Can you teach me ssri…aa in everything, history, psychopharmacology,psychodynamics,kinetics, indications, guidelines, titration, switching, side effects, recent advances, contraindications, toxicity, discontinuation,dosage,formulation,evidence based trials,…and teach each drug individually too
"selective serotonin reuptake inhibitors"[MeSH Terms] AND "antidepressive agents"[MeSH Terms]
SSRI antidepressants 2024 2025 clinical guidelines prescribing evidence-based advances
Selective Serotonin Reuptake Inhibitors (SSRIs) — Complete Teaching Guide
PART 1 — HISTORY
| Drug | Brand | FDA Approval |
|---|---|---|
| Fluoxetine | Prozac | 1987 |
| Sertraline | Zoloft | 1991 |
| Paroxetine | Paxil | 1992 |
| Fluvoxamine | Luvox | 1994 |
| Citalopram | Celexa | 1998 |
| Escitalopram | Lexapro | 2002 |
PART 2 — PSYCHOPHARMACOLOGY & MECHANISM OF ACTION
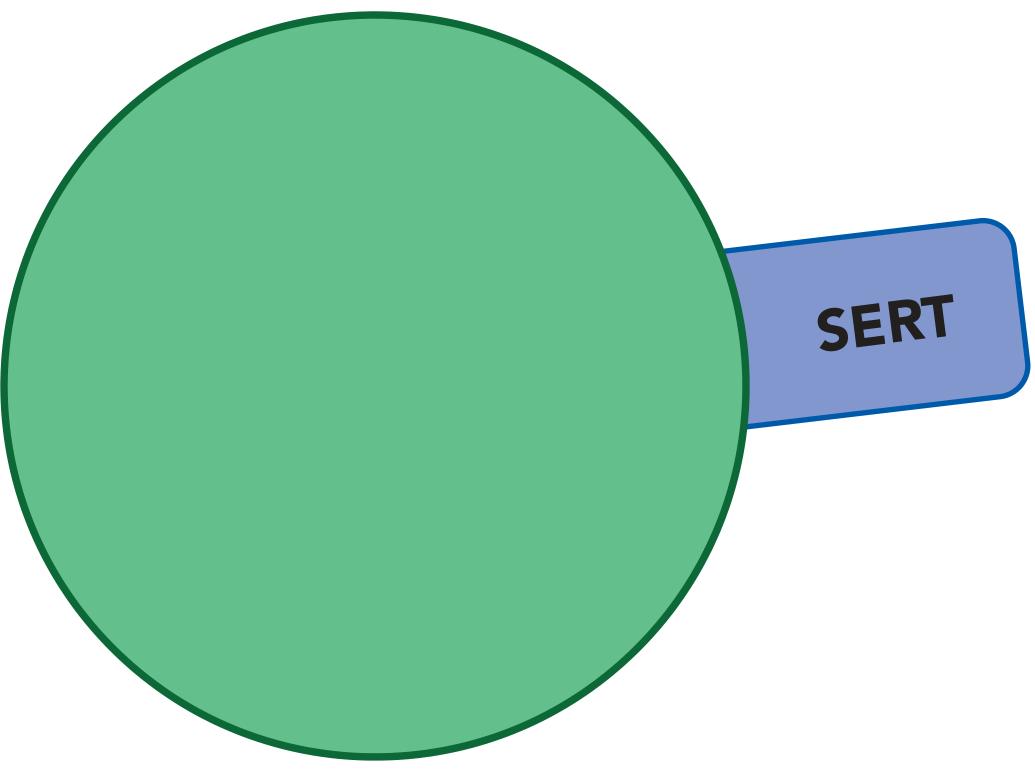
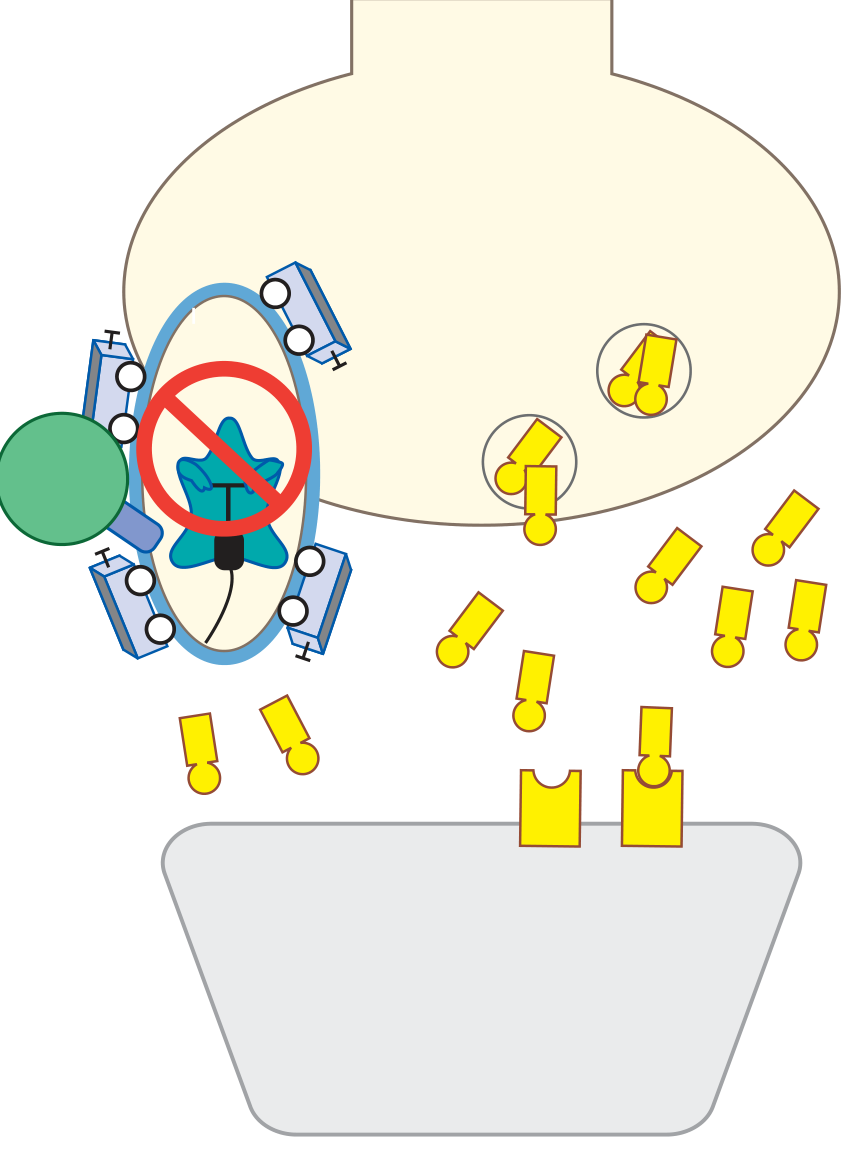
The Core Mechanism: SERT Inhibition
The Five-Step Mechanism of Action (Stahl)
-
Acute (hours): SSRI blocks SERT → serotonin accumulates at axon terminals AND at somatodendritic areas near the cell body. The cell body area has 5-HT1A autoreceptors that act as a brake — high local 5-HT activates them and inhibits neuronal firing.
-
Early (days): Because 5-HT1A autoreceptors are being continuously stimulated by elevated 5-HT, they begin to desensitize (downregulate). The brakes start releasing.
-
Intermediate (1–2 weeks): As somatodendritic 5-HT1A autoreceptors downregulate, the inhibition on neuronal firing lifts → impulse flow resumes normally.
-
Delayed (2–4 weeks): With normal impulse flow restored, serotonin is now released at axon terminals → synaptic 5-HT rises at target regions. This is when therapeutic effects begin. The delay explains why SSRIs don't work immediately.
-
Later (4–8 weeks): Postsynaptic 5-HT receptors downregulate as well → tolerance to side effects develops, and sustained clinical response is established.
Psychodynamic Considerations
PART 3 — PHARMACOKINETICS
Comparison Table
| Drug | Half-life | Active metabolite | CYP inhibition | Protein binding | Bioavailability |
|---|---|---|---|---|---|
| Fluoxetine | 2–3 days | Norfluoxetine (t½ ~2 wks) | 2D6 (potent), 3A4, 2C9 | 94% | 72% |
| Sertraline | 26 hrs | Desmethylsertraline (weak) | 2D6 (moderate), 3A4 | 98% | Variable |
| Paroxetine | 20 hrs | None (major) | 2D6 (potent), 3A4 | 95% | ~50% |
| Fluvoxamine | 15–20 hrs | None | 1A2 (potent), 2C9, 3A4 | 80% | 53% |
| Citalopram | 35 hrs | Desmethylcitalopram (weak) | Minimal | 80% | 80% |
| Escitalopram | 27–32 hrs | None significant | Minimal (2D6 weak) | 56% | 80% |
- Fluoxetine has the longest combined half-life (~7 days including norfluoxetine). This means: (a) no significant discontinuation syndrome, (b) no need for taper on stopping, (c) requires 5-week washout before starting an MAOI.
- Paroxetine has the shortest half-life and is an autoinhibitor of its own metabolism (CYP2D6) — even small dose reductions cause disproportionately steep plasma level drops, causing the worst discontinuation syndrome of all SSRIs.
