Define pain. Difference between preventive and preemptive analgesia
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive answer synthesized from authoritative anesthesia and physiology textbooks.
Definition of Pain
The International Association for the Study of Pain (IASP) defines pain as:
"An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage."
Key notes on this definition:
- Pain is always a personal experience — it has both sensory and emotional/psychological components.
- Pain can exist in the absence of tissue damage or identifiable pathophysiology. If a patient reports an experience in the same way as pain caused by tissue damage, it should be accepted as pain.
- Pain is distinct from nociception, which is defined as the neural process of encoding noxious stimuli (neurophysiologic activity in peripheral sensory neurons and higher nociceptive pathways). Nociception is not synonymous with pain.
Classification of Pain
| Type | Features |
|---|---|
| Acute (physiologic) | Sudden onset, recedes with healing; serves a protective role ("good pain") |
| Chronic (pathologic) | Persists >3 months; often refractory to NSAIDs/opioids; may be inflammatory or neuropathic |
| Neuropathic | Results from nerve injury; features burning, shooting pain, allodynia, hyperalgesia |
— Ganong's Review of Medical Physiology, 26e | Miller's Anesthesia, 10e
Preemptive vs. Preventive Analgesia
Preemptive Analgesia (older concept)
- Defined as an analgesic intervention administered before surgical incision that is more effective at pain relief than the same intervention given after surgery.
- The rationale: blocking nociceptive input before tissue injury prevents the establishment of central sensitization in the dorsal horn (wind-up, facilitation, expansion of receptive fields, long-term potentiation).
- Clinical reality: Randomized controlled trials have had mixed results. A single analgesic treatment before incision does not reduce postoperative pain beyond the expected duration of the analgesic effect. Once the block diminishes, surgical injury can reinitiate central sensitization.
- This terminology is now considered obsolete and has largely fallen out of favor.
Preventive Analgesia (current concept)
- Defined as any antinociceptive regimen delivered at any time during the perioperative period that attenuates pain-induced sensitization.
- Timing is not the defining criterion — the intervention can be preoperative, intraoperative, or postoperative.
- The focus is on intensity and duration of the analgesic intervention, not when it starts.
- Goal: block the development of sustained chronic pain by preventing NMDA receptor activation in the dorsal horn.
Three Critical Principles for Successful Preventive Analgesia:
- Depth: The analgesia must be adequate to block all nociceptive input during surgery.
- Extent: The technique must cover the entire surgical field.
- Duration: The analgesia must encompass both the surgical and post-surgical periods.
Patients with pre-existing chronic pain may respond less well due to pre-existing nervous system sensitization.
Summary Comparison
| Feature | Preemptive Analgesia | Preventive Analgesia |
|---|---|---|
| Timing | Must be before incision | Any time perioperatively |
| Mechanism targeted | Central sensitization from incision only | Central sensitization from incision + inflammation + postoperative pain |
| Key parameter | Timing of intervention | Intensity + duration of intervention |
| Clinical evidence | Mixed/negative trials | Broader, more clinically applicable |
| Current status | Obsolete terminology | Current standard concept |
Maximal clinical benefit is observed when there is complete multi-segmental blockade of noxious stimuli extended into the postoperative period, using intensive multimodal analgesic regimens.
— Miller's Anesthesia 10e | Barash Clinical Anesthesia 9e | Cummings Otolaryngology
Define pain. Difference between preventive and preemptive analgesia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive, textbook-sourced answer.
Definition of Pain
The International Association for the Study of Pain (IASP) defines pain as:
"An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage."
Key points in the definition:
- Pain is always a personal experience — it has both sensory (physical) and emotional/psychological dimensions.
- Pain can occur in the absence of tissue damage or identifiable pathophysiology. If a patient reports an experience consistent with pain, it must be accepted as pain.
- Pain is distinct from nociception: nociception is the neural process of encoding noxious stimuli — neurophysiologic activity in peripheral nociceptors and higher pathways. Nociception is not synonymous with pain.
Classification:
| Type | Characteristics |
|---|---|
| Acute (physiologic) | Sudden onset; recedes with healing; serves a protective role ("good pain") |
| Chronic (pathologic) | Persists or recurs for >3 months; often refractory to NSAIDs/opioids |
| Inflammatory | From tissue inflammation; mediated by bradykinin, prostaglandins, substance P, histamine |
| Neuropathic | From nerve injury (cutting, traction, compression); burning/shooting quality, allodynia, hyperalgesia |
— Miller's Anesthesia 10e; Ganong's Review of Medical Physiology 26e
Preemptive vs. Preventive Analgesia
Preemptive Analgesia (older, now obsolete concept)
Definition: An analgesic intervention administered before surgical incision that is more effective at relieving postoperative pain than the same intervention given after surgery.
Rationale: Blocking nociceptive input before tissue injury was hypothesized to prevent the establishment of central sensitization in the dorsal horn — thereby preventing pain hypersensitivity, reducing hyperalgesia, and reducing the magnitude and duration of postoperative pain.
Why it failed clinically:
- A single analgesic treatment before incision does not reduce postoperative pain beyond the expected duration of the analgesic effect.
- Once the block diminishes, surgical injury can reinitiate central sensitization.
- Randomized controlled trials have had mixed/negative results.
- The concept is now considered obsolete and has fallen out of favor.
Preventive Analgesia (current concept)
Definition: Any antinociceptive regimen delivered at any time during the perioperative period (preoperative, intraoperative, or postoperative) that attenuates pain-induced sensitization.
Key distinction from preemptive: The focus is not on timing but on the intensity and duration of the analgesic intervention.
Goal: Block the development of sustained chronic pain by preventing NMDA receptor activation in the dorsal horn — the mechanism underlying wind-up, facilitation, central sensitization, expansion of receptive fields, and long-term potentiation.
Three critical principles for success:
- Depth — Adequate to block all nociceptive input during surgery
- Extent — Must cover the entire surgical field
- Duration — Must encompass both the surgical and postsurgical periods
An intervention before incision is not preventive if it is incomplete or insufficient to prevent central sensitization.
Important caveat: Patients with pre-existing chronic pain and pre-established central sensitization may respond less well to preventive analgesia techniques.
Maximal benefit is achieved with complete multi-segmental blockade of noxious stimuli extended into the postoperative period, using intensive multimodal analgesic regimens.
Summary Comparison
| Feature | Preemptive Analgesia | Preventive Analgesia |
|---|---|---|
| Timing | Must be before incision | Any perioperative time |
| Focus | Timing of intervention | Intensity + duration |
| Mechanism targeted | Central sensitization from incision only | Central sensitization from incision + inflammation + postoperative period |
| Clinical evidence | Mixed/negative trials | Broader, more clinically viable |
| Status | Obsolete | Current standard |
| NMDA pathway | Implied | Explicitly targeted |
— Barash Clinical Anesthesia 9e; Miller's Anesthesia 10e; Cummings Otolaryngology
Anaesthetic management of prolapsed intervertebral disc patient
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive, textbook-sourced account of the anaesthetic management of a prolapsed intervertebral disc (PIVD) patient.
Anaesthetic Management of Prolapsed Intervertebral Disc (PIVD)
Background
Prolapse of an intervertebral disc most often occurs at L4–L5 or L5–S1 in the lumbar spine, or C5–C6 in the cervical spine. Compression may arise from disc protrusion or osteophytic bone encroaching on the spinal canal or intervertebral foramen. Surgical options include microdiscectomy, laminectomy, or spinal fusion.
1. Preoperative Assessment
Neurological evaluation:
- Document existing neurological deficits (motor weakness, sensory loss, bladder/bowel dysfunction) before surgery — this forms the baseline for postoperative comparison.
- Assess level and completeness of any neurological compromise (ASIA grading if cord involvement is suspected).
Airway assessment:
- Critical in cervical disc disease: assess neck mobility, range of motion, and any cervical instability.
- Restricted neck movement from disease, traction, or cervical collars may complicate intubation.
- Plan for video laryngoscopy or awake fiberoptic intubation if cervical instability is present; if awake intubation is planned, assess patient cooperation.
Cardiovascular and respiratory:
- High cervical lesions (C4 and above) may impair phrenic nerve function → reduced vital capacity (up to 25% loss at C4 level).
- Intercostal muscle function may be impaired by thoracic/upper cervical injuries.
- Evaluate for comorbidities: hypertension, diabetes, obesity (all increase perioperative risk).
Investigations:
- Baseline hemoglobin, coagulation profile, renal and hepatic function.
- Imaging review: MRI/CT to understand level, extent of compression, and surgical approach.
— Miller's Anesthesia 10e; Morgan & Mikhail's Clinical Anesthesiology 7e; Barash Clinical Anesthesia 9e
2. Intraoperative Management
Anaesthetic Technique
General anaesthesia (GA) is standard for most disc surgeries (discectomy, laminectomy).
