
508dff70-2d9a-4483-826c-f773920d6700.jpeg
Pain pathway question
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the diagrams and content needed. Here is the complete, exam-ready answer for Question 2:
Question 2 — Complete Answer (15-yr-old with periumbilical pain → RIF: Appendicitis)
This is a classic presentation of acute appendicitis. The pain is initially periumbilical (visceral, referred) then localizes to the right iliac fossa (parietal/somatic). This pattern perfectly illustrates the physiology asked in parts (a), (b), and (c).
Part (a) — Two Theories Explaining the Basis of This Pain
1. Convergence-Projection Theory (MacKenzie's Theory)
This is the most widely accepted theory for referred pain.
- Visceral afferent pain fibers (from the appendix/gut) and somatic afferent fibers (from the abdominal wall skin at T10 dermatome) converge onto the same second-order neurons in the dorsal horn of the spinal cord (laminae I and V).
- When visceral nociceptors are stimulated, the brain misinterprets the origin of the pain signal as coming from the skin/body surface area sharing that spinal segment, because the brain has no "experience" of pain from internal organs.
- The appendix receives innervation via T10 sympathetic afferents → pain is referred to the periumbilical region (T10 dermatome).
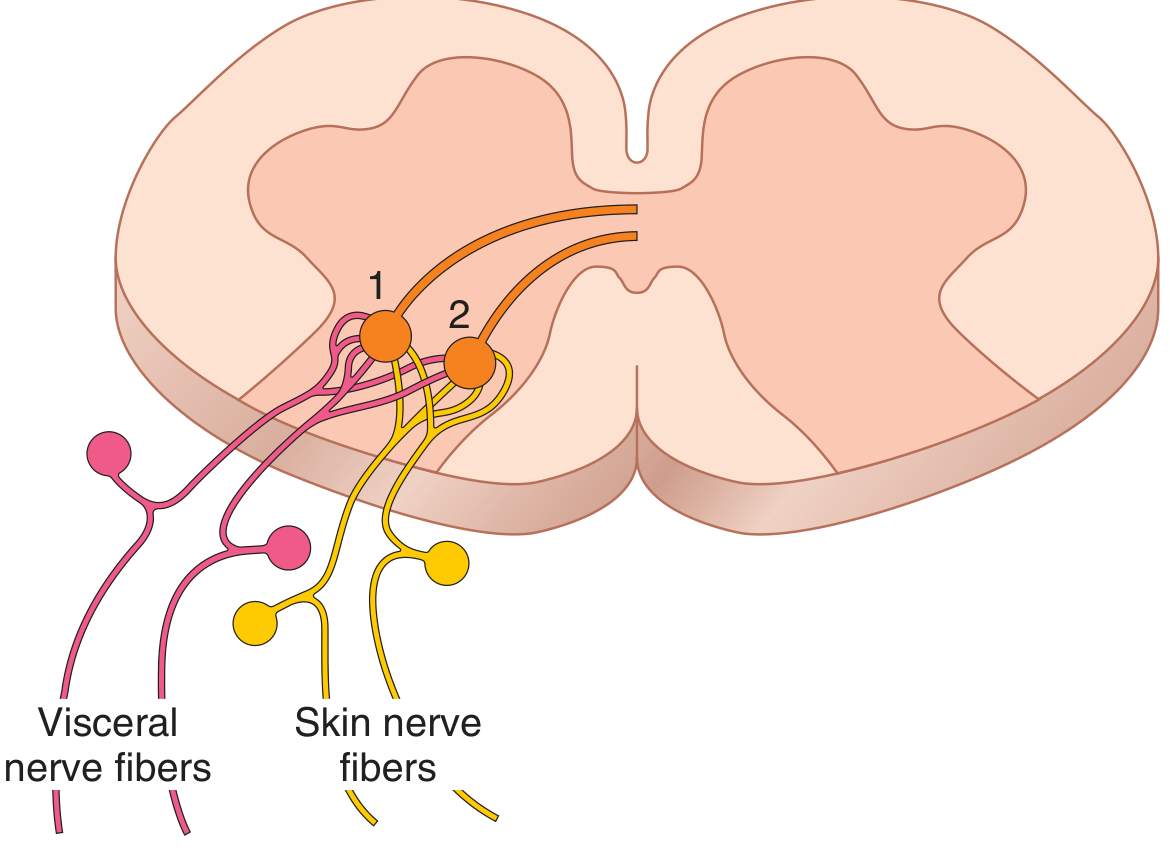
Figure: Visceral nerve fibers and skin nerve fibers synapsing on the same second-order neurons (1 and 2) in the dorsal horn — the anatomical basis of referred pain. (Guyton & Hall Medical Physiology)
2. Convergence-Facilitation Theory (Livingstone's Theory)
- Visceral pain impulses arriving at the spinal cord create a "pool" of facilitated (hyper-excitable) neurons in the dorsal horn.
