What is difference between SVT and AF . Explain in detail each topic with Definition Pathogenesis Clinical features presentation/ patient presentation Lab Reports/ diagnosis/ ECG and after treatment changes Lab and treatment Relation Treatment protocol Prognosis & Curability Disease Study Lab Co-Relation Syndrome Study Treatment Changing protocols Do's 4 Don'ts. Diagnosis and DD Drug Study/combination पथ्य व अपथ्य study
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Searching Images
atrial fibrillation ECG rhythm strip irregular no P waves
Now I have comprehensive information from Harrison's 22e, Braunwald's Heart Disease, Tintinalli's Emergency Medicine, and other authoritative sources. Let me compose the complete detailed answer.
SVT vs Atrial Fibrillation (AF) — Complete Comparative Study
PART 1 — DEFINITIONS
Supraventricular Tachycardia (SVT)
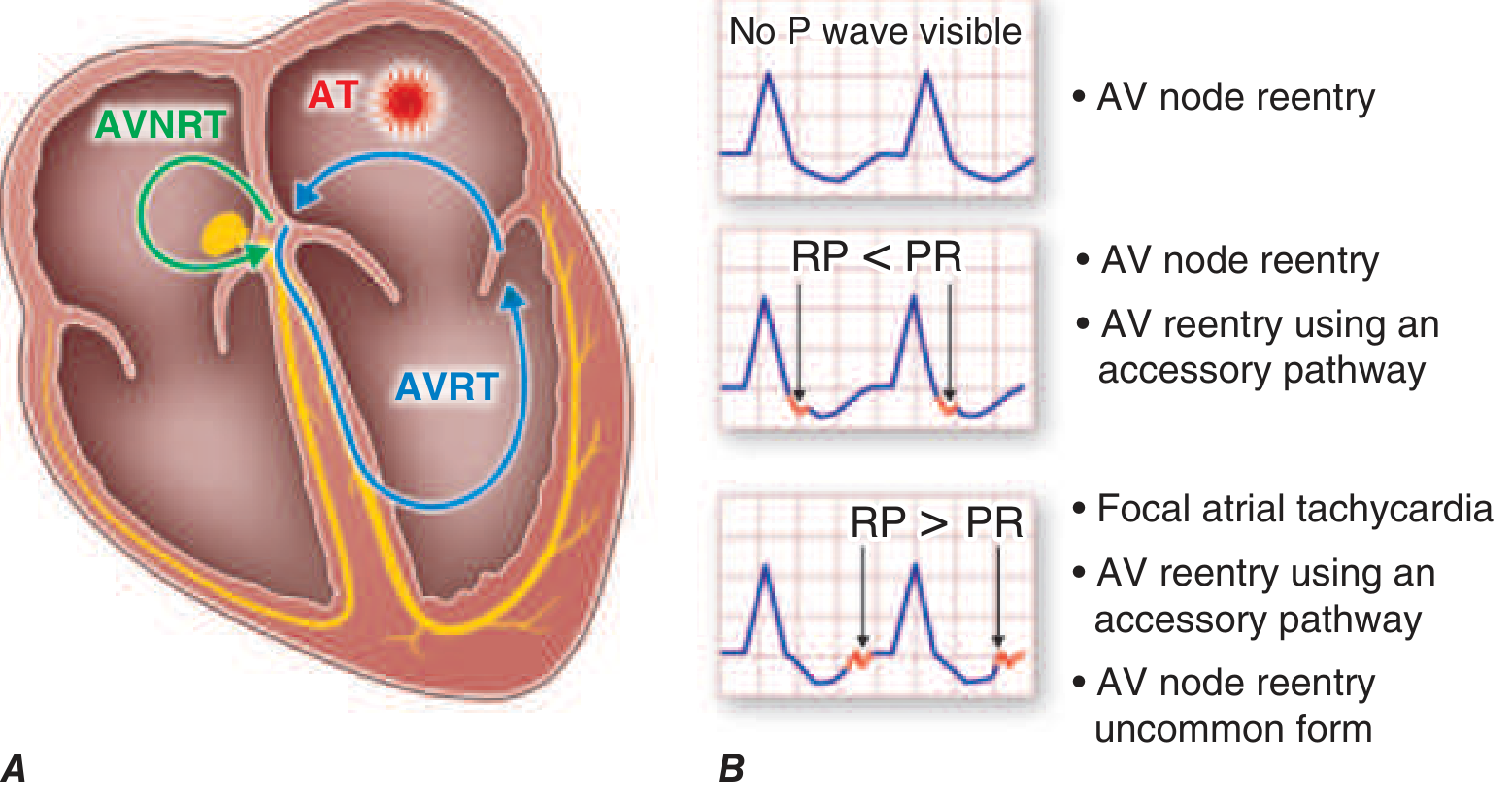
SVT is an umbrella term for all abnormal heart rhythms originating above the level of the ventricle — including the atria and the AV junction — that result in a heart rate >100 beats/min. SVTs originate from or are dependent on conduction through the atrium or AV node to reach the ventricles. In clinical practice, the term "SVT" often refers specifically to Paroxysmal SVT (PSVT), a family of tachycardias including:
- AV Nodal Reentry Tachycardia (AVNRT) — most common (60%)
- AV Reentry Tachycardia (AVRT) using an accessory pathway (e.g., WPW)
- Focal Atrial Tachycardia (AT)
"Supraventricular arrhythmias that result in an elevated heart rate (>100 beats/min) are broadly defined as supraventricular tachycardias (SVTs)." — Harrison's Principles of Internal Medicine 22E
Atrial Fibrillation (AF)
AF is a specific supraventricular arrhythmia characterized by chaotic, disorganized electrical activity throughout the atria, resulting in:
- No organized atrial contraction
- Irregularly irregular ventricular response
- Absent P waves on ECG replaced by fibrillatory (f) waves
AF is thus a subset of the SVT family, but due to its unique pathophysiology, risk profile (especially stroke), and management approach, it is always discussed separately.
