Current guidelines for cervical cancer screening
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have sufficient information to provide a comprehensive, well-cited response on cervical cancer screening guidelines.
Cervical Cancer Screening Guidelines
When to Start Screening
Screening begins at age 21, regardless of the age of sexual debut. This reflects the very low prevalence of invasive cervical cancer in adolescents, the slow multiyear course of cervical carcinogenesis, and the real (if small) risk of preterm birth associated with excisional procedures performed unnecessarily in young women. — Berek & Novak's Gynecology
Screening Intervals by Age Group
| Age Group | Recommended Test | Interval |
|---|---|---|
| 21–29 years | Pap smear (cytology) alone | Every 3 years |
| 30–65 years | Pap smear alone | Every 3 years |
| 30–65 years | Pap + HPV co-testing | Every 5 years (preferred by USPSTF 2017) |
| 30–65 years | HPV test alone (primary HPV screening) | Every 5 years (USPSTF 2017) |
HPV DNA testing is not recommended under age 30 because of the high prevalence of transient HPV infection in younger women, making the test poorly specific in that age group. — Robbins, Cotran & Kumar Pathologic Basis of Disease
Special Populations (More Frequent Screening)
The following groups require more intensive surveillance:
- HIV-positive women: Pap twice in the first year, then annually
- Immunosuppressed individuals (e.g., transplant recipients, long-term corticosteroids)
- DES (diethylstilbestrol) daughters
- History of CIN 2+ or cervical cancer: Annual screening for 20 years
— Berek & Novak's Gynecology
When to Stop Screening
- Ages 65–70: Discontinuation is reasonable if there is an adequate prior screening history (typically 3 consecutive negative Pap smears or 2 consecutive negative co-tests within the prior 10 years, with the most recent within 5 years)
- Annual reassessment of risk factors is still appropriate after stopping
- Post-hysterectomy for benign indications: Screening can be discontinued if there is no prior history of high-grade CIN or cervical cancer — Berek & Novak's Gynecology
HPV Testing Details
| Test | FDA Approval |
|---|---|
| Hybrid Capture 2 | ASC-US triage, Co-test |
