Peptic ulcer disease symptomatology with differentiation in gastric and duodenal ulcer along treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to deliver a thorough, well-cited answer. Here it is:
Peptic Ulcer Disease: Symptomatology, Differentiation, and Treatment
1. Overview
Peptic ulcer disease (PUD) refers to mucosal defects in the stomach (gastric ulcer, GU) or the proximal duodenum (duodenal ulcer, DU) caused by an imbalance between aggressive factors (acid, pepsin, H. pylori, NSAIDs) and mucosal defense mechanisms. The two principal etiologies are Helicobacter pylori infection and NSAID/aspirin use.
2. General Symptomatology
More than 90% of patients with PUD complain of abdominal pain. The pain is characteristically:
- Nonradiating
- Burning or gnawing in quality
- Epigastric in location (61–86% of duodenal ulcers; ~67% of gastric ulcers)
Other accompanying symptoms include:
- Nausea
- Bloating / early satiety
- Weight loss
- Vomiting (especially in complicated disease with obstruction)
- Heartburn or acid regurgitation
A history of prior PUD, regular NSAID/aspirin use, or self-treatment with over-the-counter antacids is suggestive of the diagnosis.
Clinical caveat: It is not reliably possible to diagnose peptic ulceration by history alone, nor to distinguish DU from GU or functional dyspepsia based on symptoms. The positive likelihood ratio of clinical diagnosis of PUD is only about 2.2. The most predictive physical sign is the "pointing sign" — when asked to indicate the location of pain, the patient points to a discrete epigastric site, which is moderately predictive of DU. — Yamada's Textbook of Gastroenterology, 7th ed.
3. Differentiation: Gastric vs. Duodenal Ulcer
| Feature | Gastric Ulcer (GU) | Duodenal Ulcer (DU) |
|---|---|---|
| Pain timing | Occurs with or shortly after eating | Occurs 2–3 hours after a meal; classically late postprandial |
| Nocturnal pain | Less common | Common — two-thirds of DU patients have pain awakening them from sleep |
| Food effect | Food worsens or does not relieve pain (~40% increased by food) | Food relieves pain (acid buffering); ~50% relief with food |
| Antacid relief | Present but inconsistent | Typically more dramatic relief |
| Weight change | May have weight loss (pain with eating causes food avoidance) | Often weight gain (eating relieves pain, so patients eat more) |
| Nausea / vomiting | More common | Less common in uncomplicated disease |
| Acid secretion | Usually normal or decreased | Usually increased (acid hypersecretion) |
| Malignancy risk | Must be excluded — biopsy mandatory | Very rarely malignant |
| H. pylori association | ~70–80% | ~90–95% |
Quantitative symptom data from Yamada's (Table 49.3):
| Symptom | GU (%) | DU (%) | Functional dyspepsia (%) |
|---|---|---|---|
| Epigastric pain | 67 | 61–86 | 52–73 |
| Within 30 min of food | 20 | 5 | 32 |
| Increased by food | ~40 | ~18 | ~35 |
| Relieved by food | ~25 | ~50 | ~28 |
| Nocturnal pain | ~35 | ~50–64 | ~25 |
| Frequently severe | 68 | 53 | 37 |
— Yamada's Textbook of Gastroenterology, 7th ed.