- Escitalopram has minimal CYP interactions — best choice when polypharmacy is a concern (Harrison's).
- All SSRIs achieve steady-state in ~5 half-lives. For fluoxetine this takes ~5 weeks.
- All are extensively protein-bound — less affected by renal disease; dose-adjust in severe hepatic impairment.
- Food does not significantly affect absorption of any SSRI.
CYP Interactions — Clinical Implications
| CYP | Inhibitor SSRI | Substrates at risk |
|---|---|---|
| 2D6 | Fluoxetine, paroxetine (potent); sertraline (moderate) | TCAs, antipsychotics, codeine→morphine conversion, tamoxifen |
| 1A2 | Fluvoxamine (potent) | Clozapine, olanzapine, theophylline, caffeine |
| 3A4 | Fluvoxamine, fluoxetine | Carbamazepine, digoxin, benzodiazepines |
| Minimal | Citalopram, escitalopram | Safest choice in complex regimens |
Tamoxifen note (2025 update): CYP2D6 inhibitors (fluoxetine, paroxetine) theoretically reduce conversion of tamoxifen to endoxifen. However, a 2022 systematic review of ~100,000 breast cancer patients found no adverse oncologic outcomes from concurrent use; updated guidelines recommend not switching antidepressants solely for this reason.
PART 4 — INDICATIONS
FDA-Approved Indications (US) by Drug
| Indication | Flu | Ser | Par | Flv | Cit | Esx |
|---|---|---|---|---|---|---|
| Major Depressive Disorder | ✓ | ✓ | ✓ | — | ✓ | ✓ |
| OCD | ✓ | ✓ | ✓ | ✓ | — | — |
| Panic Disorder | ✓ | ✓ | ✓ | — | — | — |
| Social Anxiety Disorder | — | ✓ | ✓ | ✓ | — | — |
| GAD | — | — | ✓ | — | — | ✓ |
| PTSD | — | ✓ | ✓ | — | — | — |
| PMDD | ✓ | ✓ | ✓ | ✓ | — | — |
| Bulimia Nervosa | ✓ | — | — | — | — | — |
| BDD | — | — | ✓ | — | — | — |
Off-Label Uses (well-supported)
- Generalized anxiety disorder (all SSRIs)
- Body dysmorphic disorder
- Trichotillomania & skin-picking disorder
- Premenstrual dysphoric disorder (low-dose intermittent)
- Fibromyalgia (fluoxetine)
- Premature ejaculation (paroxetine — evidence-based off-label)
- Irritable bowel syndrome
- Hot flashes (menopause-related)
- Autism-associated repetitive behaviors
PART 5 — CLINICAL GUIDELINES & TREATMENT ALGORITHM
First-Line Selection (2024–2025 Guidelines)
- Start with escitalopram or sertraline — best efficacy-tolerability balance, fewest drug interactions, most evidence.
- Alternatives: fluoxetine (if activating properties needed, eating disorders, pregnancy [most data]), paroxetine (if sedation needed, though avoid in elderly), citalopram (avoid >40 mg due to QTc).
- Paroxetine is least preferred for: elderly patients, pregnancy (neonatal withdrawal), patients likely to need future dose adjustments.
Step-Care Algorithm
Step 1: Start SSRI (escitalopram/sertraline preferred)
↓ 4–8 weeks at therapeutic dose
Step 2: Inadequate response?
→ Optimize dose (go to maximum tolerated)
→ 4 more weeks
↓
Step 3: Still inadequate?
→ Switch: SSRI → SNRI (or different SSRI)
→ Or Augment: lithium, aripiprazole, quetiapine, T3
↓
Step 4: Treatment-resistant (≥2 adequate trials failed)
→ ECT, ketamine/esketamine, TMS
→ Consider MAOIs (specialist)
PART 6 — DOSING & FORMULATIONS
Standard Doses
| Drug | Starting dose | Usual therapeutic | Maximum | Available forms |
|---|---|---|---|---|
| Fluoxetine | 10–20 mg/day | 20–40 mg | 80 mg (OCD/bulimia) | Capsule, tablet, liquid; weekly delayed-release capsule (Prozac Weekly, 90 mg) |
| Sertraline | 25–50 mg/day | 50–200 mg | 200 mg | Tablet, oral concentrate |
| Paroxetine IR | 10–20 mg/day | 20–40 mg | 60 mg | Tablet, liquid |
| Paroxetine CR | 12.5–25 mg/day | 25–50 mg | 62.5 mg | Extended-release tablet |
| Fluvoxamine | 50 mg/day | 100–300 mg | 300 mg | Tablet; CR capsule |
| Citalopram | 10–20 mg/day | 20–40 mg | 40 mg (QTc limit) | Tablet, liquid |
| Escitalopram | 5–10 mg/day | 10–20 mg | 20 mg | Tablet, liquid |
Titration Principles
- Start low, go slow — especially in anxiety disorders (initial activation effect can worsen anxiety)
- Increase dose after 2–4 weeks if tolerated but subtherapeutic response
- Allow 4–8 weeks at therapeutic dose before declaring a trial failed
- In elderly: start at half the adult starting dose; titrate more slowly
- In children/adolescents: fluoxetine has the most RCT evidence; start at 10 mg
PART 7 — THE SIX SSRIs INDIVIDUALLY
1. FLUOXETINE (Prozac)
- Most activating → best for depression with hypersomnia, psychomotor retardation, fatigue, apathy
- May worsen agitation and insomnia in anxious patients
- Only SSRI approved for bulimia nervosa (higher dose, 60 mg)
- Approved for depression + bipolar when combined with olanzapine (Symbyax)
2. SERTRALINE (Zoloft)
- Best overall efficacy-tolerability balance — most broadly prescribed SSRI worldwide
- Lowest risk of drug-drug interactions of the commonly used SSRIs (Harrison's)
- GI side effects (diarrhea) slightly more common than others
- DAT inhibition may improve motivation and drive at higher doses
- Sigma-1 binding: potential anxiolytic properties, mood stabilization
3. PAROXETINE (Paxil, Paxil CR)

- Most anticholinergic SSRI → dry mouth, constipation, urinary hesitancy, blurred vision, sedation
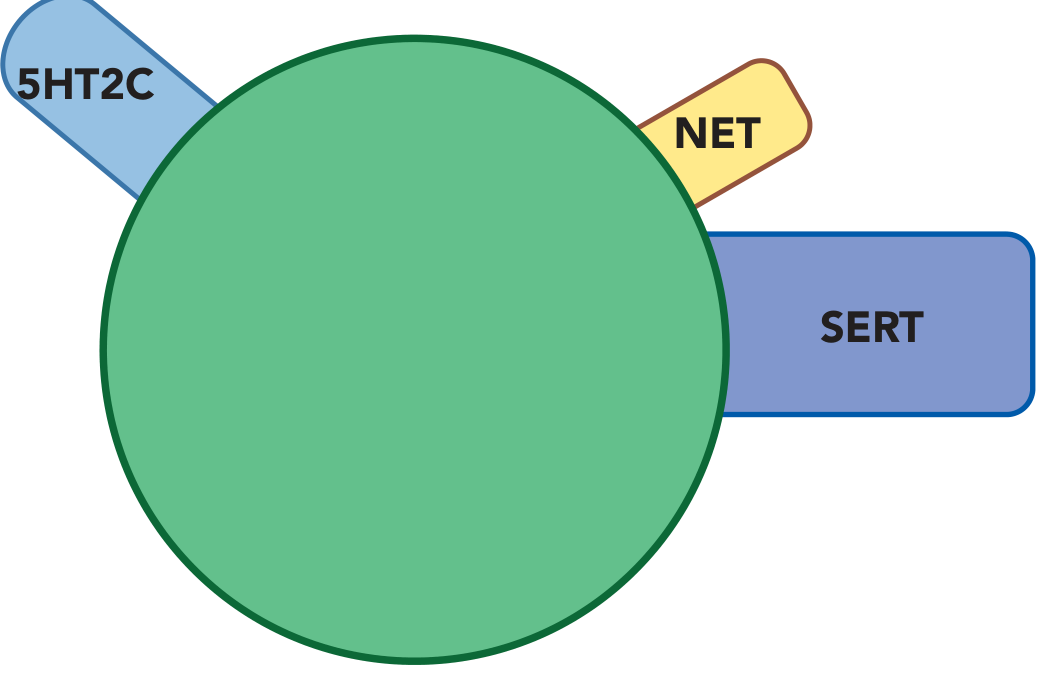
- NET inhibition → slightly more noradrenergic than other SSRIs → possibly more robust for anxiety
- NOS inhibition → contributes to sexual dysfunction and premature ejaculation treatment
- Most sedating SSRI → useful for patients with insomnia-predominant depression
- Most problematic for discontinuation syndrome (shortest half-life + autoinhibition of CYP2D6)
4. FLUVOXAMINE (Luvox)

- Not FDA-approved for MDD in adults (approved for OCD and social anxiety)
- Sigma-1 receptor agonism: anxiolytic, antipsychotic-like, neuroprotective effects; may confer unique benefits in autism, OCD, schizophrenia
- OCD drug of first choice in children in some guidelines
- Most significant CYP interactions of all SSRIs (inhibits 1A2, 2C9, 3A4) → use caution with clozapine, olanzapine (can markedly raise levels), theophylline, warfarin
- Must be given twice daily (no once-daily formulation except CR capsule)
- COVID-19 note: Fluvoxamine gained attention in 2020–2022 (TOGETHER trial) for possible benefit in early COVID via sigma-1 agonism; results were modest and not definitive
5. CITALOPRAM (Celexa)
- Cleanest pharmacological profile of the original SSRIs — least receptor promiscuity
- Minimal CYP interactions → good for elderly and polypharmacy patients
- Critical safety issue: QTc prolongation
- FDA black box warning (2012): maximum dose 40 mg/day (20 mg/day in elderly, hepatic impairment, or with CYP2C19 inhibitors like omeprazole)
- Dose-dependent QTc prolongation → risk of torsades de pointes at higher doses
- Monitor ECG in high-risk patients
6. ESCITALOPRAM (Lexapro) — The Quintessential SSRI
- Most selective SSRI — virtually no off-target effects
- Allosteric SERT binding: the S-enantiomer binds both the primary (orthosteric) and a secondary (allosteric) site on SERT — this may contribute to superior potency and possibly faster onset
- Minimal CYP inhibition → fewest drug interactions of all SSRIs (Harrison's)
- Best-tolerated SSRI in most comparative studies
- Consistently ranks #1 or #2 for efficacy in network meta-analyses (Cipriani 2018 Lancet)
- Effective across: MDD, GAD, social anxiety, panic disorder, OCD (off-label)
PART 8 — SIDE EFFECTS
Common Side Effects (All SSRIs)
- Dose reduction
- Drug holidays (2–3 times/month — not effective with fluoxetine due to long half-life)
- Switch to bupropion, mirtazapine, vortioxetine, or agomelatine (lower risk)
- Add sildenafil/tadalafil (evidence for men; limited for women)
- Add bupropion 100–150 mg/day (Maudsley)
- Amantadine 100 mg tid; buspirone 10 mg tid (Harrison's)
Serious/Rare Side Effects
PART 9 — SEROTONIN SYNDROME
Hunter Criteria for Diagnosis (requires ONE of):
- Spontaneous clonus
- Inducible clonus + agitation/diaphoresis
- Ocular clonus + agitation/diaphoresis
- Tremor + hyperreflexia
- Hypertonia + temperature >38°C + clonus
Classic Triad:
- Neuromuscular: clonus (pathognomonic), hyperreflexia, tremor, myoclonus, rigidity
- Autonomic: hyperthermia, tachycardia, diaphoresis, hypertension
- Cognitive: agitation, confusion
Precipitating Combinations:
- SSRI + MAOI (most dangerous — avoid; requires washout)