- This facilitation lowers the threshold of adjacent somatic neurons, causing them to fire even with minimal input from the corresponding skin area.
- The brain then interprets this activity as coming from the somatic territory, producing the referred pain pattern.
- This theory also explains referred hyperalgesia (increased sensitivity in the referred area).
In the appendicitis scenario: Initially, visceral C-fiber afferents from the distended appendix (T10) produce diffuse, poorly localized periumbilical pain (referred). As inflammation spreads to the parietal peritoneum (which has direct somatic innervation via spinal nerves), the pain becomes sharp and well-localized to the RIF (McBurney's point) - a shift from referred visceral to direct somatic pain.
- Guyton and Hall Textbook of Medical Physiology, p. 609-610
Part (b) — Pathways of Pain with Labelled Diagram
Overview: Dual Pain Pathway System
There are two main pathways carrying pain from the periphery to the brain, corresponding to the two types of pain fibers:
| Feature | Neospinothalamic (Fast) | Paleospinothalamic (Slow) |
|---|---|---|
| Fiber type | Aδ (myelinated, 6-30 m/sec) | C (unmyelinated, 0.5-2 m/sec) |
| Pain quality | Sharp, pricking, acute | Dull, burning, aching, chronic |
| Dorsal horn laminae | Lamina I (Marginalis), V | Laminae II, III (Substantia gelatinosa) → then Lamina V |
| Neurotransmitter | Glutamate | Substance P + Glutamate |
| Decussation | Anterior commissure → contralateral anterolateral column | Same |
| Thalamic relay | Ventrobasal complex + posterior nuclear group | Intralaminar nuclei (only 10-25% reach thalamus) |
| Cortical projection | Somatosensory cortex (precise localization) | Reticular formation, brain stem, hypothalamus (diffuse suffering) |
Step-by-Step Pathway:
Step 1 - Nociceptor activation: Free nerve endings in periphery detect noxious stimuli (thermal, mechanical, chemical). In appendicitis: distension/ischemia activates C-fiber chemoreceptors.
Step 2 - Dorsal root ganglion: 1st order neurons enter dorsal horn via dorsal root.
Step 3 - Tract of Lissauer: Fibers travel 1-2 segments up/down before synapsing.
Step 4 - Dorsal horn synapse:
- Aδ fibers → Lamina I (lamina marginalis) and V
- C fibers → Laminae II & III (substantia gelatinosa), then relay to Lamina V
Step 5 - Decussation: 2nd order neurons cross in the anterior commissure to the contralateral side, then ascend as the anterolateral spinothalamic tract.
Step 6 - Brainstem: The paleospinothalamic tract gives off branches to the reticular formation, periaqueductal gray, and tectal area (mediating the emotional/suffering component of pain).
Step 7 - Thalamus: Neospinothalamic tract → VPL (ventroposterolateral) nucleus. Paleospinothalamic → intralaminar nuclei.
Step 8 - Cortex: Somatosensory cortex (SI & SII) for localization and discrimination.