4. Gastric Ulcer Classification (Johnson/Modified)
The modified Johnson classification stratifies gastric ulcers by location and mechanism:
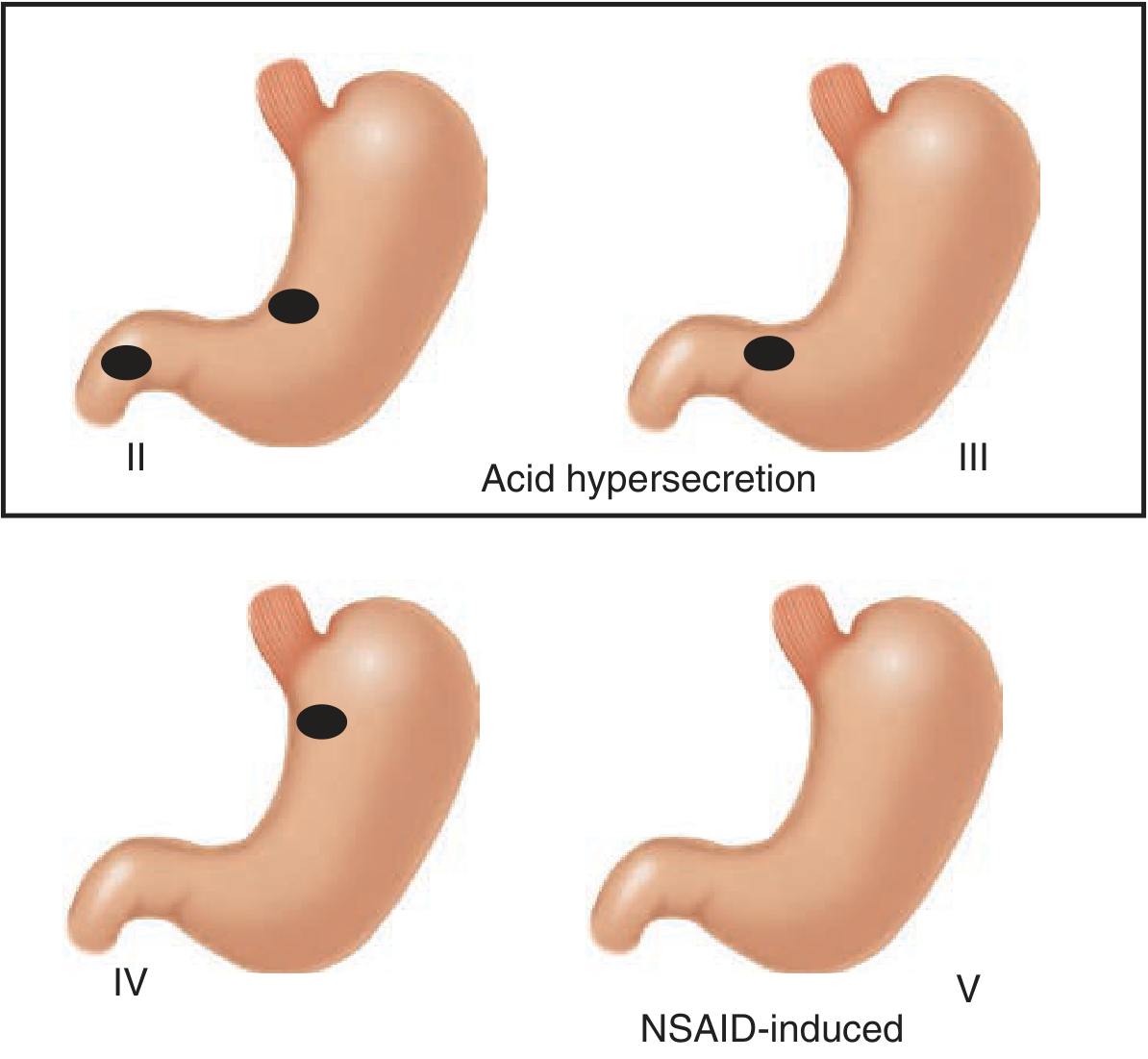
- Type I — Lesser curve at incisura (most common; normal/low acid)
- Type II — Gastric body + concurrent DU (acid hypersecretion)
- Type III — Prepyloric (acid hypersecretion, behaves like DU)
- Type IV — High on lesser curve near GEJ (low acid)
- Type V — Anywhere in stomach; NSAID-induced
— Schwartz's Principles of Surgery, 11th ed.
