
Give me detail explanation of this pic related to step 1 exam With high yeild points related to mcqs step 1
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a comprehensive breakdown of the page — Inflammatory Bowel Disease (IBD): Crohn Disease vs. Ulcerative Colitis — with all the high-yield Step 1 points you need.
IBD Overview Diagram
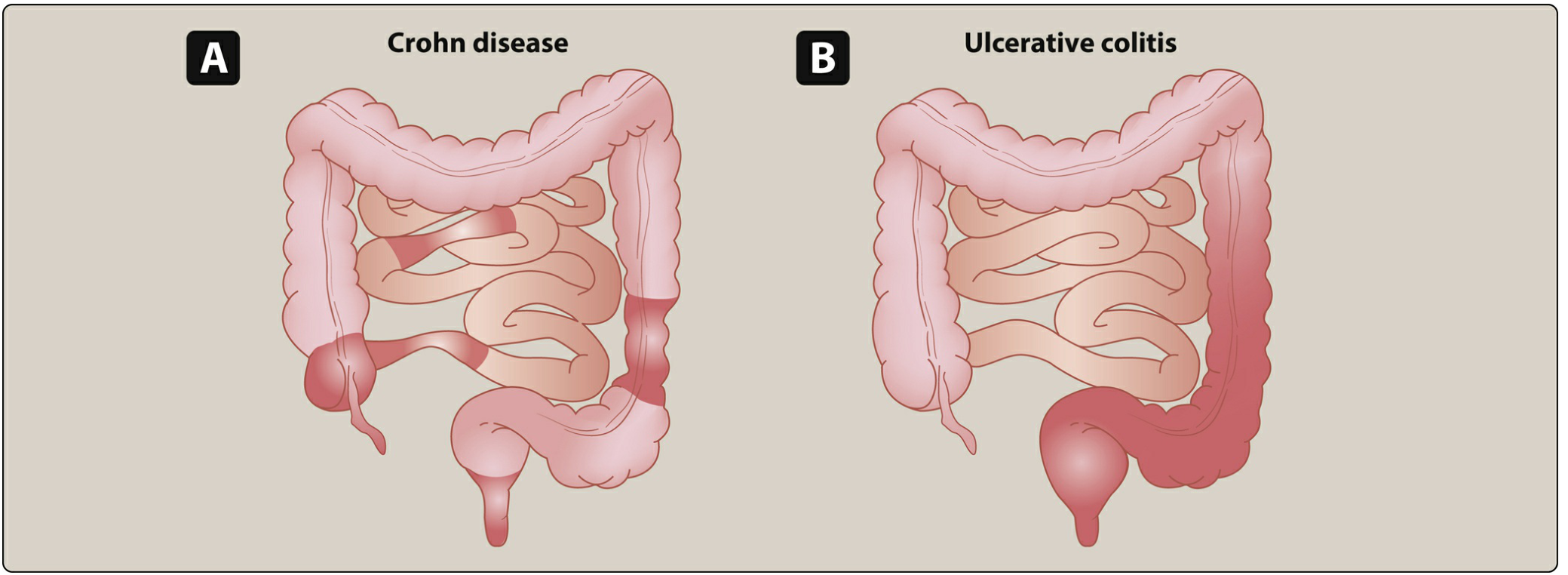
(A) Crohn disease = patchy "skip lesions" anywhere in the GI tract. (B) Ulcerative colitis = continuous involvement starting at the rectum and spreading proximally.