- Induction: Standard IV induction (propofol + opioid).
- Airway: Endotracheal intubation is preferred, given prone positioning.
- For cervical disc disease: video laryngoscopy or awake fiberoptic intubation if cervical spine is unstable; in-line stabilisation is used if intubating after induction.
- Maintenance: Total intravenous anaesthesia (TIVA) with propofol + opioid infusion is preferred when intraoperative neurophysiological monitoring (IOM) is employed, as deep inhalational agents impair evoked potential signals.
Regional anaesthesia (spinal/epidural) may be considered for selected lumbar procedures but GA dominates in practice due to positioning requirements.
Positioning
This is one of the most critical steps in spine surgery.
- Lumbar disc surgery: Prone position (most common).
- Cervical disc surgery (anterior approach): Supine position — easier airway management but risks injury to trachea, oesophagus, recurrent laryngeal nerve, sympathetic chain, carotid artery, or jugular vein.
- Lateral decubitus may be used for some lumbar procedures.
Key concerns during prone positioning:
- Induction and intubation in supine → then carefully turned prone; neutral neck position must be maintained throughout.
- Head supported on a cushioned holder, foam headrest, or secured with pins/tongs — face must be periodically checked to ensure no pressure on eyes, nose, or ears (risk of corneal abrasion, retinal ischaemia).
- Chest rolls or a frame must allow the abdomen to hang freely — abdominal compression raises epidural venous pressure → increased blood loss and risk of haemorrhage.
- Turning prone can cause hypotension — have vasopressors and IV access ready beforehand.
- Arms: tucked at sides or extended with elbows slightly flexed (avoid excessive shoulder abduction).
Monitoring
Standard monitoring: ECG, SpO₂, ETCO₂, temperature, urine output.
Additional monitoring:
- Intra-arterial blood pressure: mandatory when major blood loss is anticipated or pre-existing cardiac disease exists. Sudden catastrophic haemorrhage from great vessel injury (thoracic/lumbar procedures) can occur.
- Intraoperative neurophysiological monitoring (IOM):
- Somatosensory Evoked Potentials (SSEPs): Monitor dorsal column (sensory) integrity.
- Motor Evoked Potentials (MEPs): Monitor anterior (motor) cord integrity.
- Both require TIVA; avoid high-dose inhalational agents and neuromuscular blockers.
- Intraoperative wake-up test (Stagnara test): Nitrous oxide/narcotic or TIVA; patient briefly awakened to test voluntary motor function after spinal distraction — increasingly replaced by continuous IOM.
Blood Conservation
Multilevel surgery, fusion, and instrumentation carry risk of significant blood loss:
- Cell salvage (intraoperative autologous blood salvage) — reduces allogeneic transfusions in non-infective, non-tumour cases.
- Tranexamic acid (antifibrinolytic) — reduces bleeding with minimal thrombotic risk.
- Deliberate hypotension — historically used but now largely abandoned due to risk of perioperative vision loss (POVL) and neurological injury.
- Coagulation parameters, Hb, and platelets should be monitored regularly.
3. Perioperative Vision Loss (POVL)
A potentially devastating complication unique to prone spine surgery:
- Causes: Posterior ischaemic optic neuropathy (most common), central retinal artery occlusion, cortical blindness.
- Risk factors: Male sex, obesity, Wilson frame use, prolonged surgery, high blood loss, prolonged head-down position, diabetes, smoking.
- Prevention: Avoid hypotension, excessive blood loss; periodic eye pressure checks; colloid use may be protective.
- High-risk patients must be counselled preoperatively about this risk (ASA Practice Advisory).
4. Postoperative Care
Pain management:
- Postoperative pain after spine surgery can be severe and challenging.
- Multimodal analgesia: NSAIDs, paracetamol, regional nerve blocks (fascial plane blocks), and opioids.
- A single intraoperative dose of methadone has been shown to reduce postoperative analgesic requirements, improve pain scores, and provide analgesia lasting months.
- Epidural analgesia may be used in selected patients.
Neurological assessment:
- Reassess motor and sensory function as soon as the patient is awake — compare to preoperative baseline.
- New deficits require urgent imaging to rule out epidural haematoma or surgical complication.
DVT prophylaxis:
- Prone position, deliberate hypotension, and immobility increase DVT/PE risk.
- Lumbar fusion carries up to 4% symptomatic DVT and 2% PE incidence.
- Anticoagulation must be balanced against risk of epidural haematoma.
- Consider IVC filter in high-risk patients where anticoagulation is contraindicated.
Airway caution post-cervical surgery:
- Airway and facial oedema can develop after prolonged prone or head-down positioning — re-intubation may be significantly more difficult than at induction.
Summary Table
| Phase | Key Actions |
|---|---|
| Preop | Neurological baseline, airway assessment (especially cervical), imaging review, comorbidity optimisation |
| Induction | Careful intubation (FOB/video laryngoscopy if cervical instability), IV induction |
| Positioning | Prone (lumbar), ensure free abdomen, eye/pressure point protection, neutral neck |
| Maintenance | TIVA preferred (for IOM), avoid deep inhalational agents + NMBs |
| Monitoring | Arterial line, SSEP + MEP if cord at risk, frequent labs |
| Blood conservation | Cell salvage, tranexamic acid, avoid deliberate hypotension |
| Postop | Neurological reassessment, multimodal analgesia, DVT prophylaxis, airway vigilance |
— Morgan & Mikhail's Clinical Anesthesiology 7e; Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e
Causes of low back pain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Here is a comprehensive, textbook-sourced account of the causes of low back pain.
Causes of Low Back Pain
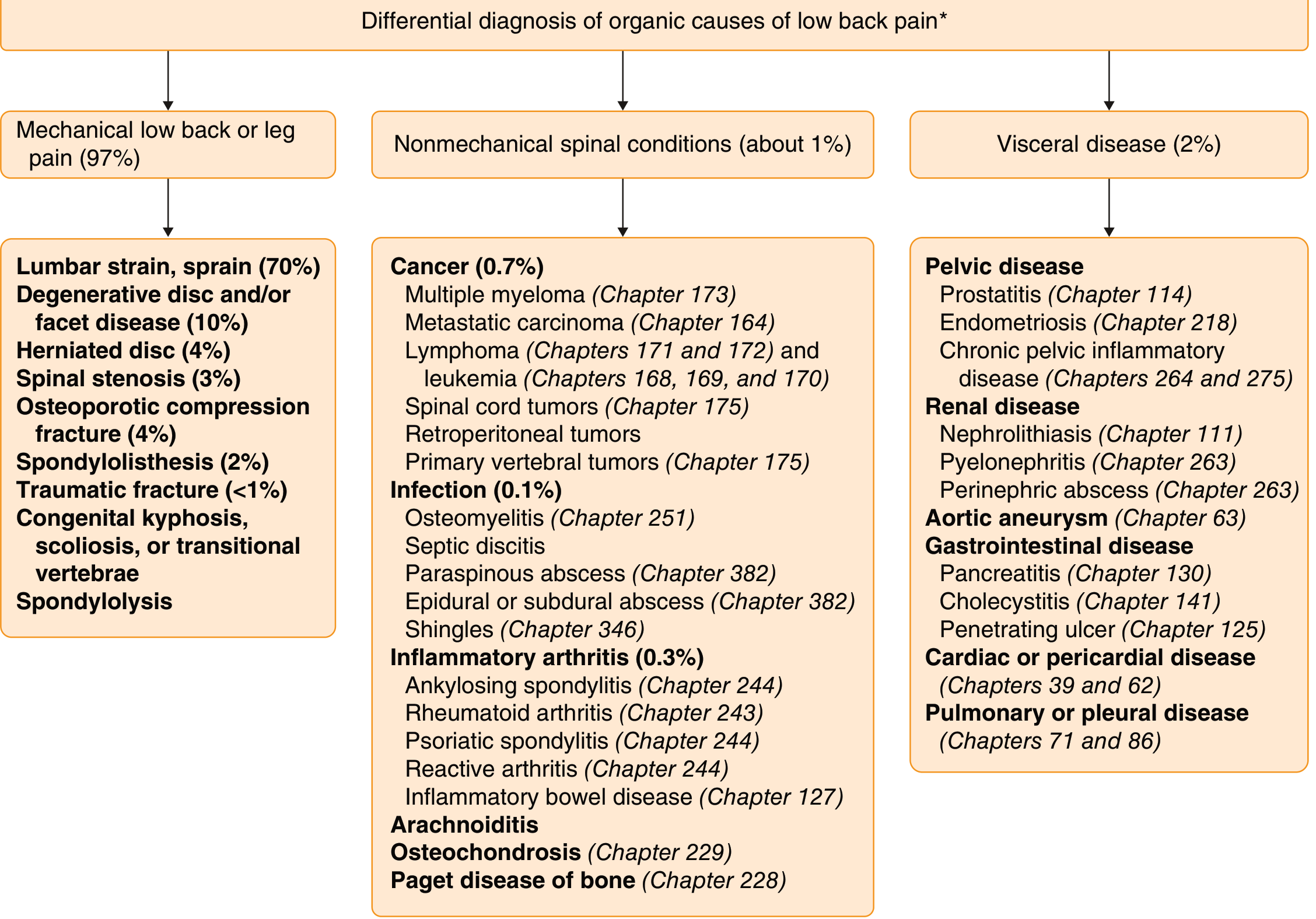
Up to 97% of low back pain is mechanical or idiopathic in origin. Only 15% of patients have a specific identifiable cause. The remaining minority have non-mechanical spinal disease or visceral referred pain.