- SSRI + tramadol, fentanyl, meperidine
- SSRI + triptans (theoretical; clinical risk debated)
- SSRI + linezolid (weak MAOI)
- SSRI + St. John's Wort
- SSRI + dextromethorphan
- SSRI + lithium (at toxic lithium levels)
Management:
- Stop all serotonergic agents immediately
- Supportive care: IV fluids, cooling
- Benzodiazepines for agitation and seizures
- Cyproheptadine 12 mg PO then 2 mg every 2 hrs (5-HT2A antagonist — antidote)
- Severe cases: ICU, intubation, temperature control
- Do NOT use physical restraints (cause hyperthermia)
PART 10 — OVERDOSE & TOXICITY
Clinical Features of Overdose:
- Tachycardia, mild hypotension, lethargy (especially with co-ingestants)
- Citalopram/escitalopram: most dangerous in overdose → dose-dependent QTc prolongation, QRS widening, seizures, torsades de pointes (even at overdoses of 600–1000 mg)
- Serotonin syndrome occurs in ~10% of overdoses
Treatment (Tintinalli):
| Intervention | Indication |
|---|---|
| IV access + cardiac monitor + ECG | All intentional ingestions |
| Activated charcoal (single dose) | Within 1 hour of ingestion |
| Benzodiazepines | Seizures (first-line) |
| Phenobarbital | Refractory seizures |
| Sodium bicarbonate | Prolonged QRS |
| Magnesium sulfate | QTc prolongation, torsades |
| Cyproheptadine | Serotonin syndrome |
- Observe 6 hours minimum; admit if: persistent tachycardia, altered mental status, citalopram/escitalopram ingestion, cardiac conduction abnormalities, serotonin syndrome features
- Gastric lavage, ipecac, whole-bowel irrigation: NOT recommended
PART 11 — SWITCHING STRATEGIES
Why Switch?
- Inadequate response after adequate trial (4–8 weeks at therapeutic dose)
- Intolerable side effects
- Drug interaction burden
Switching Principles
Stop current SSRI, start new SSRI at a low dose the next day. For SSRI-to-SSRI switches, washout is rarely needed (similar mechanisms, no dangerous interactions). Cross-taper (overlap while tapering old drug) can reduce discontinuation symptoms.
- Gradually taper down the first SSRI while gradually titrating up the new one
- Preferred for: paroxetine (due to discontinuation risk), patients sensitive to discontinuation
- Can usually do direct switch or cross-taper
- No washout required
| From | Washout before MAOI |
|---|---|
| Fluoxetine | 5 weeks (norfluoxetine half-life) |
| All other SSRIs | 2 weeks |
- Always 2 weeks washout after stopping MAOI before starting any SSRI
Step-down titration for discontinuation (Maudsley Deprescribing Guidelines):
- Never abrupt discontinuation (except fluoxetine which can usually be stopped without taper)
- Paroxetine, venlafaxine: hyperbolic tapering — small percentage reductions over months
- Use liquid formulations or pill-cutting for micro-tapering
- Fluoxetine bridge: switch to fluoxetine (long half-life), stabilize, then taper fluoxetine slowly
PART 12 — DISCONTINUATION SYNDROME
FINISH Mnemonic:
- Flu-like symptoms (myalgias, sweating, nausea)
- Insomnia (vivid dreams, nightmares)
- Nausea/GI distress
- Imbalance/dizziness
- Sensory disturbances ("brain zaps" — electric shock sensations in head)
- Hyperactivation (anxiety, agitation, irritability)
Risk by Drug (Highest → Lowest):
- Paroxetine (shortest half-life + autoinhibition = steepest drop)
- Venlafaxine (short half-life, though technically SNRI)
- Sertraline, citalopram, escitalopram (moderate)
- Fluvoxamine
- Fluoxetine (virtually none — long half-life provides self-taper)
Management:
- Prevention: Always taper; educate patients
- Mild: Reassurance; usually resolves 1–2 weeks
- Moderate-severe: Restart drug → stabilize → slower taper
- Fluoxetine bridge: Switching to fluoxetine, stabilizing, then tapering leverages its self-tapering property
- Kaplan & Sadock: movement symptoms (tremor, akathisia, parkinsonism) on discontinuation — manage akathisia with propranolol, anticholinergics, or benzodiazepines
PART 13 — CONTRAINDICATIONS
Absolute:
- Concurrent MAOI use (fatal serotonin syndrome risk)
- Known hypersensitivity to the drug
Relative / Caution:
| Situation | Guidance |
|---|---|
| Bipolar disorder (unprotected) | Risk of manic switch — use mood stabilizer first |
| QTc >500 ms | Avoid citalopram/escitalopram |
| Seizure disorders | Generally safe but use cautiously |
| Severe hepatic impairment | Halve dose; fluoxetine safest (long half-life allows slow titration) |
| Elderly | Start low, watch for hyponatremia, falls |
| Pregnancy | Fluoxetine, sertraline safest (most data); paroxetine least preferred (cardiac anomaly signal) |
| Lactation | Sertraline: lowest breast milk transfer; paroxetine also low; fluoxetine: infant serum levels higher |
| Tamoxifen | Avoid fluoxetine and paroxetine (strong 2D6 inhibitors) — use escitalopram or sertraline instead |
| Bleeding risk / NSAIDs | Add PPI; monitor |
| Linezolid / methylene blue | Contraindicated (MAOI-like activity — serotonin syndrome risk) |
PART 14 — SPECIAL POPULATIONS
Children & Adolescents:
- Fluoxetine: only SSRI FDA-approved for depression in children ≥8 years
- Fluoxetine and escitalopram: approved for adolescent depression
- All SSRIs: FDA black box warning — increased suicidal ideation in under-25s; monitor weekly initially
- OCD in children: sertraline, fluoxetine, fluvoxamine (all FDA-approved)
- CBT must accompany pharmacotherapy; do not use medication as sole treatment
Elderly:
- Start at half the adult dose; titrate slowly
- Preferred: escitalopram, sertraline (fewest interactions, no anticholinergic)
- Avoid paroxetine (Beers criteria — anticholinergic)
- Monitor: sodium (SIADH), falls (dizziness), QTc (avoid citalopram >20 mg)
Pregnancy:
- SSRIs are the most studied antidepressants in pregnancy
- Neonatal Adaptation Syndrome: transient in newborns — jitteriness, respiratory distress, poor feeding (especially paroxetine, venlafaxine); resolves in days; not a reason to withhold treatment
- Persistent Pulmonary Hypertension of Newborn (PPHN): weak signal with late-pregnancy SSRI exposure; absolute risk very low
- 2025 umbrella review (Fabiano et al., Mol Psychiatry): overall, SSRIs do not show strong teratogenic signal; risk of untreated depression > risk of SSRI exposure
Cardiac Disease:
- SADHART trial (2002): Sertraline safe in post-MI patients with depression; does not worsen cardiac outcomes
- ENRICHD trial: CBT + sertraline improved depression post-MI
- Preferred: sertraline, escitalopram (minimal CYP, no QTc at therapeutic doses)
- Avoid: citalopram >40 mg; paroxetine (anticholinergic, tachycardia)
PART 15 — EVIDENCE-BASED TRIALS
Landmark Studies
- Largest real-world antidepressant trial (n=4,041); used citalopram as first step
- 28% remission at step 1 (citalopram)
- Only ~33% remission after 4 steps → established treatment-resistance as a major clinical challenge
- Key message: most patients need more than one treatment step
- 522 trials, 116,477 patients, 21 antidepressants
- Escitalopram and sertraline had best combination of efficacy and acceptability
- All SSRIs were more efficacious than placebo
- Escitalopram ranked highest for both efficacy and tolerability
- SSRIs + SNRIs first-line for MDD, GAD, PTSD, OCD, panic disorder, social anxiety
- Augmentation with atypical antipsychotics (aripiprazole, quetiapine, brexpiprazole) for partial responders
- Level 1 evidence for escitalopram and sertraline in MDD
- Escitalopram vs. other antidepressants (Yin et al., BMC Psychiatry 2023, PMID 38001423): Escitalopram showed superior response and remission vs. several other antidepressants
- Panic disorder (Guaiana et al., Cochrane 2023, PMID 38014714): SSRIs and benzodiazepines both effective; SSRIs preferred long-term
- Hyponatremia risk (Gheysens et al., Eur Psychiatry 2024, PMID 38403888): SSRIs carry higher hyponatremia risk than other antidepressant classes
- SSRI safety in pregnancy (Fabiano et al., Mol Psychiatry 2025, PMID 39266712): low absolute teratogenic risk confirmed
PART 16 — RECENT ADVANCES (2023–2026)
-
Post-SSRI Sexual Dysfunction (PSSD): EMA and FDA have mandated label updates acknowledging PSSD as a real, potentially persistent adverse effect. Research ongoing into mechanisms (epigenetic? neurosteroid?).
