Give me details about procedure and approaches of hip aspiration
Reading File
Finding Sources
Finding Sources
Searching the Web
hip aspiration procedure approaches technique clinical
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Campbell's Operative Orthopaedics and Tintinalli's Emergency Medicine. Here is the full detailed answer:
Hip Aspiration (Arthrocentesis of the Hip Joint)
Hip aspiration (hip arthrocentesis) is the needle puncture of the hip joint to withdraw synovial fluid for diagnostic or therapeutic purposes. The hip is a deeply seated joint surrounded by thick soft tissues, making it more technically demanding than knee or shoulder aspiration.
Indications
- Suspected septic arthritis (most urgent indication)
- Diagnosis of periprosthetic joint infection (aspiration is warranted when ESR, CRP, or synovial WBC are elevated)
- Evaluation for crystal arthropathy (gout, pseudogout)
- Diagnosis of transient synovitis in children
- Hip arthrogram (after reduction of DDH, or in Legg-Calvé-Perthes disease)
- Therapeutic drainage of a painful effusion
- Gunshot injuries to the hip - aspiration followed by arthrogram is the best test to detect joint penetration
Campbell's Operative Orthopaedics 15th Ed, p. 1031; Tintinalli's Emergency Medicine, p. 1964
General Principles
- The hip can be aspirated via a lateral, anterior, or medial approach
- Image guidance (fluoroscopy or ultrasound) is strongly recommended to confirm needle placement - if fluid cannot be aspirated, an arthrogram should be performed to verify position
- Even when purulence cannot be aspirated, septic arthritis may still be present; open drainage should be considered if local and systemic symptoms persist