PART 2 — PATHOGENESIS
SVT Pathogenesis
The three major electrophysiologic mechanisms:
1. Reentry (most common for AVNRT/AVRT)
- Requires two pathways with different conduction velocities and refractory periods
- In AVNRT: dual AV nodal pathways (fast & slow) form the circuit entirely within the AV node region
- In AVRT: accessory pathway (bypass tract) creates a macro-reentrant circuit using atrium → AV node → ventricle → accessory pathway → atrium
"Reentry is a common electrophysiologic mechanism that predisposes to most ventricular arrhythmias and to most supraventricular tachyarrhythmias." — Harrison's 22E
2. Enhanced Automaticity — ectopic focus in atrial tissue fires faster than sinus node (focal AT)
3. Triggered Activity — early or delayed afterdepolarizations (digoxin toxicity, electrolyte imbalance)
Trigger for PSVT: A premature atrial contraction (PAC) typically initiates reentry by encountering a pathway in its refractory period, forcing unidirectional conduction — the circuit is established.
AF Pathogenesis
AF has a multifactorial "final common pathway" model:
Step 1 — Triggers: Ectopic beats, especially from pulmonary vein musculature, fire rapid bursts → initiate short runs of AT or AF
- Other trigger sites: posterior left atrial wall, superior vena cava sleeves, coronary sinus, vein of Marshall
Step 2 — Substrate Development:
- Risk factors (HTN, obesity, age, diabetes, alcohol, sleep apnea, structural heart disease) → atrial remodeling
- Electrical remodeling: shortening of atrial effective refractory periods ("AF begets AF")
- Structural remodeling: atrial fibrosis, left atrial enlargement, heterogeneous conduction
Step 3 — Maintenance via Functional Reentry:
- Multiple simultaneous wandering wavelets propagate through partially refractory atrial tissue
- No fixed circuit — unstable, chaotic, self-perpetuating
"There is evidence that functional reentry is the underlying mechanism for perpetuation and maintenance of both atrial fibrillation and ventricular fibrillation. Multiple wavefronts resulting from multiple functional reentrant circuits appear to drive arrhythmia." — Harrison's 22E
Progression: Paroxysmal AF → Persistent AF (>7 days) → Long-standing Persistent AF (>1 year) → Permanent AF
- Each stage involves progressively more severe structural/electrical remodeling
PART 3 — CLINICAL FEATURES / PATIENT PRESENTATION
SVT Clinical Presentation
| Feature | Details |
|---|---|
| Onset | Sudden, abrupt (paroxysmal) — "flip" or "turn" sensation |
| Termination | Abrupt — either spontaneously or with vagal maneuvers |
| Heart rate | 150–250 bpm (typically 160–200) |
| Rhythm | Regular |
| Palpitations | Prominent — rapid, regular "fluttering" in chest or neck |
| Neck pulsations | Frog-sign (cannon A waves visible in neck) — classic for AVNRT |
| Chest discomfort | Common |
| Dyspnea | Present during episode |
| Dizziness/pre-syncope | Common |
| Syncope | Can occur if HR is very high (>220 bpm in infants, >180 bpm in children) |
| Polyuria | Post-tachycardia polyuria (atrial natriuretic peptide release) — classic |
| Duration | Minutes to hours; terminates spontaneously or requires treatment |
Precipitants: Caffeine, alcohol, emotional stress, exercise, stimulants, pregnancy
Associated conditions: WPW syndrome, Ebstein's anomaly, congenital heart disease
AF Clinical Presentation
| Feature | Details |
|---|---|
| Onset | Variable — acute or insidious; may be asymptomatic ("silent AF") |
| Heart rate | 100–180 bpm (uncontrolled) — can be slow if AV block present |
| Rhythm | Irregularly irregular — hallmark |
| Palpitations | Present — but irregular, not "flipping" |
| Dyspnea | Common — especially with rapid ventricular rate |
| Fatigue | Very common — even with rate-controlled AF |
| Decreased exercise tolerance | Loss of atrial kick (especially in stiff LV/HFpEF) |
| Chest discomfort | Common |
| Acute pulmonary edema | Can occur with abrupt AF in stiff LV (loss of atrial contribution) |
