Myopia or hypemetropia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough, well-illustrated answer.
Myopia vs. Hypermetropia (Hyperopia)
Both are refractive errors - conditions where the eye fails to focus incoming parallel light rays sharply on the retina. The normal state (emmetropia) is shown in the top panel below:
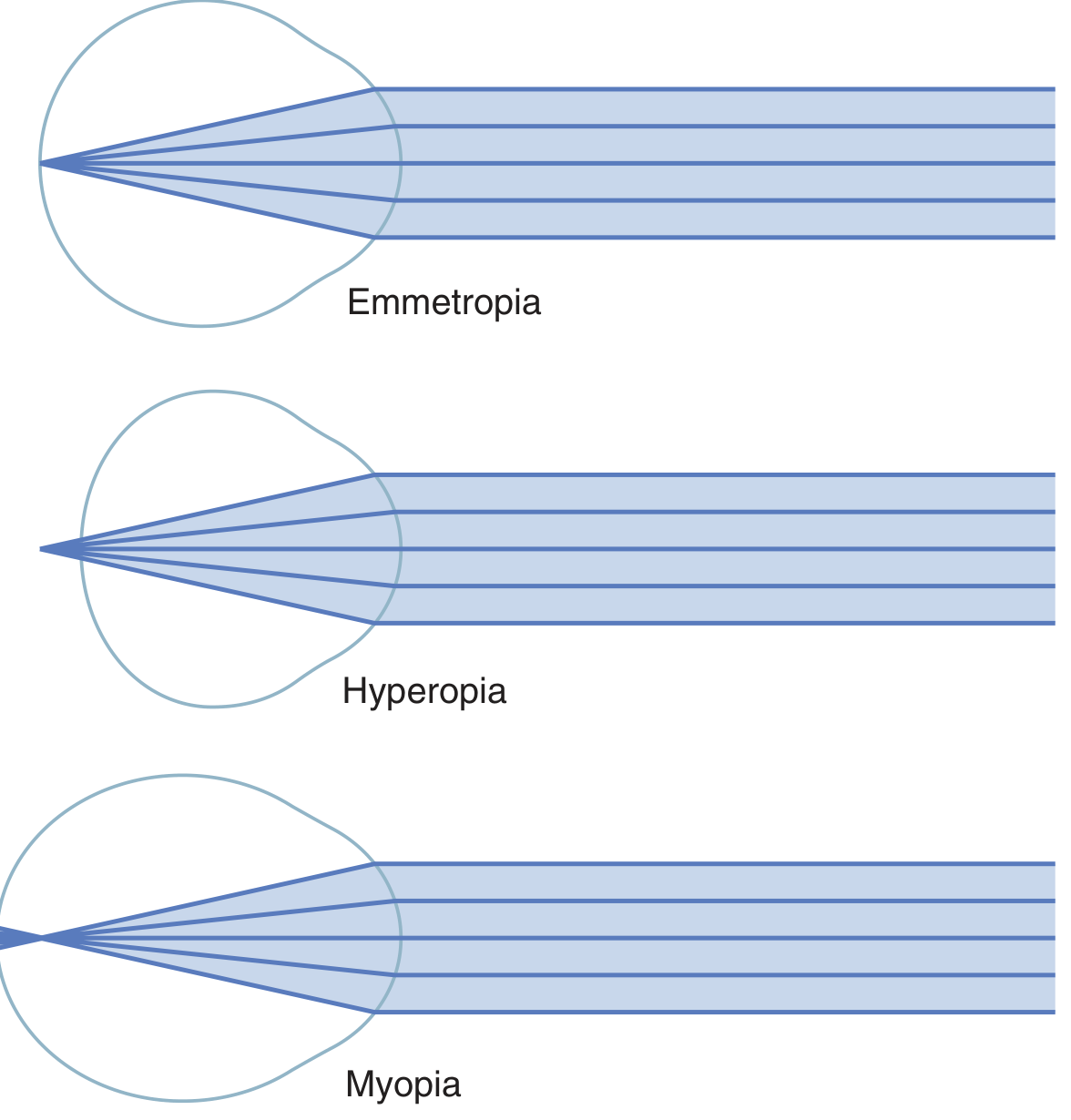
Myopia (Nearsightedness)
| Feature | Detail |
|---|---|
| Common name | Nearsightedness |
| Focus point | In FRONT of the retina |
| Cause | Eyeball too long (axial myopia), OR lens system too powerful |
| Clear vision | Near objects (close range) |
| Blurred vision | Distant objects |
| Far point | Has a definite, limited far point for clear vision |
| Accommodation | Cannot compensate - cannot reduce lens power below its relaxed state |
Key mechanism: Because the axial length is too long, parallel rays from distant objects converge to a focus before reaching the retina. The image on the retina is a blurred circle, not a point.