- An 18-gauge spinal needle (long) is standard; a 3-5 mL syringe is attached
- Do NOT dilute samples with saline or water - this kills bacteria, leading to false-negative cultures
Campbell's Operative Orthopaedics 15th Ed, p. 1030
Approaches
1. Lateral Approach (Technique 24.9)
Patient position: Supine, hip slightly internally rotated, greater trochanter prominent.
Steps:
- Insert the needle just inferior and anterior to the greater trochanter, at a 45-degree angle to the surface of the thigh
- Advance the needle medially and proximally, close to bone, for 5-10 cm (depending on patient size) until the joint is entered
Advantage: The bone (femoral neck) prevents the needle from going in too steeply; avoids overlying pannus in obese patients.
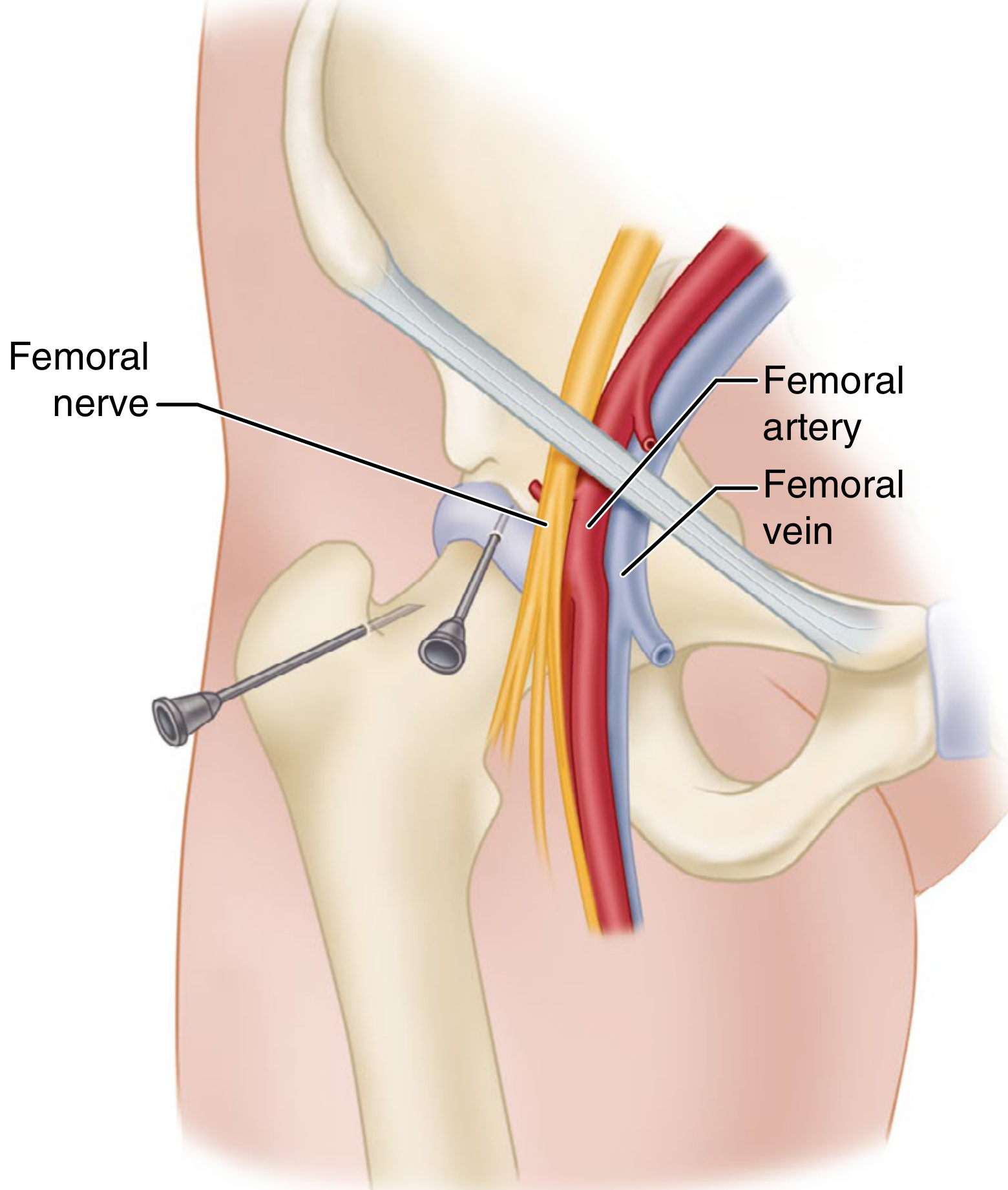
FIGURE 24.7 - Aspiration of hip, lateral and anterior approaches (Campbell's)
2. Anterior Approach (Technique 24.10)
Patient position: Supine.
Landmark: Femoral artery pulse, palpated in line with the inguinal ligament.
Steps:
- Palpate the femoral artery at the level of the inguinal ligament
- Insert the needle 2.5 cm lateral and 2.5 cm distal to the femoral artery pulse, at a 45-degree angle to the skin surface
- Advance 5-7.5 cm medially and proximally into the joint
Key hazard: The femoral neurovascular bundle runs medially - always insert the needle lateral to the femoral artery.
Campbell's Operative Orthopaedics 15th Ed, p. 1030
Tintinalli's note: The anterior approach is one of two standard approaches for emergency hip arthrocentesis. US-guided arthrocentesis by an emergency physician or radiologist is acceptable when local training is in place.
Tintinalli's Emergency Medicine, p. 1964