| Syncope | Less common; may be initial presentation in elderly |
| Stroke/TIA | May be first presentation — embolic stroke from LA thrombus |
| Elderly patients | Often atypical — fall, confusion, fatigue; palpitations less prominent |
Common comorbidities/precipitants (PIRATES mnemonic):
- Pulmonary disease (COPD, PE)
- Ischemic/structural heart disease
- Rheumatic heart disease (especially mitral stenosis)
- Alcohol ("holiday heart")
- Thyroid disease (hyperthyroidism)
- Electrolyte imbalance
- Surgery (post-cardiac surgery in up to 50%)
PART 4 — ECG / DIAGNOSIS / LAB REPORTS
SVT ECG Features
| ECG Feature | Finding |
|---|---|
| Rate | 150–250 bpm |
| Rhythm | Regular |
| P waves | Absent (buried in QRS) or retrograde (negative in II, III, aVF) |
| RP interval | RP < PR → AVNRT or typical AVRT; RP > PR → atypical AVNRT, AT |
| QRS | Usually narrow (<120 ms) — unless aberrant conduction or WPW |
| ST changes | ST depression common during tachycardia (rate-related ischemia) |
SVT ECG Subtypes:
- AVNRT: P waves buried in or just after QRS ("pseudo R' in V1", "pseudo S in II/III/aVF")
- AVRT (orthodromic): narrow QRS, retrograde P in ST segment (RP < PR)
- AVRT (antidromic / WPW): wide QRS, delta wave during SR, short PR
Response to vagal maneuvers / adenosine: Sudden termination (blocks AV node) — diagnostic and therapeutic
AF ECG Features
| ECG Feature | Finding |
|---|---|
| Rate | Variable (100–180 bpm uncontrolled; <100 if rate-controlled) |
| Rhythm | Irregularly irregular — no two R-R intervals equal |
| P waves | Absent — replaced by fibrillatory (f) waves |
| f waves | Chaotic, variable amplitude; best seen in V1, II, III |
| QRS | Narrow (unless BBB or WPW) |
| Baseline | Irregular, undulating — no flat isoelectric line |
12-lead ECG of AF — Coarse AF:
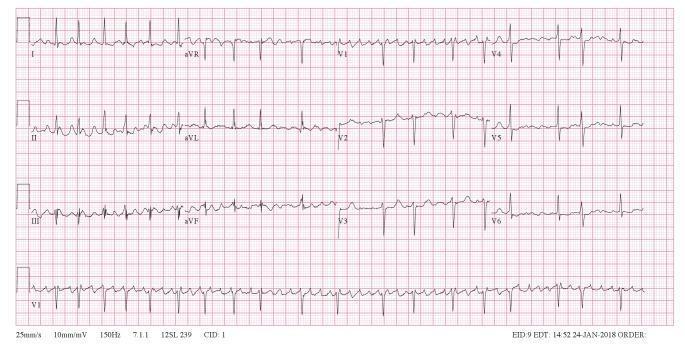 Coarse AF: absence of organized P waves, chaotic f waves prominent in V1, irregularly irregular QRS rhythm
Coarse AF: absence of organized P waves, chaotic f waves prominent in V1, irregularly irregular QRS rhythm
AF with Rapid Ventricular Response (RVR):
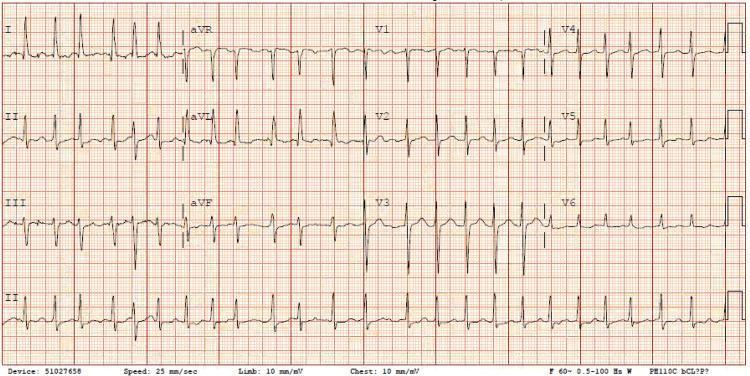 AF with RVR: HR ~149 bpm, narrow QRS, no P waves, irregularly irregular
AF with RVR: HR ~149 bpm, narrow QRS, no P waves, irregularly irregular
Key ECG Comparison Table
| Feature | SVT (AVNRT/AVRT) | Atrial Fibrillation |
|---|---|---|
| Rhythm | Regular | Irregularly irregular |
| Rate | 150–250 bpm | 100–180 bpm (uncontrolled) |
| P waves | Absent or retrograde | Absent (f waves) |
| QRS | Narrow (usually) | Narrow (usually) |
| Onset/Offset | Abrupt | Gradual or abrupt |
| Vagal response | Terminates | Slows (rate) but does not terminate |
| Adenosine | Terminates | Rate slows transiently |
Lab Investigations
For Both SVT & AF:
- Electrolytes (K+, Mg2+, Ca2+) — hypokalemia/hypomagnesemia precipitate/worsen both
- Thyroid function tests (TSH, fT4) — hyperthyroidism major cause of AF; can worsen SVT
- CBC — anemia as precipitant
- Renal function (BUN, Cr) — guides drug dosing (DOACs, digoxin)
- Liver function — affects drug metabolism (amiodarone, DOACs)
- Blood glucose — electrolyte disturbances in DM
- Cardiac enzymes (Troponin) — rule out ACS as trigger
AF-Specific:
- INR/PT — for warfarin monitoring
- CHA₂DS₂-VASc score — thromboembolic risk assessment
- HAS-BLED score — bleeding risk assessment
- BNP/NT-proBNP — assess for heart failure with AF
- Echocardiogram — LA size, LV function, valve disease, thrombus (TEE for left atrial appendage)
- Holter monitor / event recorder / implantable loop recorder — detect paroxysmal AF
SVT-Specific:
- EP Study (Electrophysiology Study) — definitive mapping of reentry circuits before ablation
- Holter/event monitor — document paroxysmal SVT episodes
After Treatment ECG Changes
| Treatment | SVT Post-Treatment ECG | AF Post-Treatment ECG |
|---|---|---|
| Adenosine / cardioversion | Return to sinus rhythm; normal P waves, regular rate | Return to sinus P waves, regular rhythm |