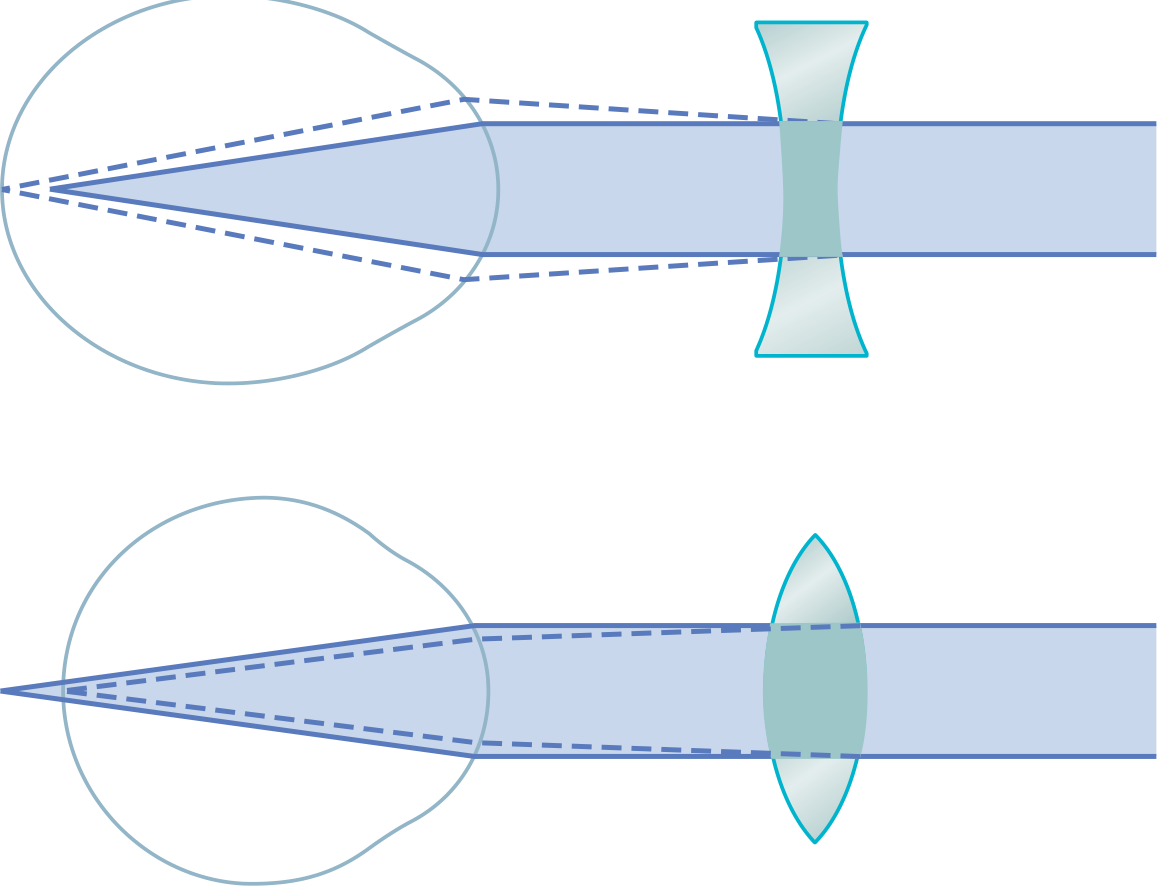
Correction: A concave (diverging, minus) lens is placed in front of the eye. This diverges rays before they enter the eye, pushing the focal point backward onto the retina.
Onset and progression: Usually discovered in childhood; progresses until age 20-25 years. Rapid progression after age 25 warrants evaluation for diabetes mellitus, trauma, or corticosteroid use (cataract formation).
Pathologic (degenerative) myopia: A partly heritable condition causing progressive posterior scleral weakening and increasing axial length (can exceed 25 mm, up to 40 mm in severe cases). Normal axial length is 20-24 mm. Complications include posterior staphyloma, retinal holes, retinal detachment, choroidal neovascularization, and intraocular hemorrhage. Associated with Marfan syndrome, Stickler syndrome, and Cornelia de Lange syndrome.