| Cobas HPV (L1 DNA, PCR) | ASC-US triage, Co-test, Primary HPV screening |
| APTIMA (E6/E7 mRNA) | ASC-US triage, Co-test, reflex typing for 16/18/45 |
| Cervista | ASC-US triage, Co-test |
— Berek & Novak's Gynecology, Table 16-2
Management of Abnormal Results
- ASC-US: Reflex HPV testing; if HPV positive → colposcopy
- LSIL: Colposcopic examination; confirmed LSIL can be managed conservatively (watchful waiting) or ablated (cryotherapy) depending on follow-up reliability
- HSIL: Cervical conization (superficial excision) is the standard treatment
- HPV positive, cytology normal (in women ≥30): Repeat cytology every 6–12 months — Robbins, Cotran & Kumar
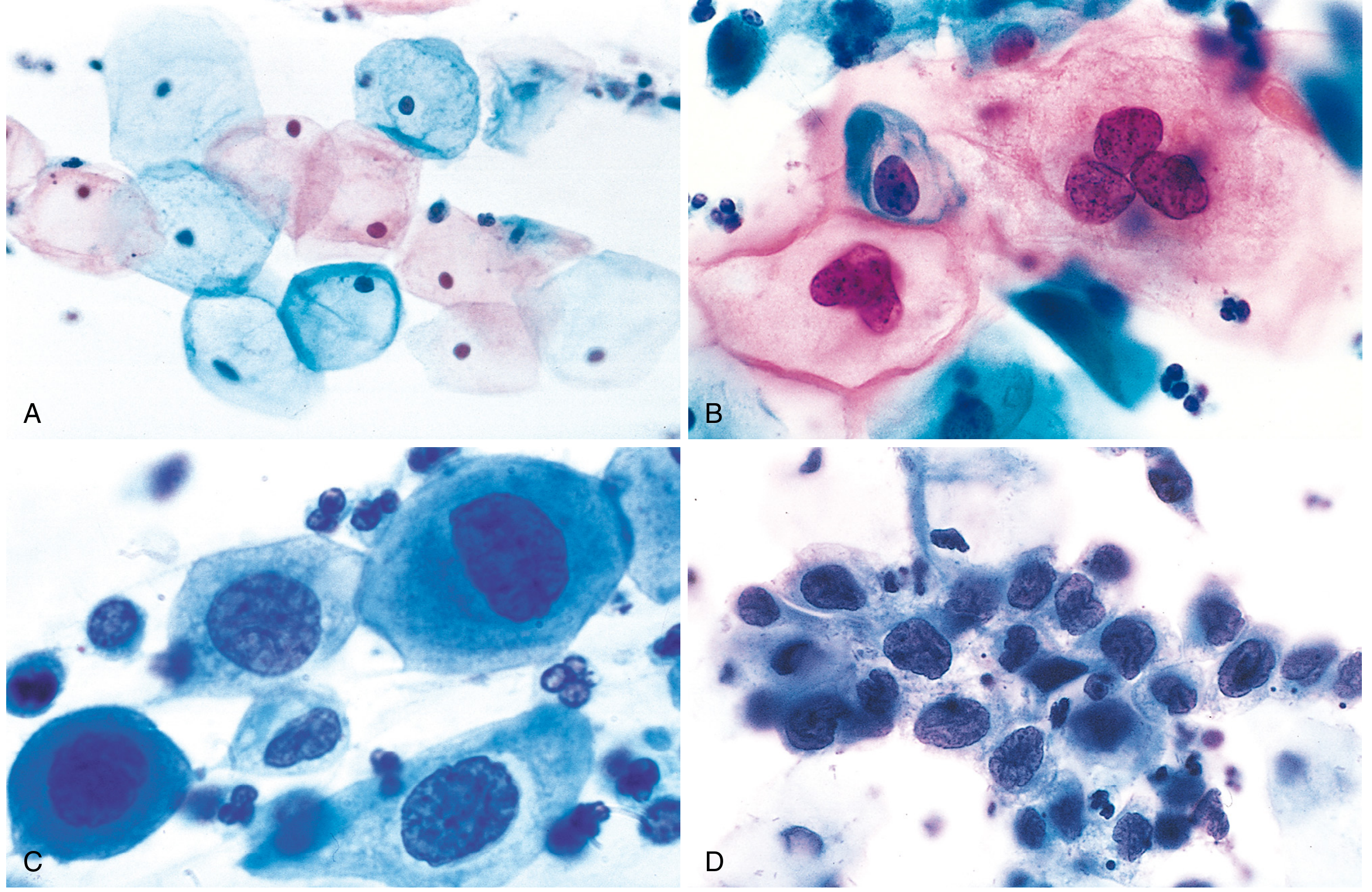
The Pap Smear — Cytologic Spectrum
The transformation zone is circumferentially scraped; cells are fixed and stained using the Papanicolaou method. The cytologic spectrum from normal to HSIL reflects a progressive reduction in cytoplasm and increase in the nucleus-to-cytoplasm ratio as differentiation is lost.
Prevention: HPV Vaccination
Vaccination against oncogenic (and low-risk) HPV types is recommended for:
- All children and adults ages 9–26 years
- Selected adults 27–45 years (shared decision-making based on risk)
— Robbins, Cotran & Kumar Pathologic Basis of Disease
Key takeaway: The USPSTF 2017 and ACS guidelines converge on starting at age 21, using cytology alone every 3 years for ages 21–29, and offering cytology + HPV co-testing or primary HPV testing every 5 years for ages 30–65. Routine annual Pap smears are no longer recommended for average-risk women. Always individualize based on risk factors and immunocompromise status.
Carcinoma lung nsccl latest update as per nccn
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, current data from Harrison's 2025, Murray & Nadel's, and Fishman's. Here is a detailed synthesis aligned with current NCCN-concordant guidelines:
Non-Small Cell Lung Cancer (NSCLC) — Current Management Guidelines
Important note: The library contains authoritative medical textbooks (Harrison's 2025, Murray & Nadel's, Fishman's). The NCCN guidelines themselves are a proprietary online resource updated continuously; the principles below are concordant with the most current NCCN framework as reflected in these texts.