🔴 CROHN DISEASE
Location
- Any portion of GI tract, mouth to anus — most commonly terminal ileum + colon
- Skip lesions (normal mucosa between diseased segments) — a classic MCQ differentiator
- Rectal sparing (~40% of cases) — opposite of UC
Gross Morphology
- Transmural inflammation → leads to fistulas, strictures, abscesses
- Cobblestone mucosa (islands of edematous mucosa surrounded by deep fissures)
- Creeping fat (mesenteric fat wraps around bowel wall)
- Bowel wall thickening → "string sign" on barium swallow X-ray (narrowed lumen)
- Linear ulcers, fissures
Microscopic Morphology
- Noncaseating granulomas ← MOST HIGH-YIELD distinguishing feature
- Lymphoid aggregates
- Th1-mediated immune response (IL-12, IFN-γ, TNF)
Complications
- Fistulas (enterovesical → recurrent UTI + pneumaturia; enterocutaneous, enterovaginal)
- Phlegmon/abscess, strictures → bowel obstruction
- Perianal disease (fissures, fistulas, skin tags)
- Malabsorption/malnutrition
- ↑ risk of colorectal cancer (with pancolitis)
Intestinal Manifestation
- Diarrhea — may or may not be bloody (non-bloody more common than UC)
Extraintestinal Manifestations (shared with UC)
- Pyoderma gangrenosum, erythema nodosum
- Eye: episcleritis, uveitis
- Oral: aphthous stomatitis
- Joints: peripheral arthritis, ankylosing spondylitis (HLA-B27)
Unique to Crohn
- Kidney stones (calcium oxalate — fat malabsorption → more oxalate absorbed)
- Gallstones (bile salt malabsorption in terminal ileum)
- Anti-Saccharomyces cerevisiae antibodies (ASCA) — positive
Treatment
- Corticosteroids, azathioprine
- Antibiotics: ciprofloxacin, metronidazole
- Biologics: infliximab (anti-TNF), adalimumab
🔵 ULCERATIVE COLITIS
Location
- Colon only — ALWAYS involves the rectum and extends proximally in a continuous pattern
- No skip lesions
- Handwritten note on your page correctly says: "Mucosa rectum — continuous colonic lesions"
Gross Morphology
- Mucosal and submucosal inflammation only (NOT transmural)
- Friable mucosa with superficial ulcerations
- Loss of haustra → "lead pipe" appearance on imaging (plain film / barium enema)
- Image C in your book shows the diseased colon vs. normal
Microscopic Morphology
- Crypt abscesses and ulcers ← MOST HIGH-YIELD distinguishing feature
- No granulomas
- Th2-mediated immune response (IL-4, IL-5, IL-13)
Complications
- Toxic megacolon ← most dangerous complication (colon dilates > 6 cm, risk of perforation)
- Fulminant colitis, perforation
- ↑ risk of colorectal cancer (higher risk than Crohn; risk increases with duration and extent of disease)
Intestinal Manifestation
- Bloody diarrhea (hallmark)
Unique to UC
- Primary sclerosing cholangitis (PSC) ← most specific association
- p-ANCA / MPO-ANCA positive
- Treated with colectomy (curative!) — unlike Crohn, which recurs after resection
Treatment
- 5-aminosalicylic acid (5-ASA / mesalamine) — first-line for mild-moderate
- 6-mercaptopurine, infliximab
- Colectomy — curative
🟡 MICROSCOPIC COLITIS (bottom of page)
- Inflammatory disease of colon → chronic watery diarrhea
- Most common in older females
- Colonic mucosa appears normal on endoscopy — Key distinction: diagnosis is made by biopsy
- Two subtypes:
- Collagenous colitis — thickened subepithelial collagen band
- Lymphocytic colitis — intraepithelial lymphocytes
⚡ HIGH-YIELD STEP 1 MCQ POINTS
| Feature | Crohn | UC |
|---|---|---|
| Location | Anywhere (mouth→anus) | Colon only |
| Rectal involvement | Spared (~40%) | Always |
| Pattern | Skip lesions | Continuous |
| Depth | Transmural | Mucosal/submucosal |
| Granulomas | Yes (noncaseating) | No |
| Crypt abscesses | No | Yes |
| String sign | Yes (bowel wall thickening) | No |
| Lead pipe | No | Yes (loss of haustra) |
| Fistulas | Common | Rare |
| Perianal disease | Yes | Rare |
| Antibody | ASCA | p-ANCA |
| T-cell mediation | Th1 | Th2 |
| PSC association | Rare | Yes (p-ANCA) |
| Kidney/gallstones | Yes (terminal ileum malabsorption) | No |
| Cancer risk | Yes (with colonic involvement) | Higher |
| Curative surgery | No (recurs) | Yes (colectomy) |
| Key drug | Infliximab, metronidazole | Mesalamine, colectomy |
🧠 Classic MCQ Scenarios
- Young patient with terminal ileum disease, skip lesions, noncaseating granulomas on biopsy, positive ASCA → Crohn disease
- Patient with continuous bloody diarrhea from rectum upward, crypt abscesses, p-ANCA positive → UC
- IBD patient develops jaundice and elevated ALP → Primary sclerosing cholangitis (associated with UC)
- Crohn patient has recurrent UTIs + pneumaturia → Enterovesical fistula
- UC patient with colon dilated >6 cm on plain film → Toxic megacolon
- Patient with calcium oxalate kidney stones + chronic diarrhea → Crohn (fat malabsorption → hyperoxaluria)
- Barium swallow shows "string sign" in small bowel → Crohn stricture
- Older female with watery diarrhea but normal colonoscopy → Microscopic colitis (diagnose by biopsy)
- IBD patient develops painful skin nodules on shins → Erythema nodosum; if ulcerating skin lesion → Pyoderma gangrenosum
- Which IBD is NOT cured by colectomy? → Crohn (it can recur at anastomosis)
This is a shared conversation. Sign in to Orris to start your own chat.