| Rate control drugs | No change in SVT (not first-line) | Slowed ventricular rate, still irregular |
| Successful ablation (SVT) | Delta wave disappears (WPW); normal AV conduction | — |
| Post-cardioversion (AF) | — | Normal P waves, regular rhythm; may show "electrical stunning" (short PR, biphasic P) |
PART 5 — LAB AND TREATMENT RELATION
| Lab Finding | Impact on Treatment |
|---|---|
| Hypokalemia / Hypomagnesemia | Must correct before cardioversion (risk of torsades); affects antiarrhythmic drug safety |
| Elevated TSH (hypothyroid) | Risk of amiodarone-induced hypothyroidism — monitor on long-term amiodarone |
| Low TSH (hyperthyroid) | Treat hyperthyroidism first — AF/SVT may resolve; beta-blockers preferred |
| Renal impairment (CKD) | Dose-reduce DOACs (dabigatran, rivaroxaban, apixaban); avoid dabigatran in ESRD |
| Elevated INR (supratherapeutic) | Hold warfarin; assess bleeding risk before cardioversion |
| Elevated BNP | Suggests HF — amiodarone or digoxin preferred; avoid flecainide/propafenone |
| Elevated troponin | ACS-triggered AF — anticoagulate, manage ACS simultaneously |
| LA thrombus on TEE | Delay elective cardioversion; anticoagulate ≥3 weeks before cardioversion |
| CHA₂DS₂-VASc ≥2 (men), ≥3 (women) | Mandatory anticoagulation for AF |
| HAS-BLED ≥3 | High bleeding risk — use lowest effective DOAC dose; avoid NSAIDs |
PART 6 — TREATMENT PROTOCOL
SVT Treatment Protocol
Acute (hemodynamically stable):
- Vagal maneuvers (Valsalva, carotid sinus massage, diving reflex in children, modified Valsalva) — first-line, success rate 20–50%
- Adenosine (6 mg IV rapid push → 12 mg → 18 mg) — first-line drug; terminates >90% of AVNRT/AVRT
- Give into antecubital vein, flush rapidly; half-life 10 seconds
- Contraindicated in: asthma, WPW with pre-excited AF, heart transplant
- IV calcium channel blockers — Verapamil 5–10 mg IV or Diltiazem IV (if adenosine fails)
- IV beta-blockers — Metoprolol 5 mg IV; Esmolol infusion
- Synchronized cardioversion — if hemodynamically unstable or drug failure (50–100 J biphasic)
Long-term / Preventive:
| Option | Drug/Procedure | Notes |
|---|---|---|
| First-choice | Catheter ablation | >95% cure rate for AVNRT; recommended for recurrent/symptomatic SVT |
| Rate control | Beta-blockers, verapamil, diltiazem | For infrequent, well-tolerated episodes |
| Rhythm control | Flecainide, propafenone (no structural disease); Sotalol; Amiodarone (last resort) | For patients declining ablation |
| "Pill-in-pocket" | Flecainide 200mg or propafenone 450–600mg single oral dose | For infrequent SVT; must be pre-tested in monitored setting |
AF Treatment Protocol
Three Pillars:
Pillar 1 — Anticoagulation (Stroke Prevention)
| Drug | Dose | Notes |
|---|---|---|
| Apixaban | 5 mg BD (2.5 mg BD if ≥2 of: age ≥80, weight ≤60 kg, Cr ≥1.5) | Preferred DOAC — least bleeding |
| Rivaroxaban | 20 mg OD with evening meal | Once daily convenience |
| Dabigatran | 150 mg BD (110 mg BD if age ≥80 or high bleeding risk) | Avoid in severe CKD |
| Edoxaban | 60 mg OD (30 mg if CrCl 15–50, weight ≤60 kg) | |
| Warfarin | Target INR 2–3 (2–2.5 in elderly) | Use in valvular AF (mitral stenosis), mechanical valves — DOACs NOT approved |
When to anticoagulate:
- CHA₂DS₂-VASc ≥2 (men) or ≥3 (women) → mandatory anticoagulation
- All patients ≥75 years → CHA₂DS₂-VASc ≥2 automatically → anticoagulate
- Anticoagulate ≥3 weeks before elective cardioversion (or TEE to exclude LA thrombus) + 4 weeks post-cardioversion
Pillar 2 — Rate Control
| Drug | Dose | Notes |
|---|---|---|
| Metoprolol succinate | 25–200 mg OD | First-line; preferred in CAD, HFrEF |
| Bisoprolol | 2.5–10 mg OD | |
| Diltiazem | 120–360 mg/day | Avoid in HFrEF (negative inotropy) |
| Verapamil | 120–480 mg/day | Avoid in HFrEF; contraindicated in WPW-AF |
| Digoxin | 0.125–0.25 mg OD | Only for rate control at rest; add-on; narrow TI — monitor levels |