Overview
NSCLC accounts for ~85% of all lung cancers and includes:
- Adenocarcinoma (most common)
- Squamous cell carcinoma
- Large cell carcinoma
5-year survival for NSCLC is ~23%, reflecting the fact that the majority present at advanced stages. — Murray & Nadel's Textbook of Respiratory Medicine
Staging-Based Treatment Framework
| Stage | General Strategy |
|---|---|
| Stage I | Surgery alone |
| Stage II | Surgery + adjuvant chemotherapy |
| Stage IIIA (resectable) | Multimodality: chemo + surgery ± immunotherapy |
| Stage IIIA/B (unresectable) | Concurrent chemoradiotherapy → consolidation immunotherapy (durvalumab) |
| Stage IV (metastatic) | Systemic therapy: targeted or immunotherapy ± chemotherapy |
— Murray & Nadel's Textbook of Respiratory Medicine
Early-Stage NSCLC (Stages I–III): Perioperative Advances
A major paradigm shift has occurred — targeted therapy and immunotherapy are now incorporated into curative-intent treatment:
| Trial | Stage | Regimen | Key Result |
|---|---|---|---|
| CheckMate 816 (Neoadjuvant) | IB–IIIA | Nivolumab + chemo × 3 cycles | EFS HR 0.63, p=.005 |
| KEYNOTE-671 (Perioperative) | II–IIIB (N2) | Pembrolizumab + chemo → surgery → pembrolizumab ~9 mo | EFS HR 0.58; OS HR 0.72 |
| IMPower010 (Adjuvant) | II–IIIA, PD-L1 ≥1% | Chemo → atezolizumab × 1 year | DFS HR 0.66 |
| KEYNOTE-091/PEARLS (Adjuvant) | IB–IIIA | Chemo → pembrolizumab × 1 year | DFS HR 0.73 |
| ADAURA (Adjuvant) | IB–IIIA, EGFR mut+ | Osimertinib × 3 years | DFS HR 0.20; OS HR 0.49 |
| ALINA (Adjuvant) | IB–IIIA, ALK fusion+ | Alectinib × 2 years | DFS HR 0.24 |
— Harrison's Principles of Internal Medicine 22E (2025)
Mandatory Molecular Testing for All Advanced NSCLC
All patients with stage IV NSCLC must undergo comprehensive molecular profiling before initiating therapy. Actionable targets and approved agents:
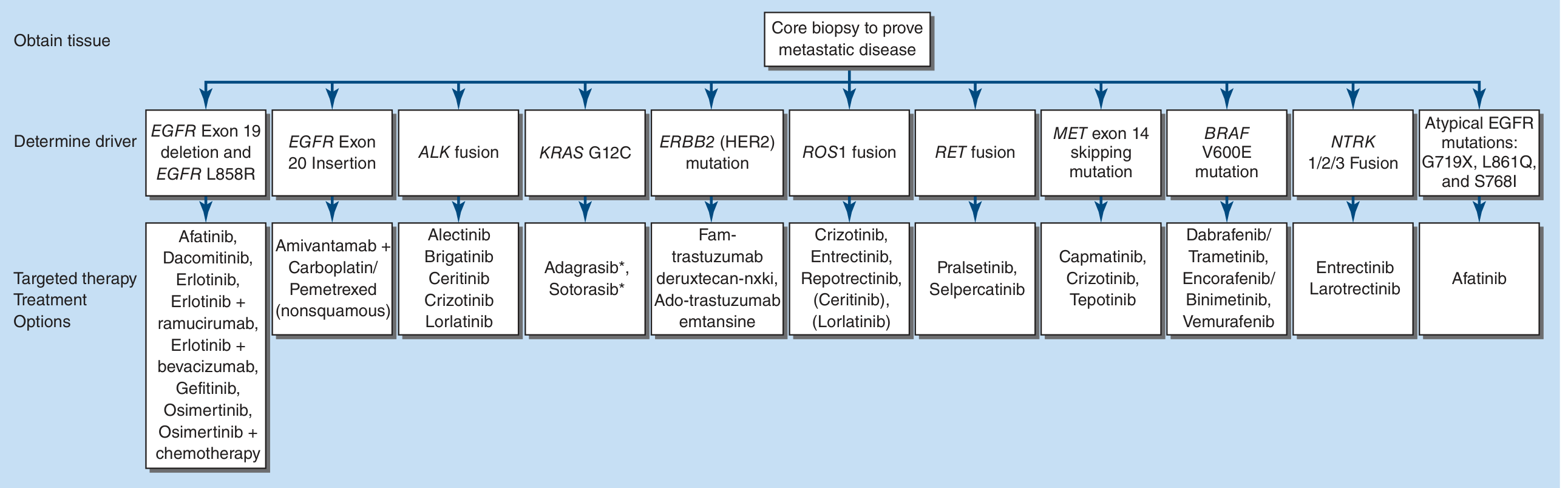
| Driver Alteration | Approved Targeted Agents |
|---|---|