-
Pharmacogenomics in SSRI prescribing: CYP2D6 and CYP2C19 genotyping is increasingly available; strong metabolizers may need higher doses; poor metabolizers risk toxicity. Not yet in routine guidelines but several countries are moving toward it.
-
Antidepressants and neuroplasticity: Beyond the monoamine hypothesis — antidepressants enhance BDNF signaling, promote neurogenesis in the hippocampus, and facilitate synaptic remodeling. This "neuroplasticity hypothesis" may explain why combining SSRIs with psychotherapy is synergistic.
-
Esketamine (Spravato) as augmentation / monotherapy: FDA approved esketamine as first monotherapy for treatment-resistant depression in January 2025 — not an SSRI, but defines the "after SSRI fails" landscape.
-
SSRI hyperbolic tapering (Maudsley Deprescribing Guidelines, 2022+): Evidence-based protocol for SSRI discontinuation using hyperbolic dose reductions (small % reductions of remaining dose) rather than linear steps — prevents protracted withdrawal. Widely adopted in UK.
-
Gepirone (Exxua) FDA approved 2023: A 5-HT1A partial agonist/5-HT2 antagonist antidepressant — new class but with serotonergic mechanism, positioned alongside SSRIs.
-
Digital phenotyping and prediction of SSRI response: Machine learning models using EEG biomarkers (e.g., frontal alpha asymmetry) and digital biomarkers to predict SSRI response before prescribing — early research stage.
QUICK REFERENCE SUMMARY TABLE
| Drug | Unique feature | Best for | Avoid in | Key interaction | Half-life |
|---|---|---|---|---|---|
| Fluoxetine | 5-HT2C antagonism, activating | Hypersomnia, bulimia, low adherence | Agitated/anxious patients | 5-wk MAOI washout | ~7 days (with norfluoxetine) |
| Sertraline | Fewest interactions, PTSD | Pregnancy, cardiac disease, PTSD | — | Minimal | 26 hrs |
| Paroxetine | Anticholinergic, sedating | Insomnia, PE treatment | Elderly, pregnancy, dose-flexible patients | 2D6 potent | 20 hrs (autoinhibitor) |
| Fluvoxamine | Sigma-1 agonism | OCD, autism, unique receptor profile | Polypharmacy (1A2) | 1A2: clozapine↑↑↑ | 15–20 hrs |
| Citalopram | Racemic, cleanest profile | Simple cases, elderly | QTc risk, >40 mg | Minimal | 35 hrs |
| Escitalopram | S-enantiomer, allosteric SERT | First-line, elderly, MDD+GAD | — | Minimal | 27–32 hrs |
Sources
- Stahl's Essential Psychopharmacology, Cambridge University Press
- Harrison's Principles of Internal Medicine, 22nd ed. (McGraw-Hill, 2025)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, 10th ed.
- The Maudsley Prescribing Guidelines in Psychiatry, 15th ed.
- Tintinalli's Emergency Medicine, 9th ed.
- Cipriani et al., Lancet 2018 (network meta-analysis, 21 antidepressants)
- Yin et al., BMC Psychiatry 2023 [PMID 38001423]
- Guaiana et al., Cochrane 2023 [PMID 38014714]
- Gheysens et al., Eur Psychiatry 2024 [PMID 38403888]
- Fabiano et al., Mol Psychiatry 2025 [PMID 39266712]
Explain further
Please teach me autism spectrum disorder…everything related to it, hisotry, intro, etiolody, epidemiology, clinical features, distinctive features of disease, how to diagnose, what questions to ask to caregiver for diagnosis, treatment pharmacological,
"autism spectrum disorder"[MeSH Terms] AND "diagnosis"[MeSH Terms]
autism spectrum disorder 2024 2025 clinical practice guidelines diagnosis treatment
Autism Spectrum Disorder (ASD) — Complete Teaching Guide
PART 1 — HISTORY
The Kanner–Asperger Origins
Evolution of Diagnostic Concepts
| Era | Concept | Key Shift |
|---|---|---|
| 1950s–60s | "Childhood schizophrenia" | Autism conflated with psychosis; Bettelheim's discredited "refrigerator mother" theory |
| 1980 | DSM-III | First separate category: "infantile autism" |
| 1987 | DSM-III-R | Renamed "autistic disorder"; broader criteria |
| 1994 | DSM-IV | Five categories: autistic disorder, Asperger's disorder, PDD-NOS, Rett syndrome, childhood disintegrative disorder |
| 2013 | DSM-5 | All collapsed into a single "Autism Spectrum Disorder" — spectrum model, two core domains |
| 2022 | DSM-5-TR | Minor text revisions, same criteria |
PART 2 — DEFINITION & INTRODUCTION
- Persistent deficits in social communication and social interaction
- Restricted, repetitive patterns of behavior, interests, or activities
- ASD is not a single disease — it is an umbrella of neurobiologically heterogeneous syndromes sharing behavioral phenotype
- No biological marker yet qualifies as a diagnostic test; diagnosis remains entirely behavioral/clinical
- ASD is not progressive — but trajectories vary widely
- ~10% of clearly affected children show substantial improvement with early intensive intervention (Kandel, Principles of Neural Science)
PART 3 — EPIDEMIOLOGY
Prevalence
- Current estimates: 1 in 36 children (US CDC, 2023) — approximately 2.8% of 8-year-olds
- Global estimates range 1–2.6% when using rigorous epidemiological methods
- Prevalence has risen dramatically over decades: this reflects diagnostic expansion, increased awareness, diagnostic substitution (children previously labeled intellectually disabled), and a possible true increase in incidence (Kandel)
Sex Ratio
- 4:1 male-to-female ratio (traditional figure)
- Recent research suggests this may be inflated due to male bias in diagnostic instruments and the "female camouflaging phenotype" — girls with ASD mask symptoms more effectively
- Corrected estimate: likely 2:1 to 3:1 male excess (Kandel)
- Females with ASD tend to be diagnosed later and have higher IQ at diagnosis
Age at Diagnosis
- Average age: 3.1 years for classic autism; 7.2 years for former Asperger's disorder
- Symptoms typically evident by second year of life; in severe cases, first year
- High-risk infants (sibling of diagnosed child) can show reliable differences within the first year
- ~⅓ of children with ASD have intellectual disability (Kaplan & Sadock)
- ASD occurs in all countries, cultures, and socioeconomic groups
Co-occurring Conditions (Micai et al., 2023 — Systematic Review, PMID 37913872)
- ADHD: ~50–70%
- Anxiety disorders: ~40–50%
- Intellectual disability: ~30–35%
- Language disorder: ~40–50%
- Epilepsy/seizures: 4–32% (increases with intellectual disability severity)
- Sleep disorders: 40–80%
- Depression: ~20–30% (increases with age)
- Sensory processing difficulties: ~90%
- GI problems: ~45–50%
PART 4 — ETIOLOGY
A. Genetic Factors (Primary — ~80% Heritability)
- Monozygotic concordance: 60–90% (broad phenotype)
- Dizygotic concordance: 5–10% — strongly implicates genetics
-
Rare single-gene mutations (high-effect, rare):
- De novo (not inherited) mutations in genes encoding synaptic proteins
- Key genes: SHANK3 (scaffold protein), NLGN4X (neuroligin, synaptic adhesion), NRXN1 (neurexin), CHD8 (chromatin remodeling), DYRK1A, ADNP
- These individually account for a small fraction but provide major mechanistic insights
-
Copy Number Variations (CNVs):
- De novo submicroscopic chromosomal deletions/duplications
- Key loci: 16p11.2, 1q21, 15q11-13, 22q11, 22q13, 2p16, 3q29
- 16p11.2 deletion/duplication: >10-fold increased ASD risk
- Same CNVs also increase risk for schizophrenia and bipolar disorder — common genetic pathways
-
Common variants (polygenic):
- Hundreds of common single nucleotide polymorphisms (SNPs), each with tiny effect
- GWAS studies identify risk loci in genes regulating synaptic function, neuronal migration, chromatin remodeling
| Syndrome | Gene/Mechanism | ASD-like Features |
|---|---|---|
| Fragile X | FMR1 repeat expansion (CGG); loss of FMRP → excess mGluR5 signaling | Stereotypies, social avoidance, ID, macrocephaly, macro-orchidism |
| Rett syndrome | MECP2 mutation (X-linked); loss of methyl-CpG-binding protein | Normal development → regression, hand-wringing stereotypies, loss of language |
| Angelman syndrome | Loss of maternal UBE3A (15q11-13) | Social affect relatively preserved, severe ID, seizures, happy demeanor |
| Prader-Willi | Loss of paternal 15q11-13 | Social cognitive deficits, hyperphagia |
| Williams syndrome | 7q11.23 deletion (elastin gene region) | Paradoxically hypersocial, but socially naive; language relatively preserved |
| Tuberous sclerosis | TSC1/TSC2 | ASD in ~50%; cortical tubers |
| 22q11 deletion | Velocardiofacial syndrome | ASD and schizophrenia risk |
B. Neurobiological Mechanisms
- Early brain overgrowth — enlarged total brain volume before age 5 years; 15–20% develop macrocephaly by age 5
- Amygdala enlargement in early childhood → normalizes or decreases by adolescence
- Enlarged striatum in young children (correlates with repetitive behavior frequency)
- Structural and functional MRI (2024 meta-analysis, Guo et al., Mol Autism): multimodal neuroimaging consistently shows reduced long-range cortical connectivity and local hyper-connectivity, especially in social brain networks (fusiform face area, medial prefrontal cortex, superior temporal sulcus)