| Amiodarone | 200 mg OD (maintenance) | Rate control last resort when others fail |
Target heart rate: <110 bpm at rest (lenient) or <80 bpm (strict, for symptomatic patients)
Pillar 3 — Rhythm Control
Pharmacologic cardioversion (if <48h or adequately anticoagulated):
- Flecainide IV/oral — rapid, effective in absence of structural disease
- Propafenone — similar to flecainide
- Amiodarone IV/oral — use in structural heart disease, HF
- Ibutilide IV — in-hospital use
Electrical cardioversion (DC cardioversion):
- Synchronized 120–200 J biphasic (200 J monophasic)
- Require adequate anticoagulation (≥3 weeks before or TEE exclusion of LAA thrombus)
- Continue anticoagulation ≥4 weeks post-cardioversion ("electrical stunning" of atria)
Antiarrhythmic drug maintenance (rhythm control):
| Structural Disease | Preferred Drug |
|---|---|
| No structural disease | Flecainide, propafenone, sotalol, dronedarone |
| HTN with LVH | Amiodarone, dronedarone |
| CAD | Sotalol, amiodarone, dronedarone |
| HFrEF | Amiodarone only |
Catheter ablation (Pulmonary Vein Isolation — PVI):
- Electrically isolates pulmonary veins (primary trigger source) from left atrium
- First-line in symptomatic paroxysmal AF; increasingly used in persistent AF
- In EAST-AFNET 4 trial — early rhythm control (including ablation) reduced CV death, stroke, and hospitalization vs. rate control alone
- In patients with HFrEF — catheter ablation superior to pharmacotherapy (improves EF)
- Success rate: ~70–80% single procedure for paroxysmal AF; lower for persistent
PART 7 — PROGNOSIS & CURABILITY
SVT Prognosis
| Aspect | Details |
|---|---|
| Mortality | Extremely low in structurally normal heart |
| Curability | Effectively cured by catheter ablation (>95% success for AVNRT, >90% for AVRT) |
| Quality of life | Significantly impaired during untreated episodes; restored after ablation |
| Recurrence on drugs | 30–50% recurrence rate — ablation far superior |
| WPW risk | Small but real risk of sudden cardiac death via pre-excited AF at very rapid rates → ablation recommended |
AF Prognosis
| Aspect | Details |
|---|---|
| Stroke risk | 5x increased risk of stroke in non-valvular AF; 17x in valvular AF + MS |
| Mortality | 1.5–2x increased all-cause mortality |
| Heart failure | AF and HF are closely linked — each worsens the other (tachycardia-mediated cardiomyopathy) |
| Curability | Not completely curable with current therapies in most patients |
| Ablation success | ~70–80% (paroxysmal); ~60–70% (persistent) — recurrence common |
| Progression | Natural history is progression: paroxysmal → persistent → permanent |
| Cognitive decline | AF independently associated with decreased cognition |
| Physical performance | Decreased in older adults even with rate control |
"AF tends to be a progressive condition, with, at this point, no definitive cure that will completely eliminate AF durably in a predictable fashion." — Harrison's 22E
PART 8 — DISEASE STUDY (Overview Summary Table)
| Parameter | SVT | AF |
|---|---|---|
| Prevalence | Common; all ages | Extremely common; increases with age (12% at ≥75 yrs) |
| Primary mechanism | AV nodal/accessory pathway reentry | Multiple functional reentrant wavelets + ectopic triggers |
| Substrate | Dual AV nodal pathways / accessory pathways | Atrial fibrosis, LA enlargement, electrical remodeling |
| Precipitants | PAC, caffeine, stress, alcohol, stimulants | HTN, age, obesity, alcohol, thyroid disease, structural heart disease |
| Risk of stroke | Very low (no independent risk unless WPW-AF) | HIGH — requires formal risk stratification |
| Major complication | Hemodynamic compromise, syncope, SCD (WPW) | Stroke, heart failure, tachycardia-cardiomyopathy |
| Definitive treatment | Catheter ablation (curative) | PVI ablation + anticoagulation (not fully curative) |
| Anticoagulation need | Not required (unless converting AF in WPW) | Required in most patients |