Hypermetropia / Hyperopia (Farsightedness)
| Feature | Detail |
|---|---|
| Common name | Farsightedness |
| Focus point | BEHIND the retina |
| Cause | Eyeball too short, OR lens system too weak |
| Clear vision | Distant objects (using accommodation to compensate) |
| Blurred vision | Near objects (worse with age as accommodation fails) |
| Accommodation | Can partially compensate for mild cases using ciliary muscle contraction |
| Association | Narrow-angle and angle-closure glaucoma |
Key mechanism: Parallel light rays are not bent enough by the lens system and would converge to a focus behind the retina. The ciliary muscle can contract to increase lens curvature (accommodation), functionally correcting small degrees of hyperopia - but only while accommodative reserve remains.
Correction: A convex (converging, plus) lens is placed in front of the eye to add refractive power and shift the focal point forward onto the retina.
Age-related changes: Compensatory accommodation works until approximately age 40, when the crystalline lens loses its pliability (presbyopia). At that point, bifocals or reading glasses become necessary for both distance and near tasks.
Side-by-Side Comparison
| Feature | Myopia | Hypermetropia |
|---|---|---|
| Also called | Nearsightedness | Farsightedness |
| Focal point | In front of retina | Behind retina |
| Axial length | Too long (> 24 mm) | Too short |
| Lens power | Too strong | Too weak |
| Blurred distance | Far | Near |
| Accommodation helps? | No | Yes (until presbyopia) |
| Correcting lens | Concave / minus / diverging | Convex / plus / converging |
| Associated risk | Retinal detachment (high myopia) | Angle-closure glaucoma |
| Onset | Childhood | Often asymptomatic until ~40 yrs |
Treatment Options
Myopia correction
- Spectacles/contact lenses - concave lenses; corrects non-pathologic myopia to 20/40 or better in >95% of patients
- Surface ablation (PRK) - up to 6 D of myopia
- LASIK - moderate to high myopia (up to 6-8 D depending on corneal thickness)
- SMILE - small incision lenticule extraction for myopia and myopic astigmatism
- Phakic IOL (ICL) - implantable collamer lens, -3 D to -20.5 D range, for high myopia not amenable to laser
- Clear lens extraction - for very high errors; carries retinal detachment risk
Hypermetropia correction
- Spectacles/contact lenses - convex lenses
- Surface ablation (PRK) - low degrees
- LASIK - up to 3-4 D
- Conductive keratoplasty (CK) - radiofrequency energy shrinks peripheral corneal stroma, steepening the central cornea; useful for low-moderate hypermetropia
- Clear lens extraction / phakic implants - for high degrees (up to 5 D surgically correctable)
Sources: Guyton & Hall Textbook of Medical Physiology; Kanski's Clinical Ophthalmology 10th ed.; Goldman-Cecil Medicine
Ok
Got it! Let me know if you have any questions about myopia, hypermetropia, or any other topic you'd like to explore.
Myopia
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough overview. Here is the complete guide:
Myopia (Nearsightedness) - Detailed Overview
1. Definition & Basic Optics
Myopia is a refractive error in which parallel light rays from distant objects are focused in front of the retina rather than on it, when the ciliary muscle is completely relaxed. Near objects can be seen clearly because they generate diverging rays that push the focal point back towards the retina.
Key optical concepts:
- The myopic eye has excess refractive power relative to its axial length
- There is a definite far point beyond which images are blurred
- The ciliary muscle cannot help - it can only increase lens power (not decrease it)
- Near tasks actually improve focus, so near work is typically comfortable
2. Classification / Types
By Cause (Optical Mechanism)
| Type | Mechanism |
|---|---|
| Axial myopia | Eyeball too long (most common) - normal axial length is 20-24 mm |
| Refractive (curvatural) myopia | Lens or cornea is too curved/powerful |
| Index myopia | Increased refractive index of the lens (e.g., nuclear sclerosis in aging/diabetes) |
By Degree (Diopters)
| Grade | Refractive Error |
|---|---|
| Low myopia | Up to -3.00 D |
| Moderate myopia | -3.00 to -6.00 D |
| High myopia | Greater than -6.00 D |
| Pathologic/Degenerative | Progressive, associated with structural changes |
Special Types
- Simple (physiologic) myopia - Common, stable after age 20-25, fully correctable
- Pathologic (degenerative) myopia - Progressive axial elongation beyond -6 D; axial length often > 26 mm; major cause of legal blindness
- Progressive myopia - Active axial elongation during childhood/adolescence
3. Causes & Risk Factors
Structural causes:
- Increased axial length (most common)
- Increased corneal or lens curvature
- Nuclear sclerosis (lens refractive index changes)