C. Environmental Risk Factors
| Factor | Evidence |
|---|---|
| Advanced paternal and maternal age | Consistent finding; older fathers have higher de novo mutation rates |
| Prenatal valproate exposure | 6–15-fold increased ASD risk; mechanism: HDAC inhibition |
| Prenatal thalidomide exposure | Historical data |
| Prenatal infection (rubella, CMV) | Historical; rare |
| Gestational diabetes | Associated |
| Maternal gestational bleeding | Associated |
| Low birth weight, prematurity | Associated |
| Perinatal hypoxia | Risk factor for multiple neurodevelopmental outcomes |
| Maternal autoantibodies against fetal brain | Under investigation |
D. Psychosocial Factors — NONE
PART 5 — PATHOPHYSIOLOGY & NEUROSCIENCE
The Mind Blindness Hypothesis (Baron-Cohen)
- Difficulty reading facial expressions and body language
- Impaired empathy and perspective-taking
- Literal interpretation of language (missing metaphor, sarcasm, irony)
- Difficulty understanding social conventions
Weak Central Coherence
- Attention to individual features rather than whole faces
- Superior performance on embedded-figures tasks
- Insistence on same details in routines
Executive Dysfunction
- Restricted, repetitive behaviors
- Difficulty with transitions and novel situations
- Perseverative thinking
Mirror Neuron System Dysfunction
PART 6 — DSM-5 DIAGNOSTIC CRITERIA
Domain A: Social Communication and Interaction (ALL THREE required)
- Abnormal social approach
- Failure of normal back-and-forth conversation
- Reduced sharing of interests, emotions, affect
- Failure to initiate or respond to social interactions
- Poorly integrated verbal and nonverbal communication
- Abnormalities in eye contact and body language
- Deficits in understanding and use of gestures
- Total lack of facial expressions and nonverbal communication
- Difficulties adjusting behavior to social context
- Difficulties in sharing imaginative play
- Absence of interest in peers
- Difficulties making friends
Domain B: Restricted, Repetitive Behaviors (AT LEAST TWO of four required)
- Simple motor stereotypies (hand-flapping, rocking, spinning)
- Lining up toys or flipping objects
- Echolalia (immediate or delayed)
- Idiosyncratic phrases ("scripting")
- Extreme distress at small changes
- Rigid thinking patterns
- Ritualized patterns of verbal or nonverbal behavior
- Same routes/foods
- Strong attachment to unusual objects
- Excessively circumscribed or perseverative interests
- Apparent indifference to pain/temperature
- Adverse response to specific sounds or textures
- Excessive smelling or touching of objects
- Visual fascination with lights or movement
Additional Criteria:
- C. Symptoms present in the early developmental period
- D. Symptoms cause clinically significant impairment
- E. Not better explained by intellectual disability or global developmental delay
DSM-5 Severity Levels
| Level | Social Communication | Restricted/Repetitive |
|---|---|---|
| Level 1 ("requiring support") | Without supports, noticeable impairments; difficulty initiating social interactions | Inflexibility causes significant interference; difficulty switching tasks |
| Level 2 ("requiring substantial support") | Marked deficits; limited initiation; reduced/abnormal responses | Inflexibility, difficulty coping with change; obvious to casual observer |
| Level 3 ("requiring very substantial support") | Severe deficits; very limited initiation; minimal response | Extreme difficulty with change; repetitive behaviors markedly interfere |
Specifiers:
- With/without intellectual impairment
- With/without language impairment
- Associated with known medical/genetic condition
- Associated with another neurodevelopmental, mental, or behavioral disorder
- With catatonia
PART 7 — CLINICAL FEATURES IN DETAIL
Early Warning Signs (Red Flags)
- No babbling
- No pointing, waving, or reaching (no joint attention)
- No response to name
- No social smile
- No single words
- No two-word spontaneous phrases (not echolalia)
- Any regression in language or social skills at any age
Social Communication Features
- Failure to develop anticipatory posture when about to be picked up
- Reduced or absent social smile
- Atypical attachment — may not differentiate primary caregivers from strangers
- Reduced eye contact (less frequent, less sustained)
- Absent joint attention (not following the caregiver's gaze; not pointing to share interest)
- Parallel play without peer interaction
- Does not bring items to show parents (protodeclarative pointing absent)
- Social withdrawal; more interested in objects than people
- May resist being cuddled or held
- Awkward social interactions; difficulty initiating and sustaining conversations
- One-sided conversations (talks at, not with)
- Literal interpretation of language; confused by idioms and sarcasm
- Difficulty understanding social hierarchies and rules
- Peer relationships absent or superficial
- May desire relationships but lack skills to form them
- Vulnerability to bullying and social exploitation
- May develop anxiety and depression as secondary consequences of social failure
- Camouflaging (especially females): consciously masking autistic traits — exhausting, leads to burnout
Language and Communication Features
- ~50% of children with classic ASD never develop functional speech (historical figure; with early intervention, this is now lower)
- Echolalia (immediate and delayed) — repeating phrases without communicative intent
- Pronoun reversal ("you want the toy" meaning "I want the toy")
- Pedantic speech — unusually formal or verbose in higher-functioning individuals
- Monotone or unusual prosody; unusual rhythm and pitch
- Hyperlexia — can read words fluently without comprehension
- Words drop in and out of vocabulary; a word used once may not reappear for months
Restricted and Repetitive Behaviors
- Stereotypies: hand-flapping, rocking, spinning, toe-walking
- Insistence on sameness: same route to school, same food, same order of events; catastrophic reactions to unexpected change
- Object preoccupations: lining up toys, spinning wheels, fixation on specific topics
- Restricted interests: intense, encyclopedic knowledge of narrow topics (trains, dinosaurs, prime numbers)
- Sensory features: hyperacusis (distress to specific sounds), tactile defensiveness, seeking vestibular stimulation (spinning, swinging), unusual pain threshold
Behavioral Features
- Irritability: aggression (toward self or others), temper tantrums, self-injurious behaviors (head-banging, skin-picking, self-biting) — especially in lower-functioning children
- Hyperactivity and inattention: common, especially in younger children
- Mood instability: sudden bursts of laughing or crying without apparent reason
- Anxiety: pervasive, often driven by unpredictability and sensory overload
- Insomnia: 40–80% prevalence; difficulty falling asleep, frequent waking, early morning waking
- Feeding problems: extreme food selectivity (often sensory-based — texture, color, smell)
Precocious / Splinter Skills ("Savant" abilities)
- Hyperlexia (reading at preschool age without comprehension)
- Extraordinary rote memory
- Calendar calculations
- Musical prodigy abilities
- Exceptional drawing or visual-spatial skills
Intellectual Profile
- ~30% have co-occurring intellectual disability
- Of those with ID: 30% mild–moderate range; 45–50% severe–profound range
- Even in those with ID: relative strengths in visuospatial tasks and rote memory vs. verbal reasoning
- About one-third of those with ASD have average or above-average IQ ("high-functioning ASD")
PART 8 — DIAGNOSTIC ASSESSMENT
Step 1: Developmental Surveillance (Level 1 Screening)
| Tool | Age | Method | Notes |
|---|---|---|---|
| M-CHAT-R/F (Modified Checklist for Autism in Toddlers, Revised with Follow-up) | 16–30 months | 20-item parent questionnaire; follow-up interview if positive | Most widely used; best evidence; free to use |
| STAT (Screening Tool for Autism in Toddlers) | 24–36 months | Interactive screening by clinician | Semi-structured play |
| PDDST-II (PDD Screening Test) | 18 months+ | Parent questionnaire | Three-stage process |
| Social Communication Questionnaire (SCQ) | 4 years+ | Parent questionnaire, 40 items | Based on ADI-R |
| ASSQ (Autism Spectrum Screening Questionnaire) | 7–16 years | School/parent rating | Asperger's-range screening |
Step 2: Comprehensive Diagnostic Assessment (Level 2)
| Instrument | Type | Who Administers | What It Measures |
|---|---|---|---|
| ADOS-2 (Autism Diagnostic Observation Schedule, 2nd ed.) | Direct observation | Trained clinician | Structured/semi-structured play and social interaction; observes social communication, restricted/repetitive behaviors; gives algorithm score |