Classification
Low back pain is broadly divided into three categories:
1. Mechanical Low Back Pain (97%)
The most common category — pain arising from structural elements of the spine.
| Cause | Approximate Frequency |
|---|---|
| Lumbar muscle strain/sprain | ~70% |
| Degenerative disc and/or facet joint disease | ~10% |
| Herniated nucleus pulposus (disc prolapse) | ~4% |
| Osteoporotic compression fracture | ~4% |
| Spinal stenosis | ~3% |
| Spondylolisthesis | ~2% |
| Traumatic fracture | <1% |
| Congenital (kyphosis, scoliosis, transitional vertebrae, spondylolysis) | Rare |
Key features of mechanical LBP:
- Worsens with activity, improves with rest
- Acute onset, often following exertion
- No systemic symptoms
Additional mechanical/neuropathic causes to consider:
- Lateral recess stenosis — from spondylotic spurs, facet hypertrophy; can cause sciatica not relieved by disc surgery
- Synovial (facet joint) cysts — may compress nerve roots in the foramen
- Tarlov cysts — perineural sheath dilatations of sacral roots
- Piriformis syndrome — entrapment of the sciatic nerve by the piriformis muscle; controversial entity
- Sacroiliac joint inflammation
- Arachnoiditis — after spine surgery or intrathecal foreign substance exposure; causes chronic back and radicular pain
2. Non-Mechanical Spinal Conditions (~1%)
These are serious causes requiring urgent evaluation.
A. Malignancy (0.7%)
- Multiple myeloma
- Metastatic carcinoma (breast, prostate, lung)
- Lymphoma / Leukaemia
- Spinal cord tumours (primary)
- Retroperitoneal tumours
- Cauda equina compression from epidural tumour deposits (prostate, breast cancer, myeloma)
- Lumbar plexus infiltration (lymphoma, neurofibrosarcoma)
B. Infection (0.1%)
- Vertebral osteomyelitis
- Septic discitis — severe back pain worsened by movement
- Paraspinous/epidural/subdural abscess
- Herpes zoster (acute radicular pain may precede the rash)
- CMV infection (in AIDS), Lyme disease (Bannwarth syndrome), neoplastic meningitis
C. Inflammatory Arthritis (0.3%)
- Ankylosing spondylitis — insidious onset, morning stiffness, night pain, responds to NSAIDs
- Psoriatic spondylitis
- Reactive arthritis
- Rheumatoid arthritis
- Inflammatory bowel disease–associated spondylitis
Key distinguishing feature: Inflammatory LBP awakens the patient from sleep; improves with exercise, worsens with rest.
D. Other Non-Mechanical Spinal Causes
- Osteochondrosis
- Paget's disease of bone
- Arachnoiditis
3. Visceral Referred Pain (~2%)
Pain referred from abdominal and pelvic organs to the back — no primary spinal pathology.
| System | Causes |
|---|---|
| Vascular | Abdominal aortic aneurysm (mid/low back, radiates to hips), aortic dissection |
| Renal | Nephrolithiasis (colicky flank/costovertebral angle), pyelonephritis, perinephric abscess |
| Gynaecological | Endometriosis, ectopic pregnancy, pelvic inflammatory disease, ovarian cyst/carcinoma |
| Gastrointestinal | Pancreatitis (L1 level), diverticulitis, cholecystitis (mid-thoracic), penetrating peptic ulcer |
| Pelvic | Prostatitis, chronic pelvic inflammatory disease |
| Cardiac/Pericardial | Rarely referred to low back |
| Pulmonary/Pleural | Pleurisy, pulmonary embolism |
4. Neurological/Other Causes
- Guillain-Barré syndrome — back and radicular pain may precede weakness
- Lumbosacral plexus neuritis (Wartenberg plexitis) — akin to brachial neuritis
- Diabetic lumbosacral radiculoplexopathy
- Sickle cell anaemia — severe pain crises involving the spine
- Catamenial sciatica — endometriosis involving the sciatic nerve, temporal with menses
- Psychogenic/depression — diffuse, emotionally described back pain; seen in 20–50% of depressed patients
Red Flags in Low Back Pain
Features requiring urgent investigation to exclude serious pathology:
| Red Flag | Possible Cause |
|---|---|
| Cauda equina syndrome (urinary retention, faecal incontinence, saddle anaesthesia) | Emergency surgical cause |
| Severe, unremitting, non-mechanical pain (worse at night, lying down) | Infection or tumour |
| Significant trauma | Fracture |
| Unexplained weight loss, fever, HIV, history of cancer | Infection or malignancy |
| IV drug use or prolonged steroid use | Infection or osteoporotic fracture |
| Widespread neurological signs | Tumour or neurological disease |
| Age >50–65 with first episode of severe back pain | Malignancy, fracture |
| Duration >6 weeks without improvement | Serious underlying cause |
— Goldman-Cecil Medicine; Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology; Grainger & Allison's Diagnostic Radiology; Textbook of Family Medicine 9e
Various modalities of pain relief for chronic pain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive, textbook-sourced overview of the modalities of pain relief for chronic pain.
Modalities of Pain Relief for Chronic Pain
Chronic pain is a disease in itself — not merely a symptom. It has biopsychosocial dimensions, and no single modality suffices. Simultaneous multimodal and multidisciplinary therapy produces better outcomes than sequential use of individual treatments.
"Simultaneous use of multiple modalities of pain management is needed for the best possible treatment outcome as opposed to using them sequentially." — Bradley & Daroff's Neurology in Clinical Practice
Overview: Multimodal Treatment Framework
| Modality | Examples |
|---|---|
| Pharmacological | NSAIDs, opioids, antidepressants, anticonvulsants, topical agents, muscle relaxants, NMDA antagonists |
| Rehabilitation | Physical therapy, occupational therapy, TENS, bracing |
| Psychological | CBT, biofeedback, relaxation therapy, support groups |
| Interventional | Epidural injections, nerve blocks, radiofrequency ablation, sympathetic blocks |
| Implantable | Spinal cord stimulation, intrathecal drug delivery pumps |
| Complementary/Alternative | Acupuncture, chiropractic manipulation, massage, craniosacral therapy |
| Surgical | Discectomy, decompression, neurolytic procedures (rarely) |
| Nutrition & Vocational | Weight loss counselling, return-to-work programmes |
1. Pharmacological Management
The WHO analgesic ladder (originally for cancer pain) guides chronic non-cancer pain management — starting with non-opioids, adding adjuvants, then stepping up to opioids only when necessary.
A. Non-Opioid Analgesics
NSAIDs (Aspirin, Ibuprofen, Naproxen, COX-2 inhibitors)
- Inhibit cyclooxygenase → reduce prostaglandin synthesis → reduce peripheral sensitisation
- Effective for nociceptive, inflammatory, and musculoskeletal pain
- Risks: GI ulceration, renal impairment, cardiovascular events, platelet inhibition
- COX-2 inhibitors (celecoxib) have better GI profile but higher cardiovascular risk
Paracetamol (Acetaminophen)
- Central and peripheral mechanisms; useful as baseline non-opioid analgesic
- Safe in low-to-moderate doses; hepatotoxic in overdose
B. Antidepressants
Used primarily for neuropathic pain — analgesic effect occurs at doses lower than required for antidepressant activity.
- Tricyclic antidepressants (TCAs): Amitriptyline, nortriptyline — first-line for neuropathic pain (diabetic neuropathy, postherpetic neuralgia). Block reuptake of norepinephrine and serotonin in descending inhibitory pathways.
- SNRIs: Duloxetine, venlafaxine — effective for diabetic neuropathy, fibromyalgia; fewer anticholinergic side effects than TCAs.
- SSRIs: Less effective for pain; used when comorbid depression is prominent.