Etiology:
- Hereditary factors - Strong genetic component; multifactorial inheritance
- Environmental factors - Long-term near work (reading, computers) is strongly associated
- Outdoor time - Reduced time outdoors is a significant risk factor; sunlight/dopamine release is protective
- Prematurity - Premature infants have increased myopia risk
Systemic associations of HIGH myopia:
| Syndrome |
|---|
| Marfan syndrome |
| Stickler syndrome |
| Down syndrome |
| Noonan syndrome |
| Ehlers-Danlos syndrome |
| Pierre-Robin syndrome |
| Prematurity |
Progression: Typically progresses in childhood until age 20-25 years. Rapid progression after 25 years warrants evaluation for:
- Diabetes mellitus (metabolic lens changes)
- Cataract formation
- Corticosteroid use
4. Clinical Features & Diagnosis
Symptoms:
- Blurred distant vision; near vision preserved
- Squinting to see far objects
- Headaches from sustained effort to see
- In pathologic myopia: decreased vision, usually asymptomatic until middle adulthood
Workup:
- Manifest and/or cycloplegic refraction (cycloplegia relaxes accommodation for accurate measurement in children)
- IOP measurement (Schiotz or Tono-pen may underestimate IOP in highly myopic eyes)
- Dilated retinal examination with indirect ophthalmoscopy - look for retinal breaks or detachment
- Slit lamp biomicroscopy with 60/90D lens - examine macula, look for CNV
- OCT - detects CNV, macular detachment over staphyloma, foveal schisis
- Fluorescein angiography (IVFA) - for suspected choroidal neovascularization (CNV)
5. Complications (Mainly in High/Pathologic Myopia)

Posterior Segment Changes:
- Tessellated (tigroid) fundus - pale appearance from RPE attenuation, large choroidal vessels visible
- Myopic crescent - crescent of white sclera/choroidal vessels adjacent to the disc (separated from fundus by a hyperpigmented line)
- Tilted/oblique optic disc
- Lacquer cracks - ruptures in the RPE-Bruch membrane-choriocapillaris complex; fine yellow irregular lines at posterior pole (~5% of highly myopic eyes)
- Fuchs spot - raised, circular, pigmented macular lesion after subretinal hemorrhage resolves
- Posterior staphyloma - focal posterior scleral ectasia (present in ~1/3 of pathologic myopia); associated with macular hole
- Lattice degeneration - peripheral retinal thinning with risk of holes
- Myopic choroidal neovascularization (MNV) - develops in ~10% of highly myopic eyes; treated with anti-VEGF
- Rhegmatogenous retinal detachment (RRD) - much more common in high myopia
- Foveal schisis - splitting of retinal layers
Other Complications:
- Posterior subcapsular cataract and early nuclear sclerosis (which paradoxically worsens the myopia)
- Open-angle glaucoma - increased risk
- Peripapillary intrachoroidal cavitation - visual field defects mimicking glaucoma
- Heavy eye syndrome (myopic esotropia) - in very high myopia
6. Treatment & Correction
A. Optical Correction
- Concave (minus, diverging) spectacle lenses - diverge rays before entry, shift focus back onto retina
- Contact lenses - same optical principle
B. Refractive Surgery
| Procedure | Range | Notes |
|---|---|---|
| PRK (surface ablation) | Up to -6 D | Slower epithelial healing; good for thin corneas |
| LASIK | Up to -6 to -8 D | Depends on corneal thickness; most common |
| SMILE | Myopia + myopic astigmatism | Small incision, no flap |
| Phakic IOL (ICL) | -3 D to -20.5 D | Inserted behind iris, in front of lens; for very high myopia |
| Clear lens extraction | Very high errors | Carries retinal detachment risk; sacrifices accommodation |
| Radial keratotomy (RK) | Historical | No longer used |
LASIK complications: Glare, dry eye, under/overcorrection, epithelial ingrowth, diffuse keratitis, flap dislocation.
C. Myopia Progression Control (Children)
- Low-dose atropine 0.01% at bedtime - significantly slows progression in children aged 5-15 years with >1 D/year progression
- Increased outdoor time in sunshine - protective effect
- High-add (+2.50 D) soft multifocal contact lenses - for children aged 7-11 years with <5 D myopia (BLINK trial evidence; dose-dependent effect)
D. Treatment of Complications
- Retinal breaks - laser photocoagulation, cryotherapy, or scleral buckling
- CNV/MNV - anti-VEGF agents (intravitreal injections)
- Glaucoma - as per primary open-angle glaucoma protocols
- Sports protection - polycarbonate safety goggles (increased risk of choroidal rupture from minor trauma)
E. Follow-Up
- Without complications: every 6-12 months
- Dilated retinal exam each visit in high myopia patients
Sources: Kanski's Clinical Ophthalmology 10th ed.; Guyton & Hall Textbook of Medical Physiology; Goldman-Cecil Medicine; Wills Eye Manual
This is a shared conversation. Sign in to Orris to start your own chat.