PART 9 — LAB CORRELATION
| Test | SVT Relevance | AF Relevance |
|---|---|---|
| ECG | Regular narrow QRS tachycardia, retrograde P | Irregularly irregular, absent P waves, f waves |
| Electrolytes | Hypokalemia/Mg2+ worsen automaticity | Critical before cardioversion; Mg2+ IV reduces AF post-surgery |
| Thyroid (TSH) | Can accelerate reentrant SVT | Hyperthyroidism major reversible cause of AF |
| Troponin | May rise with prolonged SVT (demand ischemia) | Elevated in ACS-triggered AF or tachycardia-mediated injury |
| BNP | Elevated during prolonged rapid SVT | Elevated with AF + HF; guides diuretic use |
| Holter/Event monitor | Documents paroxysmal SVT | Documents paroxysmal AF; correlates symptoms with rhythm |
| Echocardiogram | Rules out structural disease | Essential — LA size, LV function, valve disease, LAA thrombus |
| TEE | Rarely needed | Mandatory before cardioversion if anticoagulation <3 weeks |
| EP Study | Maps reentry circuit; guides ablation | Used for PVI mapping and ablation |
| INR | Not required | Target 2–3 for warfarin; affects cardioversion timing |
| Renal function | Affects drug clearance | DOAC dose adjustment in CKD; digoxin toxicity risk |
PART 10 — SYNDROME STUDY
Key Associated Syndromes
SVT-Related:
| Syndrome | Association |
|---|---|
| WPW (Wolff-Parkinson-White) | Accessory pathway + delta wave + AVRT; risk of pre-excited AF → VF → SCD |
| AVNRT | Most common cause of PSVT (60%); dual AV nodal pathways; "frog sign" in neck |
| Lown-Ganong-Levine | Short PR + normal QRS + SVT (James fiber accessory pathway) |
| Inappropriate sinus tachycardia | Elevated HR without physiologic cause; vagal dysfunction |
| POTS (Postural Orthostatic Tachycardia Syndrome) | SVT-like symptoms; autonomic dysfunction |
AF-Related:
| Syndrome | Association |
|---|---|
| Holiday Heart Syndrome | Acute AF from binge alcohol; typically self-terminating |
| Tachycardia-mediated cardiomyopathy | Prolonged rapid AF → dilated cardiomyopathy; reversible with rate/rhythm control |
| Sick Sinus Syndrome (Brady-Tachy syndrome) | Alternating sinus bradycardia and AF/SVT; requires pacemaker + anticoagulation |
| Lone AF | AF in young patients without identifiable structural/metabolic cause |
| Pre-excited AF (WPW + AF) | Life-threatening — rapid conduction down accessory pathway → VF |
PART 11 — TREATMENT CHANGING PROTOCOLS: DO'S AND DON'TS
DO'S ✅
SVT:
- Do perform vagal maneuvers first before any drug administration
- Do use modified Valsalva (semi-recumbent, leg elevation) — improves success rate
- Do give adenosine as rapid IV bolus close to the heart (antecubital) with rapid flush
- Do ablate if SVT is recurrent, poorly tolerated, or patient prefers cure
- Do stratify WPW patients for SCD risk — ablate if high-risk features (short R-R in AF <250ms, syncope)
- Do monitor ECG during adenosine administration
AF:
- Do anticoagulate before cardioversion (≥3 weeks or TEE to exclude LAA thrombus)
- Do continue anticoagulation ≥4 weeks after cardioversion (atrial stunning)
- Do treat reversible causes first (thyroid, infection, alcohol)
- Do prefer DOACs over warfarin in non-valvular AF (fewer interactions, no INR monitoring)
- Do consider early rhythm control in newly diagnosed AF (EAST-AFNET 4 trial)
- Do offer PVI ablation to symptomatic patients failing one antiarrhythmic drug
- Do use amiodarone in AF with structural heart disease / HFrEF
DON'TS ❌
SVT:
- Don't use verapamil/diltiazem in wide-complex tachycardia (may be VT — risk of VF)
- Don't use adenosine in asthma (severe bronchospasm)
- Don't use adenosine in pre-excited AF/WPW (blocks AV node → all conduction down accessory pathway → VF)
- Don't use verapamil in WPW with pre-excited tachycardia
- Don't give AV nodal blockers for wide-complex tachycardia without diagnosis
AF:
- Don't use flecainide or propafenone in structural heart disease / HF / CAD (proarrhythmic)
- Don't use verapamil/diltiazem in AF with HFrEF (EF <40%) — negative inotropic effect