| ADI-R (Autism Diagnostic Interview – Revised) | Parent interview | Trained clinician | Structured caregiver interview covering early development, language, social interaction, behavior; 93 items |
| CARS-2 (Childhood Autism Rating Scale, 2nd ed.) | Clinician rating | Clinician | 15-item rating scale; useful across ages |
| GARS-3 (Gilliam Autism Rating Scale) | Parent/teacher rating | Any professional | Norm-referenced; gives probability of ASD |
Step 3: Additional Investigations
| Investigation | Purpose |
|---|---|
| Audiogram | Rule out hearing impairment (language delay may mimic ASD) |
| Chromosomal microarray | First-tier genetic test; detects CNVs; positive in ~10–15% |
| FMR1 gene testing (Fragile X) | Rule out Fragile X (most common single-gene cause of ASD) |
| Metabolic screen | If regression or atypical features |
| EEG | If seizure concern; abnormal in 10–83% |
| MRI brain | Not routine; indicated if focal neurological signs, regression, macrocephaly |
| Wood's lamp | Tuberous sclerosis (ash-leaf macules) |
| MECP2 testing | Girls with regression and stereotypies (Rett syndrome) |
| Lead level, thyroid | Comorbid conditions |
| Psychological/neuropsychological testing | IQ, adaptive behavior (Vineland), academic achievement |
| Speech-language evaluation | Language profile, pragmatics |
| Occupational therapy evaluation | Sensory processing, fine motor, ADLs |
PART 9 — QUESTIONS TO ASK THE CAREGIVER
Developmental History
- "When did your child first smile at you?"
- "Does your child make eye contact? Is it consistent, or does it come and go?"
- "When you point at something, does your child look at what you're pointing at?"
- "Does your child point to show you things he's interested in, just to share — not because he wants them?"
- "Does your child reach up to be picked up?"
- "Does your child show things to you — like bring you a toy to show you?"
- "Does your child respond when you call his name?"
- "Does your child prefer playing with children or with objects?"
- "Does your child play pretend — like making a doll sleep or feeding a stuffed animal?"
- "Does your child seem interested in other children? Does he try to interact with them?"
- "How does your child react when you're hurt or upset?"
- "How old was your child when he said his first word? First two-word combination?"
- "Did your child ever lose language he had already acquired? When?"
- "Does your child repeat things people say (echolalia)?"
- "Does your child mix up 'I' and 'you' in sentences?"
- "How does your child communicate what he wants — pointing, pulling your hand, words?"
- "Does your child understand instructions? Simple? Complex?"
- "Does your child take things very literally?"
- "Does your child flap his hands, rock his body, or spin?"
- "Does your child line up or arrange objects in a certain way?"
- "Is your child very particular about routines — does he react badly when things change?"
- "Does your child have an intense interest in specific topics that he talks about constantly?"
- "Does your child eat a very limited range of foods? Are there textures or colors he refuses?"
- "Is your child sensitive to sounds, lights, fabrics, or textures?"
- "Did your child seem to develop normally and then lose skills? What skills? At what age?"
- "Can you describe what changed and when?"
- "Is there any family history of autism, learning difficulties, language problems, or intellectual disability?"
- "Were there any complications during pregnancy or delivery?"
- "Does your child have any seizures?"
- "Does your child have problems sleeping?"
- "Are there concerns about hearing or vision?"
Functional Questions (for severity and support needs):
- "Can your child dress, feed, and toilet himself?"
- "Does your child have safety awareness — does he run off or have no fear of traffic?"
- "Is he able to be in a regular classroom, or does he need special education support?"
- "Does your child have any friends? Any social relationships outside family?"
- "What are your biggest daily challenges?"
PART 10 — DIFFERENTIAL DIAGNOSIS
| Condition | Key distinguishing features |
|---|---|
| Global developmental delay | Delay across all domains; social skills relatively preserved; no restricted interests |
| Intellectual disability (without ASD) | Social drive present; no restricted/repetitive behaviors; language delay proportional to cognitive level |
| Language disorder | Social interaction and nonverbal communication intact; no restricted behaviors |
| Selective mutism | Speaks in some contexts; social interest and desire present |
| Childhood-onset schizophrenia | Psychosis; hallucinations; onset after normal development |
| ADHD | Social interest present; impulsive, not withdrawn; no restricted interests |
| Social (pragmatic) communication disorder | Impaired social communication but no restricted/repetitive behaviors — diagnosis excluded if ASD criteria met |
| Reactive attachment disorder | History of severe neglect; social behavior improves with appropriate caregiving |
| Rett syndrome | Female; normal early development → regression with stereotyped hand-wringing; specific genetics |
| Anxiety disorder | Social withdrawal secondary to anxiety; social desire present |
| Sensory processing disorder | Sensory features without social communication deficits |
| Hearing impairment | Audiogram normal in ASD |
| Lead poisoning | May cause regression; blood lead level elevated |
PART 11 — ASSOCIATED/COMORBID CONDITIONS
Seizures/Epilepsy
- 4–32% prevalence; bimodal onset — early childhood and again in adolescence
- All seizure types occur; infantile spasms in some cases
- Higher risk in those with lower IQ and tuberous sclerosis
- EEG abnormalities in 10–83% (not all have clinical seizures)
ADHD
- ~50–70% comorbidity
- DSM-5 now allows dual diagnosis of ASD + ADHD (not permitted in DSM-IV)
- Both inattentive and hyperactive-impulsive presentations occur
- Methylphenidate is effective but may be less so than in ADHD without ASD; lower doses often used
Anxiety
- Most common comorbid psychiatric disorder in school-age and adult ASD
- Includes social anxiety, generalized anxiety, separation anxiety, specific phobias, OCD-like features
- Often masked or expressed as increased rigidity, meltdowns, or somatic complaints
- CBT adapted for ASD shows evidence
Depression
- Increasingly common in adolescents and adults with ASD
- Driven by: social isolation, bullying, awareness of difference, camouflaging exhaustion, failed relationships
- Often atypical presentation — may manifest as increased rigidity, self-injury, withdrawal, or somatic symptoms
Intellectual Disability
- ~30–35% overall
- Ranges from mild to profound
- ASD with ID has worse prognosis for independence
Sleep Disorders
- 40–80% prevalence — most common: delayed sleep onset, night waking
- Biological basis: altered melatonin synthesis in some individuals
- Melatonin: well-supported evidence for efficacy and safety
GI Disorders
- ~45–50%: constipation, diarrhea, GERD, food selectivity
- May worsen behavioral symptoms (pain expression as aggression)
- Dietary management often needed
PART 12 — TREATMENT
Overview: No Cure, But Significant Improvement Possible
A. BEHAVIORAL AND EDUCATIONAL INTERVENTIONS
1. Applied Behavior Analysis (ABA) — Foundation of Early Intervention
- Discrete Trial Training (DTT): Structured, repetitive teaching of specific skills
- Pivotal Response Treatment (PRT): Naturalistic ABA targeting pivotal behaviors (motivation, self-management)
- Early Intensive Behavioral Intervention (EIBI): 20–40 hours/week for children under 5
- ABA meta-analysis (2024): treatment intensity is a critical moderator of outcomes; more hours associated with greater gains in communication and adaptive behavior in young children
- Best outcomes with early start (before age 3–4) and high intensity
2. TEACCH (Treatment and Education of Autistic and Communication-related Handicapped Children)
- University of North Carolina origin (1970s)
- Structured teaching using visual supports: picture schedules, visual boundaries, organized work areas
- Exploits ASD strengths in visual processing
- Promotes predictability → reduces anxiety, behavioral dysregulation
3. Speech-Language Therapy
- Core for language delays, pragmatic communication deficits
- May include AAC (Augmentative and Alternative Communication) for non-verbal children: PECS (Picture Exchange Communication System), speech-generating devices, apps
- Social pragmatics training for higher-functioning individuals
4. Occupational Therapy
- Sensory integration therapy
- Fine motor skills, self-care activities (dressing, feeding, hygiene)
- Sensory diet — structured sensory activities to regulate sensory system
5. Social Skills Training
- Group-based programs: PEERS (Program for Education and Enrichment of Relational Skills) — strong RCT evidence for adolescents and young adults