C. Anticonvulsants
First-line for neuropathic pain, especially:
- Gabapentin, Pregabalin — bind α₂-δ subunit of voltage-gated calcium channels; reduce neuronal hyperexcitability. Effective for diabetic neuropathy, postherpetic neuralgia, fibromyalgia.
- Carbamazepine — drug of choice for trigeminal neuralgia
- Oxcarbazepine, Lamotrigine — alternatives for neuropathic pain
D. Opioid Analgesics
Reserved for moderate-to-severe pain; controversial for chronic non-malignant pain due to risks of tolerance, dependence, addiction, and opioid-induced hyperalgesia.
Classification by receptor activity:
- Full agonists (μ-receptor): Morphine, codeine, oxycodone, hydrocodone, hydromorphone, fentanyl, methadone
- Partial agonists: Buprenorphine — ceiling effect on analgesia; used in opioid use disorder
- Mixed agonist-antagonists: Pentazocine, butorphanol, nalbuphine — avoid combining with full agonists (precipitate withdrawal)
Key principles:
- Use around-the-clock dosing, not PRN, for chronic pain
- Rotate opioids when tolerance develops (equianalgesic dosing guide used)
- Monitor for constipation, sedation, respiratory depression, endocrinopathy
- Psychological dependence (drug-craving behaviour) is rare in cancer pain patients; physical dependence occurs with prolonged use
E. NMDA Receptor Antagonists
NMDA receptors mediate central sensitisation in refractory chronic pain syndromes.
- Low-dose IV ketamine — effective for CRPS type I; avoid high doses (hallucinations, psychosis)
- Methadone — dual mechanism: μ-opioid agonist + NMDA antagonist; useful for opioid-refractory pain; risk of prolonged QTc, arrhythmia
- Amantadine, Dextromethorphan, Memantine — possess some analgesic properties; insufficient evidence for routine use
F. Muscle Relaxants
- Baclofen — GABA-B agonist; useful for lancinating pain, allodynia, and trigeminal neuralgia; intrathecal baclofen enhances morphine/clonidine/SCS effects
- Benzodiazepines (Diazepam) — muscle relaxation and anxiolysis; caution with opioid co-prescription
- Tizanidine, Cyclobenzaprine (Flexeril) — newer muscle relaxants
G. Topical Agents
- Lidocaine patch (5%) — for postherpetic neuralgia, localised neuropathic pain
- Capsaicin cream/patch — depletes substance P from nociceptors; useful for localised neuropathic pain
- Topical NSAIDs — diclofenac gel for osteoarthritis
- Topical opioids — limited evidence
H. Alpha-2 Agonists
- Clonidine — modulates descending noradrenergic inhibitory pathways; useful as adjunct in neuropathic pain; available in transdermal, epidural, and intrathecal forms
2. Physical / Rehabilitation Therapies
- Physical therapy: Exercise, stretching, strengthening — cornerstone of musculoskeletal chronic pain management; reduces deconditioning and improves function
- Transcutaneous Electrical Nerve Stimulation (TENS): Activates gate-control mechanisms via stimulation of large-diameter Aβ fibres; useful for localised pain
- Occupational therapy: Adaptive strategies, ergonomics, functional rehabilitation
- Bracing/orthotics: Offloading and stabilisation for spinal and joint pain
3. Psychological Therapies
Chronic pain has significant psychological and affective dimensions; 20–50% of patients with depression have back pain.
- Cognitive Behavioural Therapy (CBT): Evidence-based; changes pain cognition, catastrophising, and maladaptive behaviours — most effective psychological intervention for chronic pain
- Biofeedback: Teaches patients to modulate physiological responses (muscle tension, heart rate) to reduce pain
- Relaxation therapy / Mindfulness-Based Stress Reduction (MBSR): Reduces central sensitisation via descending inhibitory pathway activation
- Support groups: Improve coping and reduce isolation
4. Interventional Pain Management
Minimally invasive techniques delivering medications or energy directly to pain generators.
| Procedure | Indication |
|---|---|
| Epidural corticosteroid injection | Lumbar/cervical/thoracic radiculopathy |
| Facet joint block / medial branch block | Facet joint syndrome |
| Facet rhizotomy / radiofrequency ablation | Chronic facet-mediated pain |
| Sacroiliac joint injection | SI joint pain |
| Celiac plexus block | Pancreatic cancer, chronic pancreatitis |
| Lumbar sympathetic block | CRPS of lower limbs |
| Stellate ganglion block | CRPS of arm, head/neck; headache |
| Gasserian ganglion block | Trigeminal neuralgia |
| Greater/lesser occipital nerve block | Occipital neuralgia |
| Peripheral nerve blocks | Localised neuropathic pain |
| Percutaneous disc decompression (Nucleoplasty, Disc Dekompressor) | Contained lumbar/cervical disc herniation with radiculopathy |
| Vertebroplasty / Kyphoplasty | Osteoporotic/pathological vertebral compression fracture |
| Intravenous regional block | CRPS |
| Sphenopalatine ganglion block | Headache, facial pain |
Modern interventional techniques emphasise accurate delivery of corticosteroids or local anaesthetics to suppress inflammation and block pain conduction — as opposed to old surgical ablative/destructive techniques which often caused worse deafferentation pain.
5. Implantable Therapies
Reserved for refractory chronic pain after exhausting conservative and interventional measures.
Spinal Cord Stimulation (SCS)
- Electrodes placed epidurally over the dorsal columns
- Mechanism: Gate-control theory — stimulation of large-fibre Aβ input inhibits small-fibre nociceptive transmission via spinal interneurons; also involves GABA-mediated inhibition
- Indication: CRPS, failed back surgery syndrome, peripheral vascular disease, ischaemic limb pain, postherpetic neuralgia, angina, phantom limb pain, peripheral neuropathy
- A trial stimulation is performed before permanent implantation — >50% pain relief qualifies for permanent device
Intrathecal Drug Delivery (Spinal Pump)
- Delivers morphine, bupivacaine, clonidine, or baclofen directly into CSF at much lower systemic doses
- Useful for cancer pain, CRPS, spasticity (baclofen), failed back surgery syndrome
- Advantages: Reduced systemic side effects, better dose titration
6. Complementary and Alternative Medicine (CAM)
- Acupuncture — useful adjunct for chronic musculoskeletal pain and headache; evidence supports modest benefit; may activate endogenous opioid pathways
- Chiropractic manipulation — evidence for short-term benefit in low back pain
- Massage therapy — reduces muscle tension and anxiety
- Craniosacral therapy — limited evidence
7. Surgical Treatments (Last Resort)
- Discectomy / Laminectomy / Fusion — for structural compressive pathology
- Dorsal root entry zone (DREZ) lesioning — for deafferentation pain (brachial plexus avulsion, post-herpetic neuralgia)
- Deep Brain Stimulation (DBS) — for refractory neuropathic pain
- Motor cortex stimulation — neuropathic pain refractory to all other modalities
- Historical techniques (cordotomy, rhizotomy, sympathectomy) are now rarely used due to post-deafferentation pain syndromes
Key Principles of Chronic Pain Management
- Treat comorbid psychological conditions (depression, anxiety) alongside physical pain
- Use multimodal regimens simultaneously, not sequentially
- Set realistic goals — "curing" chronic pain is often not achievable; improving function is
- Avoid opioid escalation for non-malignant pain without clear benefit
- Barriers to management: analgesic overuse/underuse, missed psychological issues, poor social support
— Bradley & Daroff's Neurology in Clinical Practice; Morgan & Mikhail's Clinical Anesthesiology 7e; Barash Clinical Anesthesia 9e
Various modalities of pain relief for chronic pain
I already answered this question in detail in my previous response. Here's a structured summary of all the modalities covered:
Modalities of Pain Relief for Chronic Pain
Chronic pain requires simultaneous multimodal, multidisciplinary therapy — not sequential use of single treatments.
1. Pharmacological
| Class | Agents | Best For |
|---|---|---|
| NSAIDs | Ibuprofen, naproxen, celecoxib | Nociceptive, inflammatory, musculoskeletal |
| Paracetamol | Acetaminophen | Baseline non-opioid analgesia |
| TCAs | Amitriptyline, nortriptyline | Neuropathic pain (first-line) |
| SNRIs | Duloxetine, venlafaxine | Diabetic neuropathy, fibromyalgia |
| Anticonvulsants | Gabapentin, pregabalin, carbamazepine | Neuropathic pain, trigeminal neuralgia |
| Opioids | Morphine, oxycodone, fentanyl, methadone | Moderate–severe; last resort in non-cancer pain |
| NMDA antagonists | Ketamine (low-dose), methadone | CRPS, central sensitisation |
| Muscle relaxants | Baclofen, tizanidine, diazepam | Spasticity, muscle spasm |
| Topical agents | Lidocaine patch, capsaicin, topical NSAIDs | Localised neuropathic/musculoskeletal pain |
| Alpha-2 agonists | Clonidine | Adjunct in neuropathic pain |
The WHO analgesic ladder guides stepwise escalation: non-opioids → adjuvants → weak opioids → strong opioids.