3. Medial Approach (Technique 24.11)
Patient position: Hip flexed and abducted - this is often a more comfortable position for patients with septic arthritis.
Steps:
- Flex and abduct the leg
- Place the needle inferior to the adductor longus tendon
- Using image intensification, advance the needle in a plane below the palpated femoral artery until the femoral head or neck is reached
- Aspirate the joint
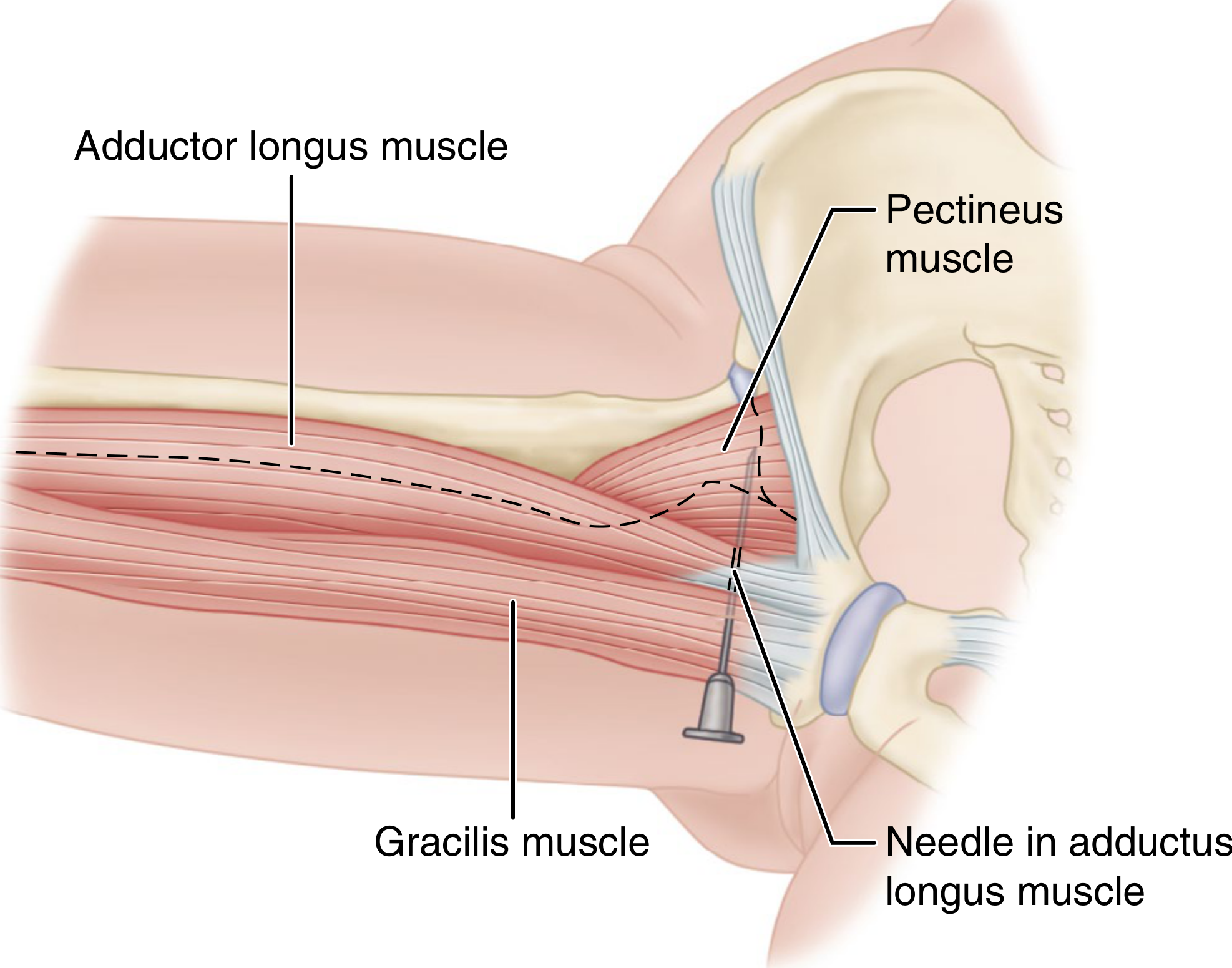
FIGURE 24.8 - Aspiration of hip, medial approach (Campbell's)
4. Ultrasound-Guided Approach (Preferred in Emergency Settings)
The US-guided anterior approach targets the anterior synovial recess between the femoral neck and femoral head cortex.
Steps:
- Place the patient supine, hip slightly internally rotated
- Use a curvilinear probe to identify the femoral head-neck junction and any hypoechoic effusion in the anterior synovial recess
- Use color Doppler to avoid vessels
- Infiltrate local anesthetic with a 25-gauge needle to create a track
- Insert an 18-gauge spinal needle in-plane (long axis) under direct US visualization, distal to proximal
- Maintain negative pressure; aspirate all visible fluid
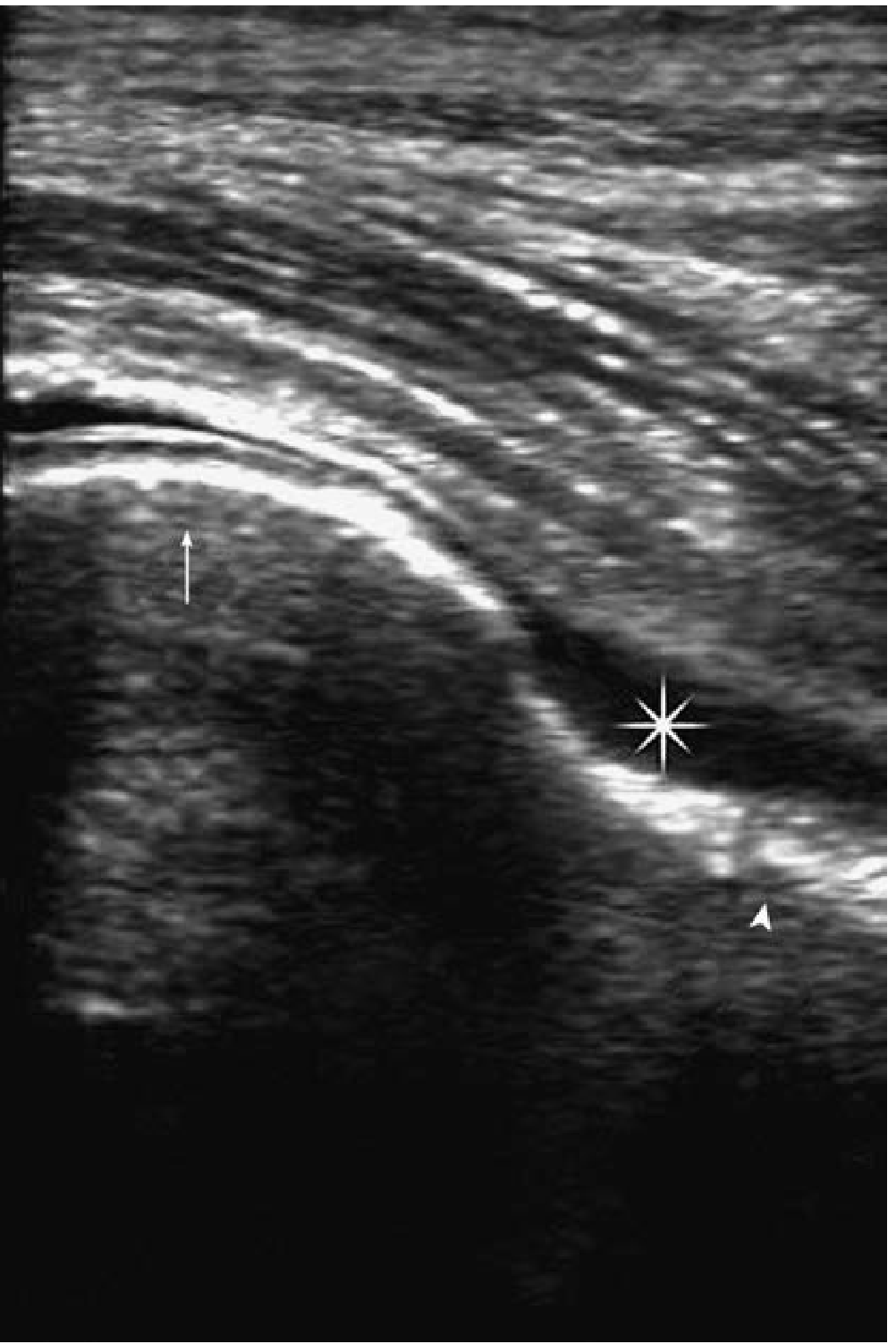
FIGURE 284-5 - US image of a hip effusion, Tintinalli's Emergency Medicine, p. 1964
US guidance improves accuracy, and adding joint lavage to native fluid collection may improve sensitivity/specificity for diagnosing prosthetic joint infection.
Comparison of Approaches
| Approach | Entry Point | Needle Direction | Position | Notes |
|---|---|---|---|---|
| Lateral | Inferior/anterior to greater trochanter | 45° medially and proximally | Supine | Bone guides depth; avoids medial vessels |