- Teaches literal social rules, conversation skills, friendship-building
6. Naturalistic Developmental Behavioral Interventions (NDBIs)
- Combine ABA with developmental approaches; delivered in natural settings
- Examples: JASPER (Joint Attention, Symbolic Play, Engagement, Regulation), ESDM (Early Start Denver Model)
7. Parent/Caregiver Training
- Essential — parents as co-therapists
- Training in behavioral management, communication support, sensory strategies
- Reduces parenting stress, improves child outcomes
8. Computer-based and Virtual Reality approaches
- Programs like Let's Face It! — computerized face processing training; RCT evidence for improved face recognition
- VR environments teaching social interactions (ordering food, navigating social situations)
9. Insomnia Management
- Behavioral: sleep hygiene, graduated extinction, caregiver-focused approaches (removing attention for waking behavior)
- Pharmacological: melatonin (see below)
- Massage therapy before bedtime has shown evidence of improved sleep onset in ages 2–13
B. PHARMACOLOGICAL TREATMENT
1. IRRITABILITY (Aggression, Self-Injury, Severe Temper Tantrums)
Risperidone (Risperdal)
- FDA-approved for ASD-related irritability in children and adolescents 5–16 years
- Mechanism: D2 + 5-HT2A antagonism
- Evidence: 7 RCTs + 3 reanalysis studies + 2 add-on studies — consistent reduction in aggression, self-injury, tantrums
- RUPP Autism Network trial: Risperidone superior to placebo; 57% responder rate vs. 14% placebo
- Doses: 0.25–0.5 mg/day starting; titrate to 0.5–3 mg/day (weight-based)
- Side effects: Weight gain (major problem), sedation, hyperprolactinemia, EPS (rare at low doses), metabolic syndrome
Aripiprazole (Abilify)
- FDA-approved for ASD-related irritability in children 6–17 years
- Mechanism: D2 partial agonist + 5-HT1A partial agonist + 5-HT2A antagonist — "stabilizer" profile
- Evidence: Multiple RCTs confirm efficacy
- Advantage over risperidone: Less weight gain, less sedation, less prolactin elevation
- Doses: 2 mg/day start; titrate to 5–15 mg/day
- Side effects: Akathisia (more than risperidone), mild weight gain, sedation, EPS
Comparison: Risperidone vs. Aripiprazole
| Feature | Risperidone | Aripiprazole |
|---|---|---|
| FDA approval | ✓ ASD irritability | ✓ ASD irritability |
| Weight gain | Significant | Moderate |
| Sedation | More sedating | Less sedating |
| Prolactin | Elevated | Not elevated |
| Akathisia | Less | More |
| Metabolic risk | Higher | Lower |
2. HYPERACTIVITY, IMPULSIVITY, INATTENTION (ADHD symptoms)
Methylphenidate (Ritalin, Concerta)
- Evidence: Effective but response rate lower in ASD (~50%) vs. ADHD alone (~75–80%)
- RUPP Autism Network: response rate 49%; also higher adverse effect rate (irritability, stereotypies)
- Doses: Start at 2.5–5 mg/day; lower effective doses in ASD; titrate carefully
- IR or ER formulations
Atomoxetine (Strattera)
- SNRI; non-stimulant ADHD treatment
- Evidence: RCTs show modest but significant benefit for hyperactivity/inattention in ASD
- May be preferred when stimulants cause irritability
- Doses: 0.5 mg/kg/day → 1.2 mg/kg/day
Alpha-2 Agonists
- Guanfacine (Intuniv/Tenex): RCT evidence for hyperactivity, impulsivity in ASD; also helps sleep and tics
- Clonidine: Shorter-acting; also helps sleep; less evidence than guanfacine
3. ANXIETY
SSRIs
- Widely used; fluoxetine has best evidence in ASD-related repetitive behaviors and anxiety
- Sertraline, fluvoxamine: also used
- Caution: ASD children may be more sensitive to activating side effects (agitation, behavioral activation); start at very low doses (e.g., fluoxetine 2.5–5 mg, sertraline 12.5–25 mg)
- Fluvoxamine: sigma-1 receptor agonism may have additional benefits; used in ASD + OCD spectrum
- Evidence mixed for core ASD features; more consistent for comorbid anxiety and repetitive behaviors
Buspirone
- 5-HT1A partial agonist; limited evidence for anxiety and repetitive behaviors in ASD
4. SLEEP — MELATONIN
- Best evidence for any pharmacological sleep intervention in ASD
- Multiple RCTs: reduces sleep onset latency, increases total sleep time
- Dose: 0.5–10 mg, 30 minutes before desired sleep time; start at 0.5–1 mg
- Slow-release melatonin (Slenyto, licensed for ASD in Europe) has strong RCT data
- Generally safe for long-term use; minimal side effects
- Mechanism: ASD may involve impaired endogenous melatonin synthesis
5. SEIZURES
- Treat according to seizure type and EEG findings; standard antiepileptic drugs
- ASD children with seizures need specialist input; some AEDs (valproate, lamotrigine) also have mood-stabilizing properties that may be secondarily beneficial
- Note: Valproate is associated with increased ASD risk when used prenatally — not a contraindication in ASD itself
6. OTHER MEDICATIONS
| Symptom | Drug | Notes |
|---|---|---|
| Self-injurious behavior | Naltrexone | Mixed evidence; may reduce SIB via opioid modulation |
| GI symptoms | Probiotics, dietary management | Evidence limited but improving |
| Anxiety/OCD spectrum | SSRIs, clomipramine | Clomipramine: some evidence for repetitive behaviors; anticholinergic burden limits use |
| Tics | Guanfacine, clonidine; risperidone | ASD commonly co-occurs with tic disorders |
| Aggression (acute) | Lorazepam (short-term) | Crisis management only |
Investigational / Emerging Pharmacological Approaches (2024–2025)
- Oxytocin: Intranasal; plausible mechanism (promotes social bonding); multiple RCTs — results disappointing overall; not recommended routinely
- Bumetanide: GABA modulation (NKCC1 inhibitor); shifts GABA from excitatory to inhibitory in immature neurons; Phase II trials showed some social behavior improvement; not yet approved; diuretic side effects
- mGluR5 antagonists (fragile X research): Targeting glutamate excess; promising in animal models; human trials have been disappointing
- SHANK3-targeting approaches: Gene therapy and targeted molecular interventions in early development — research stage
- D-cycloserine: NMDA partial agonist; small studies suggest benefit for social withdrawal; not in routine use
PART 13 — PROGNOSIS & NATURAL HISTORY
- Higher IQ
- Functional language by age 5
- Early diagnosis and intensive intervention
- Milder symptoms
- Absence of intellectual disability and severe seizure disorder
- ~10% of clearly affected children show substantial improvement approaching normal functioning in longitudinal studies
- Most adults with ASD have ongoing support needs
- Many higher-functioning adults live independently, maintain employment, and relationships
- Autism is lifelong but not static — behavior improves with age, development, and intervention
- Major unmet needs: transition to adult services, employment support, mental health care
PART 14 — RECENT ADVANCES (2023–2026)
-
Diagnostic screening meta-analysis (Santos et al., Clinics 2024, PMID 38484581): M-CHAT-R/F remains the best-validated Level 1 screening tool; ADOS-2 and ADI-R maintain gold standard status for Level 2; no biomarker has yet reached clinical utility.
-
ABA intensity and outcomes (Sandbank et al., JAMA Pediatrics 2024, PMID 38913359): Meta-analysis confirmed that greater ABA treatment intensity (hours/week) is significantly associated with better communication and adaptive behavior outcomes in young autistic children — reinforcing the importance of early intensive intervention.
-
Neuroimaging meta-analysis (Guo et al., Mol Autism 2024, PMID 38576034): Multimodal neuroimaging consistently shows reduced long-range connectivity and local hyper-connectivity — the "underconnectivity" theory of ASD gains structural support. Amygdala, default mode network, and frontal-temporal circuits most affected.
-
Female phenotype recognition: Increased recognition that ASD in females is systematically under-diagnosed due to camouflaging. Diagnostic criteria developed primarily from male cohorts may miss the female presentation. Updated clinical guidance recommends lower thresholds for ASD evaluation in girls.
-
Co-occurring condition prevalence (Micai et al., 2023, PMID 37913872): Largest systematic review of comorbidities confirmed very high rates of ADHD, anxiety, language disorder, and sleep disorders — reinforcing need for comprehensive screening and treatment of co-occurring conditions in all ASD individuals.
-
Slow-release melatonin (Slenyto) evidence: Multiple trials now support slow-release melatonin as the first-line pharmacological intervention for ASD-related insomnia, with strong safety data.
-
Genetics: Whole exome sequencing increasingly used diagnostically; now detecting causative variants in ~10–15% of cases. The "one-to-many" (one gene, many phenotypes) and "many-to-one" (many genes, ASD phenotype) relationships being unraveled.