2. Physical / Rehabilitation
- Physical therapy — exercise, stretching, strengthening; reduces deconditioning
- TENS (Transcutaneous Electrical Nerve Stimulation) — activates gate-control mechanism via Aβ fibres
- Occupational therapy — ergonomics, functional adaptation
- Bracing / orthotics — structural offloading
3. Psychological
- Cognitive Behavioural Therapy (CBT) — most evidence-based; addresses catastrophising, maladaptive pain behaviour
- Biofeedback — self-regulation of physiological pain responses
- Mindfulness / relaxation therapy — activates descending inhibitory pathways
- Support groups — improve coping, reduce isolation
4. Interventional
| Procedure | Indication |
|---|---|
| Epidural corticosteroid injection | Radiculopathy (lumbar/cervical/thoracic) |
| Facet joint block / medial branch block | Facet joint syndrome |
| Radiofrequency ablation (rhizotomy) | Chronic facet pain |
| Sacroiliac joint injection | SI joint pain |
| Celiac plexus block | Pancreatic cancer, chronic pancreatitis |
| Lumbar sympathetic block | CRPS of lower limbs |
| Stellate ganglion block | CRPS of arm, head/neck |
| Occipital nerve block | Occipital neuralgia |
| Percutaneous disc decompression (Nucleoplasty, Disc Dekompressor) | Contained disc herniation |
| Vertebroplasty / Kyphoplasty | Vertebral compression fracture |
5. Implantable Therapies
- Spinal Cord Stimulation (SCS) — epidural dorsal column electrodes; gate-control mechanism + GABA inhibition; indicated for CRPS, failed back surgery syndrome, ischaemic limb pain, postherpetic neuralgia, angina
- Intrathecal drug delivery pump — delivers morphine, bupivacaine, clonidine, or baclofen directly into CSF; lower doses, fewer systemic side effects; used for cancer pain, CRPS, spasticity
6. Complementary & Alternative Medicine
- Acupuncture — activates endogenous opioid pathways; evidence for musculoskeletal pain and headache
- Chiropractic manipulation — short-term benefit in low back pain
- Massage therapy — reduces muscle tension and anxiety
- Craniosacral therapy — limited evidence
7. Surgical (Last Resort)
- Discectomy / Laminectomy / Fusion — structural compressive pathology
- DREZ lesioning — deafferentation pain (brachial plexus avulsion)
- Deep Brain Stimulation (DBS) — refractory neuropathic pain
- Motor cortex stimulation — neuropathic pain refractory to all other modalities
Key Principles
- Treat comorbid depression and anxiety alongside pain
- Use modalities simultaneously, not one at a time
- Goal is improved function, not necessarily complete pain elimination
- Avoid opioid escalation without clear benefit in non-malignant pain
- Address barriers: analgesic overuse/underuse, unidentified psychological issues, poor social support
— Bradley & Daroff's Neurology in Clinical Practice; Morgan & Mikhail's Clinical Anesthesiology 7e; Barash Clinical Anesthesia 9e
Define chronic pain. Explain pain pathway. Gate control theory of pain. Types of chronic pain.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
All the necessary content is now in hand. Here is the comprehensive answer.
1. Definition of Chronic Pain
The IASP defines chronic pain as pain that persists or recurs for more than 3 months.
More clinically, chronic pain is described as:
"Pain that persists beyond the usual course of an acute disease or after a reasonable time for healing to occur, typically 1 to 6 months."
Key distinctions from acute pain:
| Feature | Acute Pain | Chronic Pain |
|---|---|---|
| Role | Protective (biological) | None (disease in itself) |
| Duration | Short; resolves with healing | >3 months; outlasts tissue damage |
| Neuroendocrine response | Intact | Attenuated or absent |
| Associated features | Anxiety, tachycardia | Sleep disturbance, mood disorders, disability |
| Mechanism | Nociceptive | Nociceptive, neuropathic, or mixed |
Chronic pain is a disease in itself — it involves long-lasting, potentially permanent changes in CNS physiology, including central sensitisation, altered functional brain connectivity, and psychobiological remodelling.
— Morgan & Mikhail's Clinical Anesthesiology 7e; Cummings Otolaryngology
2. Pain Pathway
Pain is conducted along three sequential neuronal orders from the periphery to the cortex.
First-Order Neurons (Peripheral → Dorsal Horn)
- Cell bodies in the dorsal root ganglia (DRG), located in vertebral foramina at each spinal level
- Each neuron has a bifurcating axon: one end innervates peripheral tissue, the other enters the dorsal horn
- Two main fibre types carry pain:
- Aδ fibres (thinly myelinated, 15 m/s): sharp, well-localised, fast pain
- C fibres (unmyelinated, 0.5–2 m/s): dull, burning, poorly localised, slow pain
Dorsal horn laminae (Rexed):
| Lamina | Input | Function |
|---|---|---|
| I | Aδ, C | Nociception, thermoreception (Marginal layer) |
| II (Substantia gelatinosa) | C, Aδ | Key modulation site; major site of opioid action |
| V | Aβ, Aδ, C | WDR neurons — visceral + somatic convergence → referred pain |
| VII | — | Sympathetic (intermediolateral column) |
Second-Order Neurons (Dorsal Horn → Thalamus)
- Axons of second-order neurons cross the midline at the anterior commissure → ascend in the contralateral spinothalamic tract (STT) — the principal pain pathway, lying anterolaterally in the spinal cord
- The STT divides into two tracts:
| Tract | Destination | Function |
|---|---|---|
| Lateral STT (neospinothalamic) | Ventral posterolateral nucleus (VPL) of thalamus | Discriminative aspects of pain: location, intensity, duration |
| Medial STT (paleospinothalamic) | Medial thalamus | Emotional, affective, autonomic aspects of pain |
- Collateral fibres also project to:
- Periaqueductal grey (PAG) — links ascending and descending pathways
- Reticular activating system — arousal response to pain
- Hypothalamus — neuroendocrine and autonomic responses
Alternate pain pathways (explain why pain persists after cordotomy):
- Spinoreticular tract → arousal and autonomic responses
- Spinomesencephalic tract → activates antinociceptive descending pathways via PAG
- Spinohypothalamic/spinotelencephalic tracts → emotional pain behaviour
- Spinocervical tract → uncrossed, major alternative pathway
Third-Order Neurons (Thalamus → Cortex)
- Located in the thalamus → project to somatosensory cortices I and II in the postcentral gyrus of the parietal lobe
- Perception and discrete localisation of pain occur here
Descending Pain Modulation (Inhibitory Pathways)
A key mechanism explaining why pain is not proportional to injury:
Periaqueductal grey (PAG) → Raphe nuclei (serotonin) / Locus coeruleus (norepinephrine) → Dorsal horn → Suppress nociceptive transmission
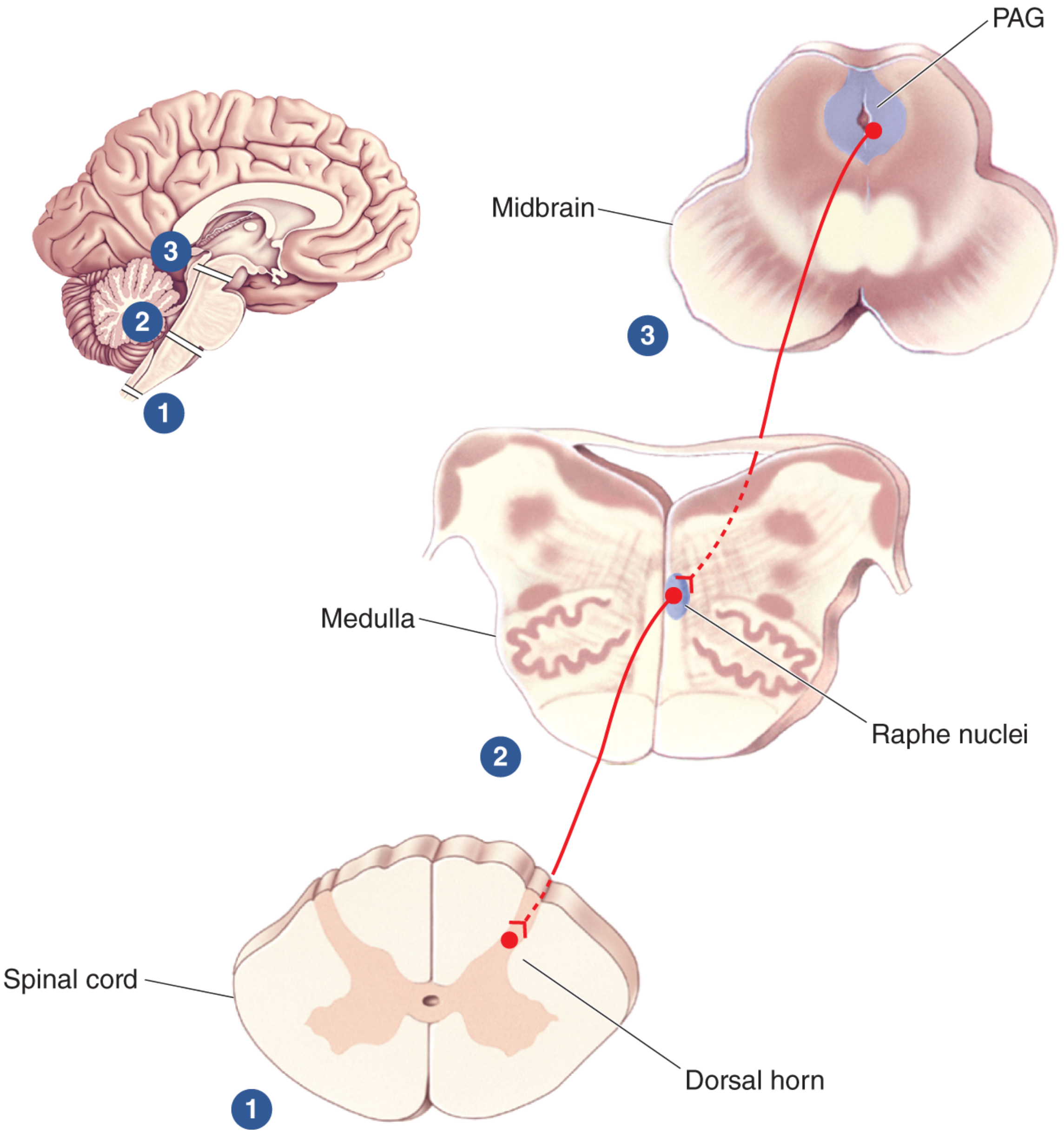
Endogenous opioids (endorphins, enkephalins, dynorphins) act at PAG, raphe nuclei, and dorsal horn → suppress glutamate release from presynaptic terminals → analgesia. Naloxone blocks these effects.