| EGFR exon 19 del / L858R | Osimertinib (preferred 1st line), Afatinib, Dacomitinib, Erlotinib ± ramucirumab/bevacizumab, Gefitinib |
| EGFR exon 20 insertion | Amivantamab + carboplatin/pemetrexed |
| ALK fusion | Alectinib, Brigatinib, Lorlatinib, Ceritinib, Crizotinib |
| KRAS G12C | Adagrasib*, Sotorasib* (*2nd line) |
| ERBB2 (HER2) mutation | Fam-trastuzumab deruxtecan-nxki, Ado-trastuzumab emtansine |
| ROS1 fusion | Crizotinib, Entrectinib, Repotrectinib, (Ceritinib), (Lorlatinib) |
| RET fusion | Pralsetinib, Selpercatinib |
| MET exon 14 skipping | Capmatinib, Crizotinib, Tepotinib |
| BRAF V600E | Dabrafenib/Trametinib, Encorafenib/Binimetinib, Vemurafenib |
| NTRK 1/2/3 fusion | Entrectinib, Larotrectinib |
| Atypical EGFR (G719X, L861Q, S768I) | Afatinib |
Key rule: Patients with EGFR or ALK driver mutations derive greater benefit from TKIs than immunotherapy, even when PD-L1 is ≥50% — they should receive a TKI first, not immunotherapy. — Harrison's 2025
Stage IV NSCLC Without Actionable Mutations: Immunotherapy Framework
Treatment is guided by histology and PD-L1 expression:
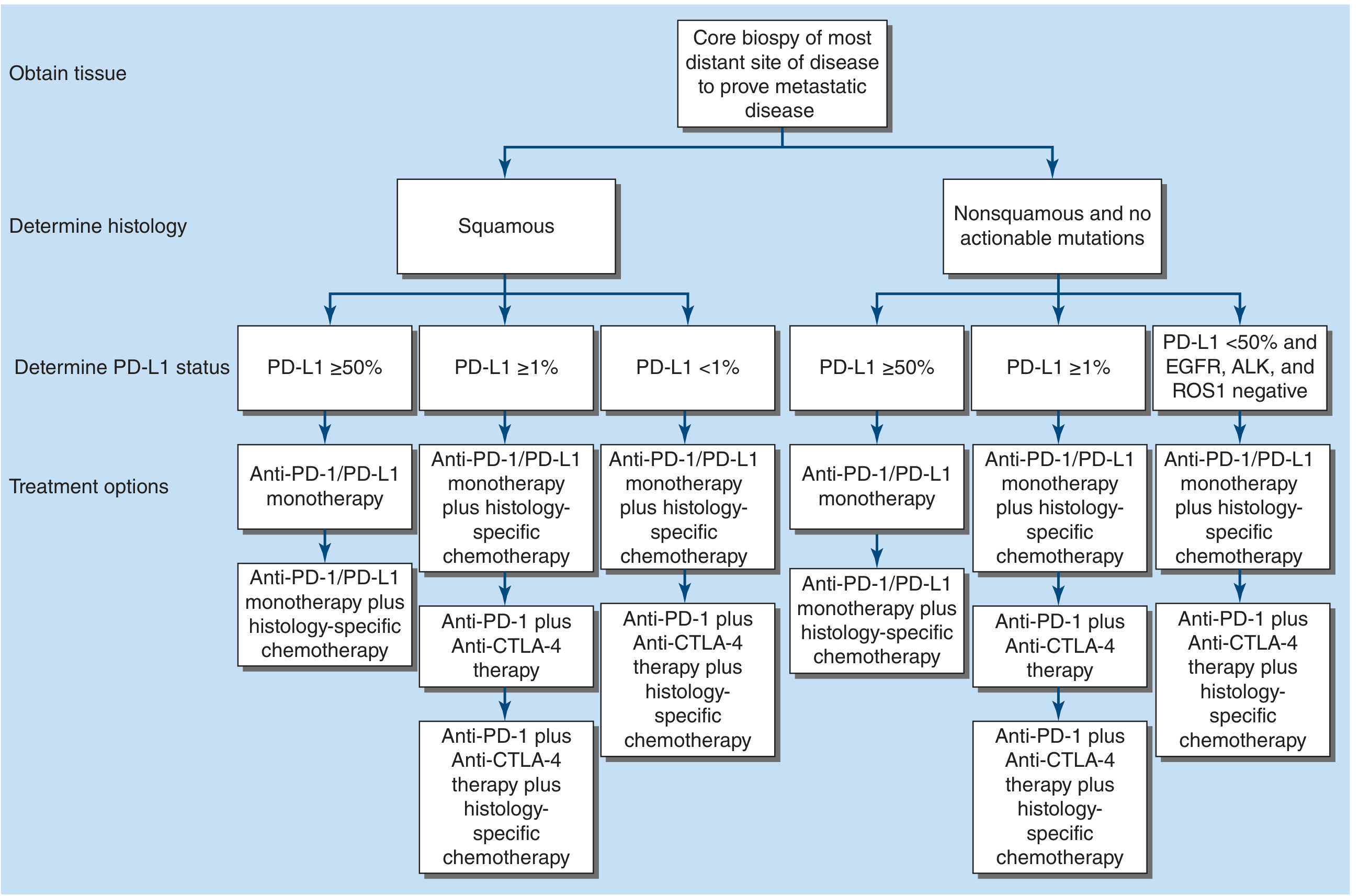
PD-L1 ≥50% (no driver mutation):
- Pembrolizumab monotherapy (KEYNOTE-024, KEYNOTE-042): preferred 1st-line
- Atezolizumab monotherapy (IMpower 110): alternative
- Nivolumab + ipilimumab (CheckMate 227): option
- Chemo + immunotherapy also acceptable
PD-L1 1–49% (no driver mutation):
- Chemo + immunotherapy preferred (monotherapy less supported)
- Anti-PD-1 + anti-CTLA-4 ± chemo
PD-L1 <1% or PD-L1 low:
- Chemo + immunotherapy combination
- Anti-PD-1 + Anti-CTLA-4 + chemo
Histology-specific chemotherapy backbone:
- Nonsquamous (adenocarcinoma): Cisplatin + pemetrexed (superior to gemcitabine; pemetrexed restricted to nonsquamous due to thymidylate synthase expression)
- Squamous: Cisplatin + gemcitabine (preferred)
- Bevacizumab (anti-VEGF): add to platinum + paclitaxel for nonsquamous only (contraindicated in squamous — hemorrhage risk)