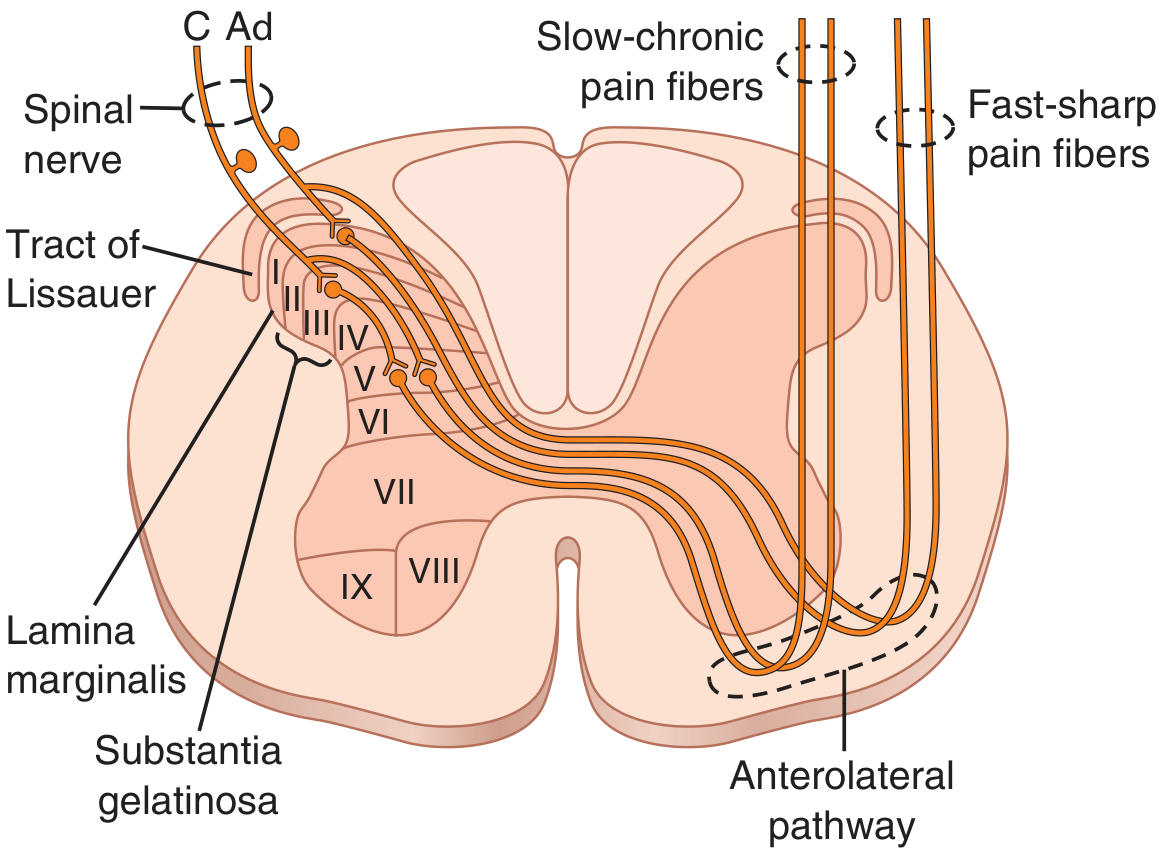
Figure: Spinal cord entry of fast-sharp (Aδ) and slow-chronic (C) pain fibers, showing laminar terminations and the anterolateral pathway. (Guyton & Hall)
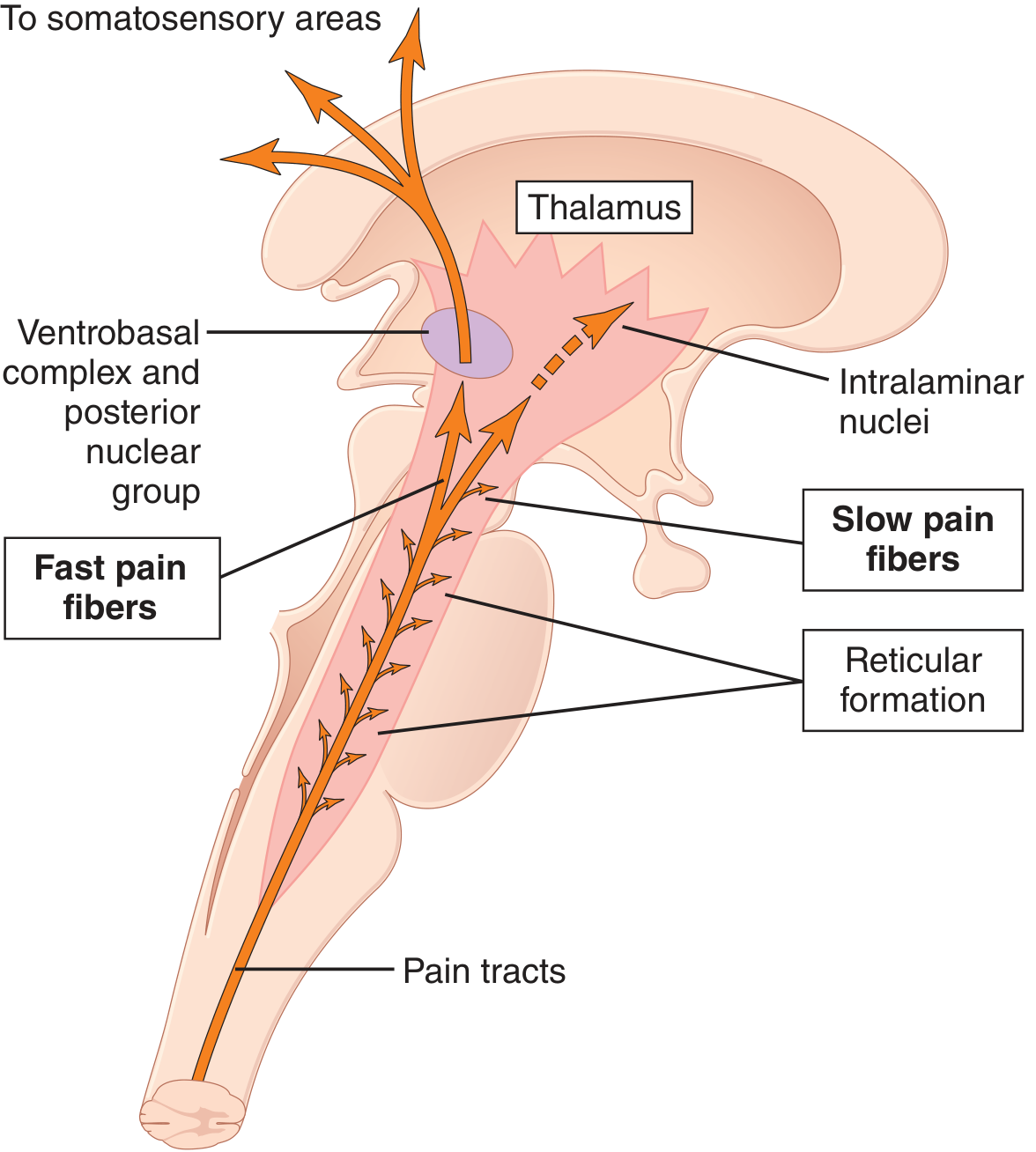
Figure: Neospinothalamic (fast) vs. paleospinothalamic (slow) pain pathways projecting to thalamus and cortex. (Guyton & Hall)
Part (c) — Supraspinal Analgesia Mechanism (Endogenous Pain Suppression)
This is the pain suppression (analgesia) system of the brain and spinal cord.
Key Components:
1. Periventricular Nuclei (Hypothalamus)
- Adjacent to the 3rd ventricle
- Receive input from higher cortical and limbic areas
- Stimulation here initiates the entire descending analgesia cascade
2. Periaqueductal Gray (PAG) - Midbrain
- The central hub of the system
- Rich in opioid receptors (mu, delta, kappa)
- Neurons here release enkephalin
- Stimulation of PAG produces profound analgesia
- Morphine microinjected here causes extreme analgesia
3. Raphe Magnus Nucleus (Pons/Upper Medulla)
- Receives enkephalinergic input from PAG
- Responds by activating serotonergic (5-HT) neurons
- These serotonergic fibers descend in the dorsolateral funiculus to the dorsal horn
4. Dorsal Horn of Spinal Cord
- Serotonin from raphe magnus activates local enkephalinergic interneurons in the dorsal horn
- Enkephalin causes:
- Presynaptic inhibition of incoming Aδ and C pain fiber terminals (reducing substance P and glutamate release)
- Postsynaptic inhibition of second-order pain transmission neurons
Cascade Summary:
Cortex/Limbic → Periventricular nuclei (Hypothalamus)
↓
Periaqueductal Gray (PAG) - releases enkephalin
↓
Raphe Magnus Nucleus - releases serotonin
↓
Dorsal Horn interneurons - release enkephalin
↓
Pre + Postsynaptic inhibition of pain transmission
↓
ANALGESIA
Endogenous Opioids Involved:
- β-Endorphin - from hypothalamus and pituitary (derived from pro-opiomelanocortin)
- Met-enkephalin and Leu-enkephalin - in brain stem and spinal cord (from proenkephalin)
- Dynorphin - found in same areas as enkephalins
These are the brain's natural morphine-like substances. Synthetic morphine and opioid analgesics work at these same receptor sites (mu opioid receptors), mimicking the endogenous analgesia system.