— Morgan & Mikhail's Clinical Anesthesiology 7e; Neuroscience: Exploring the Brain 5e
3. Gate Control Theory of Pain
Proposed by Melzack and Wall (1965) — a landmark concept explaining pain modulation at the spinal cord level.
Core Hypothesis
The firing of dorsal horn projection neurons (which send axons up the anterolateral tract) is determined by the balance of activity between:
- Large-diameter Aβ fibres (non-nociceptive mechanoreceptors — touch, vibration)
- Small-diameter C fibres (nociceptive)
Mechanism
| Input | Effect on Inhibitory Interneuron | Gate State | Pain Transmission |
|---|---|---|---|
| Aβ activity high (e.g., rubbing skin, TENS) | Excited (inhibitory interneuron activated) | CLOSED | Reduced — analgesia |
| C fibre activity high (nociceptive) | Inhibited | OPEN | Increased — pain felt |
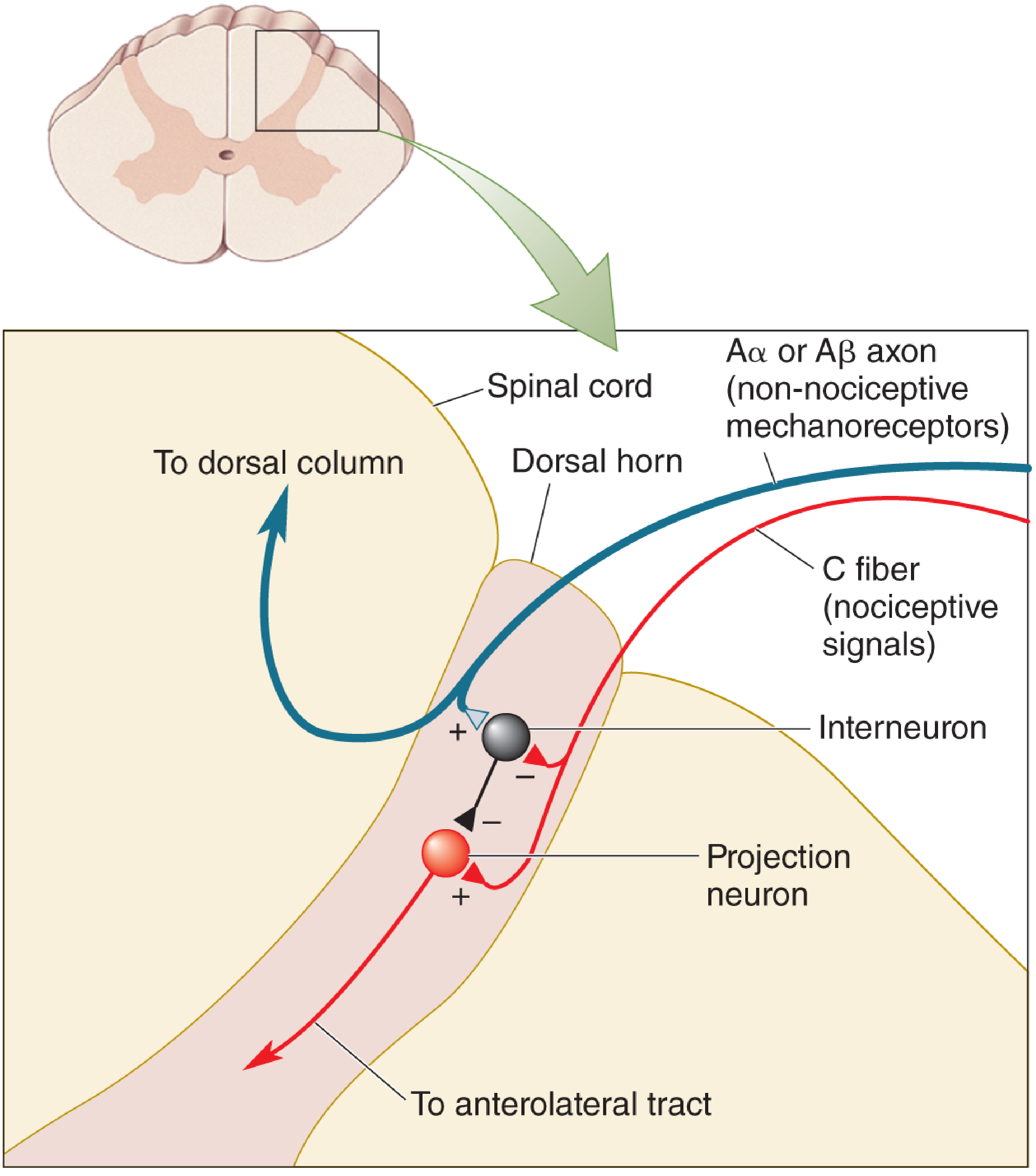
The inhibitory interneuron is excited by large Aβ fibres (closing the gate) and inhibited by C fibres (keeping the gate open). The projection neuron sends pain signals up the anterolateral tract.
Clinical Applications of Gate Control Theory
| Intervention | Mechanism |
|---|---|
| TENS | Activates large Aβ fibres → closes gate → reduces pain |
| Spinal cord stimulation (SCS) | Electrically stimulates dorsal columns (Aβ) → gate inhibition |
| Rubbing skin after injury | Aβ mechanoreceptor activation → closes gate |
| Acupuncture | May activate large-fibre afferents + endogenous opioids |
Limitations
The original gate theory was later modified — a single peripheral nerve block before incision does not always abolish pain. The theory does not fully explain all clinical neuropathic pain phenomena. Wall and Melzack themselves emphasised that descending brainstem control also regulates the gate.
— Neuroscience: Exploring the Brain 5e; Adams & Victor's Principles of Neurology 12e; Eric Kandel's Principles of Neural Science 6e
4. Types of Chronic Pain
A. Nociceptive Pain
Pain arising from activation of nociceptors in damaged tissue — transmitted via healthy, intact nerves.
Subdivisions:
| Subtype | Origin | Quality | Examples |
|---|---|---|---|
| Somatic | Skin, muscles, bones, joints, ligaments | Sharp, aching, cramping, throbbing — well localised | Arthritis, post-surgical incisional pain, bone metastasis |
| Visceral | Internal organs (thorax, abdomen) | Deep, colicky, gnawing — poorly localised; may be referred | Pancreatitis, cholecystitis, renal colic |
B. Neuropathic Pain
Pain resulting from injury, disease, or dysfunction of the nervous system itself — transmitted on damaged nerves.