— Murray & Nadel's; Harrison's 2025
Stage III Unresectable: Chemoradiotherapy + Durvalumab
Concurrent platinum-based chemoradiotherapy followed by consolidation durvalumab (anti-PD-L1) for up to 12 months is the standard of care for unresectable stage III NSCLC with PS 0–1 after chemoRT (PACIFIC trial). Immunotherapy also shows promise in early-stage disease. — Murray & Nadel's
Maintenance Therapy (Stage IV, Nonsquamous, Good PS)
After 4–6 cycles of platinum doublet + immunotherapy, in patients with stable/responding disease:
- Pemetrexed maintenance: 22% reduction in risk of death vs. placebo
- Bevacizumab maintenance: improved PFS (4.4 vs. 2.8 mo) and OS
- Continuation immunotherapy per initial regimen
Second-Line and Beyond
- Docetaxel ± ramucirumab (all histologies): standard after progression on platinum-based therapy; ramucirumab (anti-VEGFR2) improves PFS and OS
- Pemetrexed (2nd line, nonsquamous only)
- Afatinib (2nd line, squamous)
- Erlotinib: option in patients unsuitable for immunotherapy or chemo (OS 6.7 vs. 4.7 mo vs. placebo)
- Immunotherapy agents approved 2nd-line: nivolumab, pembrolizumab, atezolizumab
Key Summary Points
- Molecular testing is mandatory for all advanced NSCLC before any treatment decision
- Driver mutation present → targeted TKI first (not immunotherapy, even if PD-L1 high)
- Driver mutation absent, PD-L1 ≥50% → immunotherapy monotherapy (pembrolizumab)
- Driver mutation absent, PD-L1 <50% → chemo + immunotherapy combination
- Early-stage: perioperative immunotherapy (nivolumab/pembrolizumab) and adjuvant targeted therapy (osimertinib for EGFR+; alectinib for ALK+) are now standard
- Histology matters: pemetrexed for nonsquamous; gemcitabine for squamous
- Chemotherapy backbone: cisplatin or carboplatin-based doublets remain the foundation when combined with immunotherapy
— Harrison's Principles of Internal Medicine 22E (2025); Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.