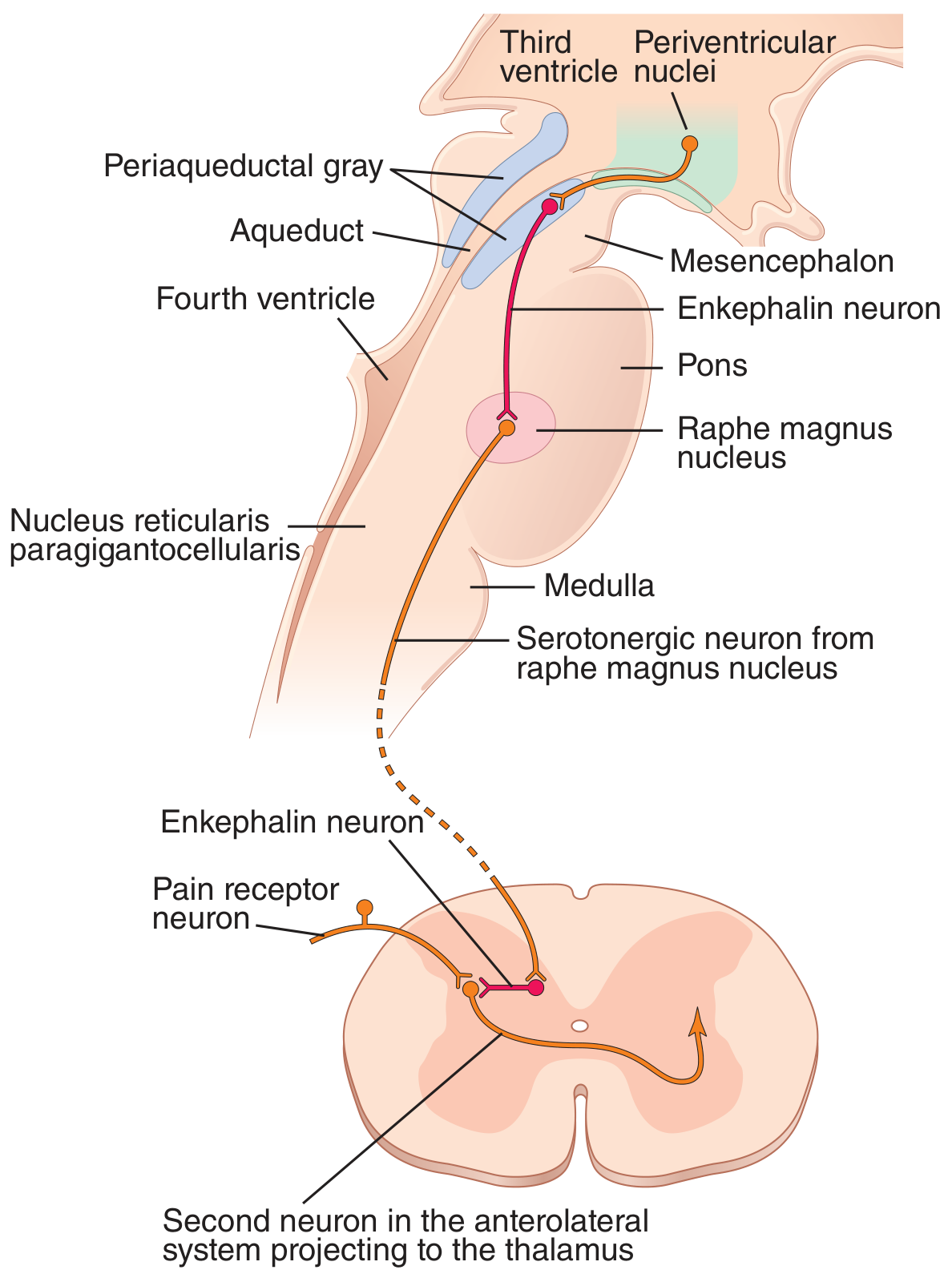
Figure: The brain's analgesia system. (1) PAG enkephalin neuron activates (2) raphe magnus serotonergic neuron, which activates (3) dorsal horn enkephalin interneuron to block pain signal presynaptically and postsynaptically. (Guyton & Hall)
Clinical Relevance:
- Stress-induced analgesia (soldiers feeling no pain after battle injuries) is mediated via this pathway
- Placebo analgesia involves endorphin release through this system
- Morphine, codeine, fentanyl - all act at mu receptors throughout this pathway
- Naloxone (opioid antagonist) blocks this system and reverses both narcotic and stress-induced analgesia
All content sourced from: Guyton and Hall Textbook of Medical Physiology (14th ed.), Chapter 49.