Features: Burning, shooting, stabbing, electric-shock quality; allodynia, hyperalgesia, paresthesias, dysesthesias
Subtypes:
| Subtype | Mechanism | Examples |
|---|---|---|
| Peripheral neuropathic | Peripheral nerve damage | Diabetic neuropathy, postherpetic neuralgia, chemotherapy neuropathy, trigeminal neuralgia, phantom limb pain |
| Central neuropathic | CNS lesion | Stroke, spinal cord injury, multiple sclerosis |
| Deafferentation pain | Loss of sensory input + neuropathic | Phantom limb pain, brachial plexus avulsion |
| Sympathetically maintained pain | Sympathetic system dysfunction | CRPS type I & II (reflex sympathetic dystrophy / causalgia) |
C. Nociplastic Pain (Mixed/Central Sensitisation Pain)
- Pain arising from altered nociception without clear tissue damage or nerve injury
- Due to central sensitisation: amplified, prolonged CNS responsiveness
- Examples: Fibromyalgia, irritable bowel syndrome, widespread chronic low back pain
- Opioids may be less effective (opioid antagonists like low-dose naltrexone may paradoxically help)
D. Myofascial Pain
- Pain localised to muscles — often triggered by biomechanical changes
- Features: trigger points, referred pain patterns, stiffness
- Common after surgery, radiation, or prolonged immobility
E. Cancer Pain
- Often mixed — nociceptive (tumour invading tissue), neuropathic (nerve infiltration), and visceral components
- Types include breakthrough pain, incident pain, and end-of-dose failure
F. Mixed Pain
- Most chronic pain conditions involve more than one mechanism
- Examples: Chronic back pain (after surgery), cancer pain, CRPS
Summary of Types
| Type | Mechanism | Quality | Examples |
|---|---|---|---|
| Nociceptive (somatic) | Tissue damage, intact nerves | Sharp, well-localised | Arthritis, fracture |
| Nociceptive (visceral) | Organ distension/ischaemia | Colicky, referred | IBS, renal colic |
| Neuropathic | Nerve/CNS injury | Burning, electric, allodynia | Diabetic neuropathy, PHN, CRPS |
| Nociplastic | Central sensitisation | Diffuse, amplified | Fibromyalgia |
| Myofascial | Muscle dysfunction | Trigger points, referred | Post-surgical, radiation |
| Mixed | Multiple mechanisms | Variable | Cancer pain, chronic back pain |
— Morgan & Mikhail's Clinical Anesthesiology 7e; Cummings Otolaryngology; Goldman-Cecil Medicine; Bradley & Daroff's Neurology in Clinical Practice; Neuroscience: Exploring the Brain 5e
Pain pathway and gate control theory in flowchart
Here are both concepts as detailed flowcharts:
Pain Pathway (Ascending)
NOXIOUS STIMULUS
(tissue damage, thermal, mechanical, chemical)
│
▼
PERIPHERAL NOCICEPTORS
(free nerve endings in skin, muscle, viscera, periosteum)
│
├──► Aδ fibres (myelinated, 15 m/s) → FAST, sharp, well-localised pain
│
└──► C fibres (unmyelinated, 0.5–2 m/s) → SLOW, dull, burning, poorly localised
│
▼
DORSAL ROOT GANGLION (DRG)
[Cell bodies of 1st-order neurons]
│
▼
DORSAL HORN OF SPINAL CORD
[Rexed Laminae]
│
├── Lamina I & II (Substantia Gelatinosa)
│ • Aδ + C fibres terminate here
│ • Key modulation zone
│ • Major site of opioid action
│
├── Lamina V (WDR neurons)
│ • Receives both somatic + visceral input
│ • Basis of REFERRED PAIN
│
└── Modulation by interneurons, opioids,
descending pathways occurs here
│
▼
2ND-ORDER NEURON
Axon crosses midline at ANTERIOR COMMISSURE
│
▼
SPINOTHALAMIC TRACT (STT)
[Anterolateral white matter of spinal cord]
│
├──► LATERAL STT (Neospinothalamic)
│ → Ventral Posterolateral (VPL) nucleus of thalamus
│ → Discriminative pain:
│ location, intensity, duration
│
└──► MEDIAL STT (Paleospinothalamic)
→ Medial thalamus
→ Affective/emotional/autonomic
aspects of pain
│
├──► Collaterals → PERIAQUEDUCTAL GREY (PAG)
│ [Links ascending ↔ descending pathways]
│
├──► Reticular Activating System
│ [Arousal response to pain]
│
└──► Hypothalamus
[Neuroendocrine + autonomic responses]
│
▼
3RD-ORDER NEURON
[Cell bodies in thalamus]
│
▼
SOMATOSENSORY CORTEX I & II
(Postcentral gyrus, parietal lobe)
│
▼
CONSCIOUS PERCEPTION OF PAIN
(Localisation, quality, intensity)
Descending Inhibitory Pathway
EMOTIONAL STATE / STRESS / CORTEX / AMYGDALA / HYPOTHALAMUS
│
▼
PERIAQUEDUCTAL GREY (PAG) — Midbrain
│
▼
RAPHE NUCLEI (Serotonin) LOCUS COERULEUS (Norepinephrine)
[Medulla] [Pons]
│ │
└──────────────┬────────────────────┘
▼
DORSAL HORN (Spinal Cord)
Inhibits nociceptive transmission
│
▼
REDUCED PAIN PERCEPTION
(Endogenous opioids — endorphins,
enkephalins, dynorphins — act here)
Gate Control Theory (Melzack & Wall, 1965)
PERIPHERAL INPUT
│
├──────────────────────────────────────────────┐
│ │
▼ ▼
Aβ FIBRES C FIBRES
(Large-diameter, (Small-diameter,
non-nociceptive: nociceptive:
touch, vibration, pain, heat,
proprioception) tissue damage)
│ │
│ (+) EXCITES (−) INHIBITS │
▼ ▼
┌─────────────────────────────────────────────────────┐
│ INHIBITORY INTERNEURON │
│ (Substantia Gelatinosa, Lamina II) │
└───────────────────────┬─────────────────────────────┘
│
┌───────────┴────────────┐
│ │
Aβ active → interneuron (+) C active → interneuron (−)
│ │
▼ ▼
GATE CLOSED GATE OPEN
│ │
▼ ▼
Projection neuron Projection neuron
INHIBITED EXCITED
│ │
▼ ▼
NO PAIN SIGNAL PAIN SIGNAL ASCENDS
transmitted via Anterolateral Tract
│
▼
BRAIN PERCEIVES
PAIN
Gate Control — Clinical Correlation
THERAPEUTIC AIM: CLOSE THE GATE
│
├──► TENS (Transcutaneous Electrical Nerve Stimulation)
│ → Activates large Aβ fibres → excites interneuron → gate closes
│
├──► Spinal Cord Stimulation (SCS)
│ → Dorsal column (Aβ) stimulation → gate inhibition
│
├──► Rubbing injured skin
│ → Aβ mechanoreceptor activation → closes gate
│
├──► Opioids (morphine, endorphins)
│ → Act on Lamina II interneurons → directly suppress
│ projection neuron activity
│
└──► Descending inhibitory pathways (PAG activation)
→ Serotonin + norepinephrine suppress dorsal horn
→ Functionally equivalent to "closing the gate"
from above
Key Summary
| Element | Role |
|---|---|
| Aβ fibres | Close the gate (inhibit pain) |
| C fibres | Open the gate (facilitate pain) |
| Inhibitory interneuron (SG) | The "gate" itself |
| Projection neuron | Transmits pain up the STT |
| Descending PAG pathway | Supraspinal gate control |
| Opioids / endorphins | Directly act on gate at lamina II |
— Neuroscience: Exploring the Brain 5e (Melzack & Wall, 1965); Morgan & Mikhail's Clinical Anesthesiology 7e; Adams & Victor's Principles of Neurology 12e
Crps
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive account of Complex Regional Pain Syndrome (CRPS) from authoritative textbooks.
Complex Regional Pain Syndrome (CRPS)
Historical Terminology
| Old Term | Corresponds To |
|---|---|
| Causalgia (Weir Mitchell, 1870s) | CRPS II |
| Reflex Sympathetic Dystrophy (RSD) (Evans, 1946) | CRPS I |
| Sudeck atrophy, shoulder-hand syndrome, algodystrophy | All now under CRPS I |
In 1994, the IASP replaced all these terms with Complex Regional Pain Syndrome (CRPS).