- Don't use verapamil in pre-excited AF (WPW + AF) — absolute contraindication (→ VF)
- Don't stop anticoagulation just because patient is in sinus rhythm after ablation (AF may recur asymptomatically)
- Don't rely on aspirin alone for stroke prevention in AF — it is inferior to anticoagulation
- Don't cardiovert AF of unknown duration without adequate anticoagulation (3 weeks) or TEE
- Don't use dronedarone in permanent AF (increases mortality)
- Don't use amiodarone without monitoring TFTs, LFTs, PFTs (pulmonary fibrosis, thyroid toxicity, hepatotoxicity)
PART 12 — DIAGNOSIS & DIFFERENTIAL DIAGNOSIS (DD)
SVT Differential Diagnosis
| Condition | How to Differentiate |
|---|---|
| Sinus tachycardia | Regular P waves before each QRS; HR responds to maneuvers/adenosine by gradual slowing, not termination |
| Atrial flutter | Saw-tooth flutter waves 300 bpm; 2:1 or 4:1 block → regular ventricular rate ~150 bpm; adenosine unmasks flutter |
| Atrial fibrillation | Irregularly irregular; absent P waves |
| Ventricular tachycardia (VT) | Wide QRS >120ms; AV dissociation; fusion beats; capture beats |
| AVNRT vs AVRT | RP interval: short RP (<70 ms) → AVNRT; longer RP → AVRT |
| Junctional tachycardia | Regular narrow QRS; P before/after/absent; no sudden termination with adenosine |
AF Differential Diagnosis
| Condition | How to Differentiate |
|---|---|
| Atrial flutter | Regular "saw-tooth" baseline at 300 bpm; ventricular rate regular (e.g., 150 bpm at 2:1 block) |
| Multifocal AT (MAT) | ≥3 distinct P wave morphologies; isoelectric baseline between P waves |
| Frequent PACs | Isolated irregularity; P waves identifiable; regular baseline |
| AF with aberrancy | Wide QRS during AF — Ashman phenomenon; vs pre-excited AF (WPW) |
| Sinus arrhythmia | P waves identical; variation linked to respiration |
PART 13 — DRUG STUDY / COMBINATIONS
Antiarrhythmic Drug Classification (Vaughan-Williams)
| Class | Drug | Mechanism | Use in SVT | Use in AF |
|---|---|---|---|---|
| Ia | Quinidine, Procainamide, Disopyramide | Na+ channel block (intermediate kinetics) + K+ channel block | Limited | Limited (historical); procainamide for pre-excited AF |
| Ib | Lidocaine, Mexiletine | Na+ channel block (fast kinetics) | No | No |
| Ic | Flecainide, Propafenone | Na+ channel block (slow kinetics) | Yes (WPW/AVRT) | Yes — only in no structural disease |
| II | Metoprolol, Esmolol, Propranolol | Beta-blockade | Yes — rate/prevention | Yes — rate control |
| III | Amiodarone, Sotalol, Dronedarone, Ibutilide, Dofetilide | K+ channel block (↑ refractory period) | Amiodarone, Sotalol | All four used in AF |
| IV | Verapamil, Diltiazem | Ca2+ channel block | Yes — acute termination | Yes — rate control (not in HFrEF) |
| Other | Adenosine | A1 receptor → ↑ K+ conductance → AV block | Yes — acute termination | Diagnostic only |
| Other | Digoxin | Vagal ↑; Na/K ATPase inhibition | Limited | Rate control at rest; narrow TI |
Key Drug Combinations
| Combination | Use | Caution |
|---|---|---|
| Metoprolol + Digoxin | AF rate control | Bradycardia, heart block |
| Amiodarone + Warfarin | AF rhythm + anticoagulation | Amiodarone inhibits CYP2C9 → ↑ INR; reduce warfarin dose by 30–50% |
| Amiodarone + Digoxin | AF with HF | Amiodarone inhibits P-gp → ↑ digoxin levels → reduce digoxin dose by 50% |
| Flecainide + Beta-blocker | AF rhythm control / SVT prevention | Flecainide alone can organize AF into flutter with 1:1 conduction — beta-blocker prevents this |
| DOAC + P2Y12 inhibitor (no aspirin) | AF + recent ACS/PCI | Less bleeding than triple therapy (DOAC + dual antiplatelet) |
| Adenosine + Dipyridamole | ⚠️ Avoid — dipyridamole blocks adenosine metabolism → potentiates effect dramatically | |
| Sotalol + QT-prolonging drugs | ⚠️ Avoid — risk of torsades de pointes |
PART 14 — पथ्य व अपथ्य (Pathya-Apathya) Study
Dietary, lifestyle, and behavioral recommendations in the context of SVT and AF.
