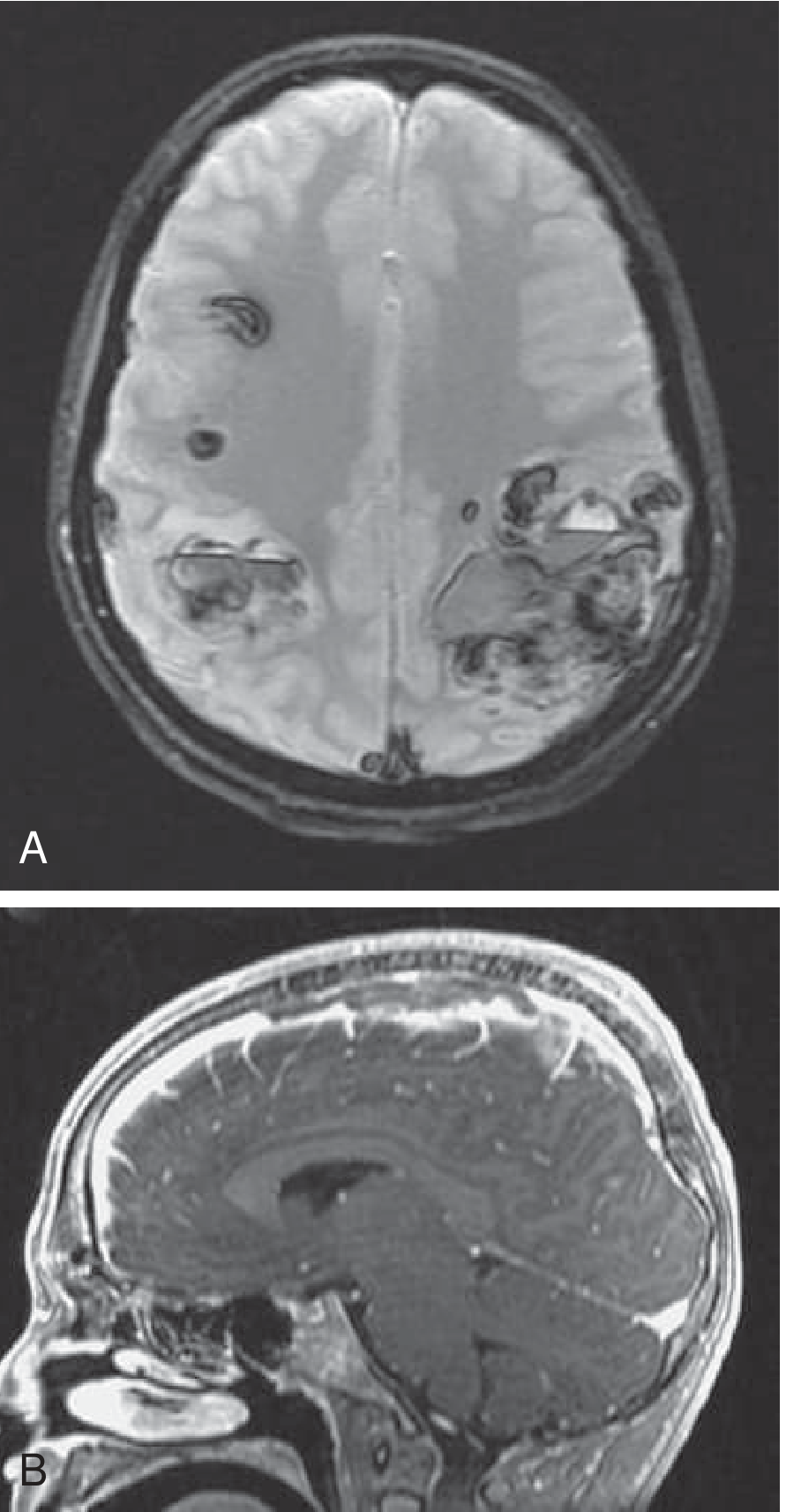
Fig. 65.36 — Bilateral hemorrhagic parietal infarctions (GRE, Panel A) and MRV showing SSS thrombosis (sagittal, Panel B) in a 14-year-old on L-asparaginase therapy:
CT Venography (CTV)
- Alternative to MRV when MRI is unavailable or contraindicated
- Excellent sensitivity and specificity; requires IV contrast and radiation
- Head ultrasound with color Doppler is used in neonates/infants
Conventional Angiography
- Rarely needed; reserved for cases where non-invasive imaging is indeterminate or when intervention is planned
Step 4 — Lumbar Puncture
- LP can be safely performed in CVST (no herniation risk from the diffuse venous pathology)
- Findings: elevated opening pressure (often >25 cmH₂O), may show xanthochromia or mild pleocytosis
- An elevated LP opening pressure in a patient with severe headache should specifically prompt MRV to rule out CVST
- LP also helps rule out meningitis/SAH if the diagnosis is unclear
Step 5 — Workup for Underlying Cause
| Category | Investigations |
|---|---|
| Infection | Blood cultures, throat swab, ENT exam, CT sinuses/mastoids (septic CVST from otitis, mastoiditis, sinusitis, facial infection) |
| Malignancy | CT chest/abdomen/pelvis, tumor markers |
| Inflammatory | ANA, ANCA, anti-dsDNA (lupus, Behçet, IBD-associated) |
| Hematologic | Peripheral smear, bone marrow biopsy if myeloproliferative disorder |
| Medications | Review OCP, HRT, tamoxifen, L-asparaginase, corticosteroids |
Summary of Key Imaging Points
| Finding | Modality | Significance |
|---|---|---|
| Hyperdense sinus | Non-contrast CT | Acute thrombus |
| Empty delta sign | Contrast CT | Filling defect in SSS, ~30% sensitive |
| Absent flow void in sinus | MRI T2 | Loss of normal "black" flow signal |
| Blooming artifact | GRE/SWI | Highly sensitive for cortical vein thrombosis |
| Non-visualization of sinus | MRV | Diagnostic of CVST |
| Hemorrhagic infarct, multifocal, bilateral | MRI | Characteristic venous pattern |
Anticoagulation Note (not to delay workup)
Once CVST is confirmed, IV heparin or LMWH is first-line, even in the presence of hemorrhagic infarction. Transition to warfarin for 3–12 months. DOACs are being studied but evidence remains limited. Anticoagulation should not be withheld pending the full thrombophilia workup — send labs before starting heparin when possible.
Sources: Bradley and Daroff's Neurology in Clinical Practice; Tintinalli's Emergency Medicine: A Comprehensive Study; Rosen's Emergency Medicine: Concepts and Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.