Definition & Classification
CRPS is a neuropathic pain disorder characterised by regional pain and sensory changes following a noxious event, with prominent autonomic, trophic, and motor features disproportionate to the inciting injury.
| Type | Former Name | Key Feature |
|---|---|---|
| CRPS I | Reflex Sympathetic Dystrophy (RSD) | No definable nerve lesion |
| CRPS II | Causalgia | Definable peripheral nerve injury present |
Both types share identical clinical features — the distinction is purely based on the presence or absence of an identifiable nerve injury.
CRPS is now considered nociplastic in nature (caused by ongoing inflammation and central sensitisation), rather than purely neuropathic.
Epidemiology
- Mean age of onset: 36–46 years
- Women predominate (60–81% of cases)
- Precipitating events:
- Fracture: 16–46%
- Sprain/strain: 10–29%
- Post-surgery: 3–24%
- Contusion/crush: 8–18%
- Myocardial infarction: ~12% (shoulder-hand syndrome)
Pathophysiology
The exact mechanism remains unclear. Multiple theories exist:
- Sympathetic-afferent coupling — abnormal cross-excitation between efferent sympathetic fibres and somatic afferent pain fibres at the nerve terminal (chemical, not electrical); circulating catecholamines trigger abnormal adrenergic sensitivity in injured nociceptors
- Central sensitisation — sustained peripheral pain bombardment sensitises dorsal horn neurons; NMDA receptor activation, COX/prostaglandin induction, and reduced GABAergic inhibition all implicated
- Autonomic dysregulation — decreased sympathetic outflow to the affected limb; the vasomotor/sudomotor changes are due to catecholamine hypersensitivity, not sympathetic overactivity
- Inflammatory mechanisms — ongoing tissue inflammation with neurogenic inflammation (substance P, CGRP release) drives peripheral sensitisation
- Cortical reorganisation — altered somatosensory cortex representation of the affected limb
Clinical Features
Cardinal Feature: Excruciating, disproportionate pain
- Burning, aching, pricking, or shooting in quality
- Not limited to the territory of one nerve or to the area of injury
- Severity disproportionate to the original injury
Sensory Abnormalities
- Hyperalgesia — exaggerated response to minor stimuli (e.g., safety-pin prick)
- Mechanical allodynia — light touch causes severe, prolonged pain
- Thermal allodynia — cold stimulus (e.g., alcohol drop) perceived as painful
- Decreased temperature and pinprick sensation in affected limb
Autonomic (Vasomotor/Sudomotor) Features
- Skin colour changes: reddish → blue/purple/pale (fluctuates over minutes to hours)
- Livedo reticularis — non-blanchable reticulated pattern on skin
- Temperature asymmetry >1°C between affected and unaffected limb
- Hyperhidrosis — excessive sweating in ~60% of patients
Oedema
- Early: mild, may mimic cellulitis
- Late: severe — DVT must be excluded by Doppler
Motor Dysfunction
- Weakness, tremor, dystonia
- Joint contractures
- Causalgia-dystonia syndrome — fixed dystonic posture engrafted on causalgic pain
Trophic Changes (Late)
- Shiny, smooth, hairless, discoloured skin
- Poor nail growth; brittle, ridged nails
- Muscle and bone atrophy
- Severe demineralisation on X-ray
Clinical Images


Stages of Progression (Schwartzman & Maleki)
| Stage | Timing | Features |
|---|---|---|
| Stage I (Acute) | 0–3 months | Burning pain, minor oedema, increased skin temperature, vasomotor changes; one limb |
| Stage II (Dystrophic) | 3–6 months | Progressive soft tissue oedema, thickened skin and articular tissues, muscle wasting |
| Stage III (Atrophic) | >6 months | Limited movement, frozen joint (e.g., frozen shoulder), contractures, waxy/trophic skin, brittle nails, severe bone demineralisation; may involve 4 limbs |
Diagnosis
CRPS is a clinical diagnosis — no single test is diagnostic.
Budapest Criteria (IASP, high sensitivity and specificity when applied):
Must have:
- Continuing pain disproportionate to inciting event
- At least one symptom in 3 of 4 categories
- At least one sign in 2 of 4 categories at time of evaluation
- No other diagnosis that better explains the findings
Four categories:
| Category | Symptoms | Signs |
|---|---|---|
| Sensory | Hyperaesthesia, allodynia | Hyperalgesia to pin-prick, allodynia |
| Vasomotor | Temperature asymmetry, colour changes | Temperature asymmetry >1°C, colour change |
| Sudomotor/Oedema | Oedema, sweating changes | Oedema, sudomotor asymmetry |
| Motor/Trophic | Reduced ROM, weakness, dystonia | Weakness, tremor, dystonia, trophic changes |
Ancillary investigations:
- Autonomic testing: resting sweat output + quantitative sudomotor axon reflex test (QSART) — 94% sensitive, 98% specific; excellent predictor of response to sympathetic block
- Bone scan: increased uptake in affected region
- X-ray/MRI: demineralisation, periarticular osteoporosis
- Thermography: skin temperature asymmetry
Treatment
Management is multimodal — no single treatment is uniformly effective.
A. Pharmacological
| Drug | Mechanism / Use |
|---|---|
| Gabapentin / Pregabalin | α₂-δ calcium channel — first-line neuropathic pain |
| TCAs (amitriptyline) | Descending inhibition; neuropathic pain |
| NSAIDs | Inflammatory component |
| Memantine | NMDA antagonist |
| Alendronate / Bisphosphonates | Prevent bone resorption; analgesic effect (oral or IV) |
| Calcitonin | IM or SC; bone pain |
| Ketamine infusion | Low-dose IV — 4–5 day infusion (1–7 μg/kg/min) or 4h daily for 10 days (0.35 mg/kg/hr); monitor liver enzymes |
| Prazosin, propranolol, nifedipine | Sympatholytic/vasodilatory |
| Guanethidine / Phenoxybenzamine | Adrenergic blockade |
| Corticosteroids | Early inflammatory stage |
| Low-dose naltrexone | Emerging evidence for nociplastic component |
B. Interventional
| Procedure | Details |
|---|---|
| Sympathetic nerve blocks | First-line interventional treatment — stellate ganglion block (upper limb), lumbar sympathetic block (lower limb); provides short-term relief facilitating PT; repeat if >50% relief from first block |
| IV regional block (Bier block) | Guanethidine or bretylium IV via isolated limb — sympatholytic effect |
| Phenol neurolysis of lumbar sympathetic ganglia | As effective as thermal radiofrequency ablation |
| Botulinum toxin A (76 IU) into L2-L3 sympathetic ganglia | Greater temperature increase and pain reduction vs local anaesthetic |
| Intravenous ketamine | For refractory CRPS (infusion protocol) |
| IV bisphosphonates | IV pamidronate or zoledronate |
Note: degree of temperature increase after sympathetic block does not correlate with amount of pain relief — correlates with magnitude of sympathetic block.
C. Implantable Therapies
- Spinal Cord Stimulation (SCS) — indicated when other treatments fail; proven efficacy for CRPS; trial stimulation first; delivers dorsal column stimulation to close the gate and activate inhibitory circuits
- Intrathecal drug delivery — morphine + clonidine intrathecally for refractory cases
D. Physical Therapy
- Essential — SMP blocks are intended to facilitate PT, not replace it
- Desensitisation, graded motor imagery, mirror therapy, progressive loading
- Early mobilisation prevents contractures and atrophy
E. Surgical
- Sympathectomy — reserved for progressive disease that has previously responded to sympathetic blocks; provides longer-lasting relief than repeated blocks
- Surgical ablation techniques largely avoided (risk of deafferentation pain)
F. Psychological
- CBT, biofeedback, relaxation therapy — important given high rates of depression and anxiety in CRPS
Summary
PRECIPITATING INJURY (fracture, surgery, sprain, MI)
↓
Abnormal peripheral sensitisation
+ Sympathetic-afferent coupling
+ Central sensitisation (NMDA, CRPS)
↓
CRPS I (no nerve lesion) / CRPS II (nerve lesion)
↓
Cardinal features:
Burning pain (disproportionate) + Allodynia + Hyperalgesia
+ Vasomotor changes + Oedema + Sudomotor + Trophic
↓
Progresses Stage I → II → III
(Acute → Dystrophic → Atrophic)
↓
DIAGNOSIS: Budapest Criteria (clinical)
+ QSART / Bone scan / Thermography
↓
TREATMENT: Multimodal
Gabapentin + PT + Sympathetic blocks
→ IV Ketamine / Bisphosphonates
→ SCS if refractory
— Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology 12e; Barash Clinical Anesthesia 9e; Morgan & Mikhail's Clinical Anesthesiology 7e
VAPORIZERS-PRINCIPLES, CLASSIFICATION, SAFETY FEATURES
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
AWARENESS UNDER ANESTHESIA. DEPTH OF ANESTHESIA MONITORING
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.