| Anterior | 2.5 cm lateral + 2.5 cm distal to femoral artery | 45° medially and proximally | Supine | Must stay lateral to femoral vessels |
| Medial | Inferior to adductor longus tendon | Below femoral artery toward femoral head | Flexed, abducted | Comfortable for septic patients; image guidance essential |
| US-guided anterior | Anterior synovial recess | In-plane, distal to proximal | Supine, internal rotation | Preferred in emergency settings |
Fluid Analysis After Aspiration
| Test | Purpose |
|---|---|
| Gram stain and culture | Identify infectious organisms |
| WBC count and differential | Septic arthritis: typically >50,000 cells/mL |
| Crystal analysis | Gout, CPPD |
| Glucose/protein | Supplemental markers |
- Do NOT place fluid in water - use universal culture media directly
- In total hip arthroplasty patients, about 1/3 of aspirations are "dry" - cultures may be less reliable in such cases; repeat aspiration or lavage should be considered
Special Considerations
Children: The anterior approach is preferred in small children because it:
- Avoids damage to the primary blood supply to the femoral head
- Reduces chance of postoperative dislocation
- Has more evident landmarks
Adults: The posterior approach allows dependent drainage and is more familiar to most orthopaedic surgeons (used for open drainage, not needle aspiration alone).
Periprosthetic infection: Hip aspiration is warranted when any of the three screening lab values (ESR, CRP, synovial WBC) are elevated in a patient with a total hip arthroplasty.
Campbell's Operative Orthopaedics 15th Ed, p. 1030-1031
This is a shared conversation. Sign in to Orris to start your own chat.