5. Complications
Complications arise in a minority of patients but carry significant morbidity:
| Complication | Key Features |
|---|---|
| Bleeding | Most common complication; presents as hematemesis, melena, or hematochezia. Posterior DU erodes into the gastroduodenal artery; lesser curve GU erodes the left gastric artery |
| Perforation | Sudden onset of excruciating abdominal pain; peritoneal signs; free air on upright CXR in ~80% |
| Gastric outlet obstruction | ≤5% of PUD; from DU or prepyloric ulcer; nonbilious vomiting, succussion splash, hypokalemic hypochloremic metabolic alkalosis |
| Intractable/nonhealing ulcer | Failure to heal after adequate therapy; consider malignancy, Zollinger-Ellison syndrome |
6. Diagnosis
- Endoscopy (EGD) is the gold standard — most sensitive and specific; allows biopsy for H. pylori and histology (malignancy exclusion in GU)
- Barium contrast studies — still used when endoscopy is contraindicated; barium filling a crater is diagnostic
- CT scan — much less sensitive; can show perforation, not first-line for diagnosis
- H. pylori testing: urea breath test, stool antigen, or biopsy-based (rapid urease test, histology, culture)
7. Treatment
7.1 Medical Treatment
PPIs are the cornerstone of therapy — they irreversibly bind proton pumps in parietal cell secretory canaliculi, suppressing acid more durably and effectively than H₂-receptor antagonists. PPIs heal a greater proportion of ulcers more rapidly.
| Drug Class | Examples | Role |
|---|---|---|
| Proton pump inhibitors (PPIs) | Omeprazole, lansoprazole, esomeprazole, pantoprazole | First-line; active ulcer healing and maintenance |
| H₂-receptor antagonists (H₂-RAs) | Ranitidine, famotidine | Second-line; still effective; replaced largely by PPIs |
| Sucralfate | — | Acts locally on mucosal defects; useful supplement to acid suppression |
| Antacids | — | Symptomatic relief only |
| Misoprostol | — | PGE₁ analogue; gastroprotection in NSAID users |
General principles:
- Stop NSAIDs, aspirin, smoking, and alcohol
- Patients requiring NSAIDs/aspirin must receive concomitant PPIs
- Acid suppression can typically be stopped after 3 months if the ulcerogenic stimulus is removed
- Long-term PPI maintenance is indicated for: patients hospitalized with ulcer complications, elderly/debilitated NSAID users, anticoagulated patients, recurrent bleeders
7.2 H. pylori Eradication
Testing and treatment of H. pylori is mandatory — eradication dramatically reduces ulcer recurrence.
Standard regimens:
| Regimen | Components | Duration |
|---|---|---|
| Standard triple therapy | PPI + clarithromycin + amoxicillin (or metronidazole) | 10–14 days |
| Bismuth quadruple therapy | PPI + bismuth + metronidazole + tetracycline | 10–14 days; used in clarithromycin-resistant areas |
| Concomitant therapy | PPI + clarithromycin + amoxicillin + metronidazole | 10–14 days |
| Sequential therapy | PPI + amoxicillin × 5 days → PPI + clarithromycin + tinidazole × 5 days | 10 days total |
If initial testing is negative but ulcer symptoms persist, an empirical anti-H. pylori trial is reasonable given the rate of false-negative tests. Confirm eradication at ≥4 weeks post-treatment (urea breath test or stool antigen).
7.3 Surgical Treatment
Surgery is reserved for complications (bleeding uncontrolled endoscopically, perforation, obstruction) or truly intractable/nonhealing ulcers:
- Bleeding DU: Oversewing of the bleeding vessel ± vagotomy/pyloroplasty
- Perforated DU: Omental patch (Graham patch) ± definitive acid-reducing procedure
- Perforated GU: Excision + closure, or partial gastrectomy
- Outlet obstruction: Balloon dilation (endoscopic) or surgical bypass/resection; malignancy must be excluded
- Acid-reducing procedures: Truncal vagotomy + pyloroplasty, highly selective vagotomy, or Billroth I/II gastrectomy
Planned surgery under controlled circumstances yields better outcomes than emergent surgery. Deep bleeding ulcers on the posterior duodenal bulb or lesser gastric curvature often erode large arteries less amenable to endoscopic treatment, warranting early operative consideration.
— Schwartz's Principles of Surgery, 11th ed.
Key Takeaways
- DU — pain 2–3 hours postprandially + nocturnal; food relieves; acid hypersecretion; strongly H. pylori associated
- GU — pain with eating; food worsens or does not help; weight loss; biopsy mandatory to exclude malignancy
- Neither type can be reliably differentiated from functional dyspepsia by symptoms alone — endoscopy is required for definitive diagnosis
- PPIs + H. pylori eradication are the foundation of medical treatment; surgery is for complications or refractory cases
This is a shared conversation. Sign in to Orris to start your own chat.