पथ्य (Beneficial — Do's)
आहार (Diet):
- Low-sodium diet — reduces hypertension-driven AF substrate
- Mediterranean diet — reduces AF recurrence and cardiovascular events
- High-potassium foods (bananas, leafy greens, avocado) — maintains electrolyte balance
- Magnesium-rich foods (nuts, seeds, dark leafy greens) — reduces atrial irritability
- Omega-3 fatty acids (fish, walnuts, flaxseed) — anti-inflammatory; reduces AF substrate
- Adequate hydration — dehydration can trigger SVT/AF
- Green tea (light) — antioxidant properties; however, avoid excess (caffeine)
विहार (Lifestyle):
- Moderate aerobic exercise — reduces AF burden, improves vagal tone
- Weight loss (obesity management) — reduces LA size, AF recurrence (LEGACY trial: weight loss >10% → 46% AF-free)
- Sleep hygiene — treat obstructive sleep apnea (CPAP reduces AF recurrence)
- Stress management — yoga, meditation, pranayama reduce SVT/AF triggers
- Alcohol cessation — holiday heart syndrome; alcohol is a direct AF trigger
- Smoking cessation — reduces cardiovascular risk and atrial inflammation
- Regular INR monitoring (if on warfarin) — strict compliance
- Medication compliance — take antiarrhythmics and anticoagulants as prescribed
अपथ्य (Harmful — Avoid)
आहार (Dietary Avoid):
- Caffeine excess (coffee, energy drinks, cola) — triggers SVT and AF in susceptible patients
- Alcohol — even moderate intake triggers AF; binge drinking = holiday heart
- High-fat, processed, fried foods — promote inflammation and metabolic syndrome
- Excessive salt — worsens hypertension → AF substrate
- Vitamin K–rich foods in excess (spinach, kale) if on warfarin — destabilizes INR
- Grapefruit / grapefruit juice — inhibits CYP3A4 → increases levels of some antiarrhythmics and some DOACs (rivaroxaban, apixaban)
- Liquorice (mulethi) — causes pseudohyperaldosteronism → hypokalemia → worsens arrhythmia
विहार (Lifestyle Avoid):
- Strenuous competitive exercise without cardiac clearance (WPW — SCD risk)
- Sleep deprivation — increases sympathetic tone, AF triggers
- Emotional stress / anger — catecholamine surge triggers reentrant circuits
- Self-medication / herbal remedies without physician guidance — many contain ephedrine-like compounds (e.g., ma huang, bitter orange) → potent arrhythmogenic
- Over-the-counter decongestants (pseudoephedrine, phenylephrine) — trigger SVT/AF
- NSAIDs (ibuprofen, diclofenac) — increase AF risk; increase bleeding risk with anticoagulants
- Obesity — independent risk factor for AF; worsens SVT frequency
- Tobacco / smoking — directly proarrhythmic; increases cardiovascular burden
- Driving / operating machinery during recurrent uncontrolled SVT/AF episodes
- Missed doses of anticoagulants — catastrophic stroke risk in AF
Summary Comparison Table
| Aspect | SVT (PSVT) | Atrial Fibrillation |
|---|---|---|
| Definition | Regular tachycardia from AV node/atrium, >100 bpm | Chaotic atrial electrical activity, irregularly irregular |
| Mechanism | AV nodal / accessory pathway reentry | Multiple functional reentrant wavelets + PV triggers |
| Heart rate | 150–250 bpm | 100–180 bpm (uncontrolled) |
| Rhythm | Regular | Irregularly irregular |
| P waves | Absent/retrograde | Absent (f waves) |
| Vagal/Adenosine | Terminates | Slows rate transiently |
| Stroke risk | Very low | High — anticoagulation required |
| Curative treatment | Catheter ablation (~95%) | PVI ablation (~70–80%); not fully curative |
| Anticoagulation | Not needed (except WPW-AF) | Central to management |
| Prognosis | Excellent, essentially curable | Progressive condition; ongoing risk management |
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Braunwald's Heart Disease 12th Ed | Tintinalli's Emergency Medicine | Miller's Anesthesia 10e | Fuster & Hurst's The Heart 15th Ed | Katzung's Basic & Clinical Pharmacology 16th Ed | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.