805b199e-7f40-438b-b16e-016226f03121.jpeg
Is this picture enough
The picture shows slide notes covering:
- Paleospinothalamic pathway (laminae II, III, V → cross → ascend → reticular formation, PAG, tectum, thalamus, hypothalamus)
- The brainstem/thalamic projection diagram (fast vs slow fibers)
- Pain modulation basics (endorphins, enkephalins, morphine)
This is good but not complete enough for a 10-mark long essay. Here is what it covers and what it misses:
✅ What Your Notes Cover Well
- The slow (paleospinothalamic) pathway terminations
- The diagram of fast vs slow fiber projections to thalamus
- Basic concept of pain modulation (endorphins/enkephalins)
❌ What is Missing (Examiner Will Look For)
For Part (b) — Pain Pathways:
| Missing Point | Why It Matters |
|---|---|
| Peripheral fibers - Aδ (6-30 m/sec) vs C (0.5-2 m/sec) | Starting point of any pathway answer |
| Neospinothalamic (fast) pathway - Lamina I & V → decussate → VPL thalamus → somatosensory cortex | Only the slow pathway is visible in your notes |
| Tract of Lissauer | Standard exam point |
| Anterior commissure decussation | Must be mentioned explicitly |
| Neurotransmitters - Glutamate (fast/Aδ), Substance P (slow/C) | Frequently asked in exams |
| Substantia gelatinosa (laminae II-III) | Labeled in Guyton diagrams |
For Part (c) — Supraspinal Analgesia:
Your notes only mention endorphins/enkephalins superficially. The examiner expects:
| Missing Point |
|---|
| Full PAG → Raphe Magnus → Dorsal Horn cascade (step by step) |
| Serotonin as the descending neurotransmitter from raphe magnus |
| Pre AND postsynaptic inhibition at dorsal horn |
| β-endorphin, met-enkephalin, leu-enkephalin, dynorphin - the four key opioids |
| Clinical examples - stress analgesia, placebo, how morphine works here |
For Part (a) — Theories of Referred Pain:
Your notes don't appear to cover the Convergence-Projection theory or Convergence-Facilitation theory at all, which are the two theories asked directly.
Verdict
Your picture covers roughly 40-50% of what is needed. Use the detailed answer I gave in the previous response - it covers all three parts completely with the labelled Guyton diagrams already embedded. That answer is exam-ready as written.
I am only talking about the pic is it fine
You're asking specifically about the diagram (the brainstem/thalamic pain pathway picture in the middle of the slide) — whether that diagram alone is sufficient to draw for the exam.
Yes, that diagram is fine for Part (b). It clearly shows:
- Pain tracts ascending from spinal cord
- Fast pain fibers → Ventrobasal complex + posterior nuclear group → Somatosensory areas
- Slow pain fibers → Intralaminar nuclei + Reticular formation → Thalamus
- The thalamus as the relay
However, add these 3 labels to make it exam-perfect:
- Aδ fibers next to "Fast pain fibers"
- C fibers next to "Slow pain fibers"
- Anterior commissure (where fibers cross to the opposite side) — this is not shown in the diagram but examiners expect it mentioned
The diagram as shown is the Guyton Fig. 49.3 equivalent — it is a standard, accepted diagram for this topic and will fetch full marks if these small additions are made.
This is a shared conversation. Sign in to Orris to start your own chat.