-
Neurodiversity movement: Increasingly influential in clinical practice — reframing ASD not purely as deficit but as neurological difference. Clinical approach now emphasizes strengths-based assessment, autonomy, and quality of life, not merely symptom reduction.
CLINICAL PEARLS SUMMARY
| Pearl | Detail |
|---|---|
| ASD diagnosis is clinical | No blood test, imaging, or biomarker is diagnostic |
| Screen at 18 and 24 months | M-CHAT-R/F; any regression = immediate referral |
| Ask about regression | 25% of ASD cases show language/social regression between ages 1–2 |
| Joint attention is the key early marker | Absence of pointing to share interest is highly specific for ASD |
| Girls are under-diagnosed | Lower threshold for evaluation; ask about masking |
| Genetic workup in all | Chromosomal microarray + Fragile X testing first-tier |
| Vaccines do NOT cause ASD | Wakefield study was fraudulent; 30+ large studies refute the link |
| Pharmacotherapy targets symptoms, not core | Risperidone/aripiprazole for irritability (FDA-approved); SSRIs for anxiety; melatonin for sleep |
| Start SSRIs very low in ASD | Highly sensitive to activation side effects |
| Early intensive intervention is essential | ABA before age 5, ≥20 hrs/week; outcomes significantly better |
| Comorbidities are the rule | Assess for ADHD, anxiety, sleep, GI, seizures in every patient |
| ASD in adults is underrecognized | Many adults diagnosed late after misdiagnosis with anxiety, depression, personality disorders |
- Kaplan & Sadock's Synopsis of Psychiatry, 12th ed.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, 10th ed.
- Eric Kandel's Principles of Neural Science, 6th ed.
- Tintinalli's Emergency Medicine, 9th ed.
- Katzung's Basic and Clinical Pharmacology, 16th ed.
- Micai et al., Neurosci Biobehav Rev 2023 [PMID 37913872]
- Santos et al., Clinics 2024 [PMID 38484581]
- Guo et al., Mol Autism 2024 [PMID 38576034]
- Sandbank et al., JAMA Pediatrics 2024 [PMID 38913359]
- CASP ABA Practice Guidelines, Version 3, 2024
Mental health care act 2017….in utmost detail…and precision such that i can answer it in viva and write a 20 -30 marks question as a psychiatry resident
Mental Health Care Act 2017 India complete provisions chapters sections psychiatry
Mental Health Care Act 2017 India all chapters sections rights involuntary admission Board
MHCA 2017 India psychiatry viva important sections advance directive mental health review board
https://www.indiacode.nic.in/bitstream/123456789/2249/3/A201…
Mental Health Care Act (MHCA) 2017 — India
Complete Examination Guide for Psychiatry Residents
INTRODUCTION & OVERVIEW
HISTORICAL CONTEXT — FROM MHA 1987 TO MHCA 2017
| Feature | MHA 1987 | MHCA 2017 |
|---|---|---|
| Philosophy | Custodial; safety of society | Rights-based; dignity of person |
| Admission focus | Compulsory detention | Supported admission; least restrictive |
| Legal capacity | Presumed lost in mental illness | Presumed to have capacity always |
| Patient rights | Minimal, paternalistic | Extensive, enforceable |
| Advance directive | Not recognized | Legally recognized |
| Nominated representative | Not present | Explicit provision |
| Right to free treatment | Not guaranteed | Guaranteed (right to access) |
| Mental health authority | State mental health authority (different structure) | Central + State Mental Health Authorities |
| Review Board | Mental Health Review Board (different composition) | Mental Health Review Board (restructured) |
| ECT | Modified and unmodified both allowed | Unmodified ECT banned |
| Suicide | Attempted suicide — criminal offense (Section 309 IPC) | Decriminalized (presumed severe stress) |
CHAPTER I — PRELIMINARY (Sections 1–5)
Key Definitions (Section 2)
Exam point: Intellectual disability/mental retardation is explicitly excluded from the definition of mental illness.
CHAPTER II — MENTAL HEALTH POLICY, PLAN, PROGRAMME (Sections 6–8)
- Central and State Governments must formulate mental health policies, programmes, and plans to provide mental health services
- Services must be at all levels of the general health care system (not segregated)
- State Governments must ensure community-based treatment as far as possible
CHAPTER III — RIGHTS OF PERSONS WITH MENTAL ILLNESS (Sections 18–28)
Section 18 — Right to Access Mental Health Care
- Mental health care and treatment from government-run or government-funded mental health services
- Affordable, good quality, geographically accessible mental health services
- Equality of treatment at par with physical illness in all healthcare facilities
Section 19 — Right to Community Living
- Every person with mental illness shall live in community, in their family, or in a family-like setting
- Can only be separated from family if care in community is not possible and person gives consent or Board authorizes
Section 20 — Right to Protection from Cruel Treatment
- No person with mental illness shall be subjected to cruel, inhuman, degrading treatment
- No physical restraint except in therapeutic emergencies; documented; never punitive
- No seclusion unless all other methods exhausted; maximum 24 hours at a time
Section 21 — Right to Equality and Non-Discrimination
- Right to live with dignity
- No discrimination on grounds of mental illness in matters of employment or education
- Emergency medical care must not be denied on grounds of mental illness
Section 22 — Right to Information
- Right to know diagnosis, treatment plan, risks/benefits
- Right to receive information in a language/manner understood
- Right to have all records
Section 23 — Right to Confidentiality
- Full confidentiality of mental health history; cannot be disclosed without consent
- Exceptions: in interest of person's safety; in interest of others' safety; in public interest (court order)
Section 24 — Right to Access Medical Records
- Entitled to access all records
- Can nominate a person to receive records on their behalf
Section 25 — Right to Personal Contacts and Communication
- Right to communicate with family, friends, nominated representative, legal representative, Inspector General of Prisons, Mental Health Review Board
- Cannot be denied
Section 26 — Right to Legal Aid
- Right to free legal services under Legal Services Authorities Act
Section 27 — Right to Make Complaints
- Right to make complaints about deficiencies in mental health services to Central/State Mental Health Authority
Section 28 — Rights Applicable to Homeless Persons
- Homeless persons with mental illness shall not be denied any rights under the Act
CHAPTER IV — ADVANCE DIRECTIVE (Sections 5–12)
This is the most novel and frequently examined section of the Act.
Section 5 — Making an Advance Directive
- Any person who is NOT currently admitted to a mental health establishment and has capacity can make an advance directive
- Specifies how to be cared for and how NOT to be cared for during a mental illness episode
- Specifies the nominated representative
Format Requirements:
- Must be in writing
- Signed by the person with two witnesses
- Counter-signed by a magistrate (to prevent forgery/coercion)
- May also be registered
Section 6 — Content of Advance Directive
- Medications that can be given
- Medications that cannot be given
- Other treatment that can be given
- Other treatment that cannot be given
- Where to be treated (facility, home)
- Who should be informed
- Name of nominated representative
Section 7 — Nominated Representative
- The person specifies who should act on their behalf when they lack capacity
- Must be an adult (18+)
- Must consent to be the nominated representative
- Takes precedence over family members
- Spouse (if not separated)
- Parent
- Major sibling
- Major other relative
- In case of minor: guardian/parent
- If no one available: Board appoints
Section 8 — Revocation/Amendment of Advance Directive
- Can be revoked, amended, or cancelled at any time when the person has capacity
- Same formalities as making it
Section 9 — Review of Advance Directive
- Mental health professional treating the person must review the directive
- Can apply to Board to review if they believe it is inconsistent with the person's best interests
- Board can override the directive in a specific situation if it finds: (a) the person did not have capacity when making it, (b) the directive was fraudulently made, (c) following it would cause serious harm to the person or others
Exam Points on Advance Directives:
- Valid only if made when person has capacity
- Protects against both over-treatment and under-treatment
- Unique to MHCA 2017 — did not exist in MHA 1987
- Mental health professional CANNOT override it unilaterally — must go to Board
- Patient can nominate specific hospital, specific drugs, or refuse specific drugs (e.g., "I do not want ECT")
CHAPTER V — CENTRAL MENTAL HEALTH AUTHORITY (CMHA) (Sections 33–45)
Composition (Section 33):
- Chairperson: Secretary, Ministry of Health and Family Welfare (or designated officer)
- Members:
- At least 3 qualified medical practitioners in psychiatry
- At least 1 person who has been a person with mental illness (by experience)
- At least 1 representative of a non-governmental organization working for persons with mental illness
- Surgeon General/Director General Health Services
- Additional Secretary, Law/Legal Affairs Ministry
- Additional Secretary, Social Justice Ministry
- Representative from National Human Rights Commission
- Representative from National Medical Commission
Functions of CMHA (Section 43):
- Maintain central register of all mental health establishments
- Develop quality and service provision standards
- Register/regulate psychiatrists and mental health professionals
- Collect/maintain data on mental health establishments
- Develop manuals, protocols, and guidelines
- Train mental health professionals
- Receive and respond to grievances from persons with mental illness
- Publish and disseminate mental health information
- Develop minimum standards for residential facilities
CHAPTER VI — STATE MENTAL HEALTH AUTHORITY (SMHA) (Sections 45–55)
Composition (Section 45):
- Chairperson: Secretary in charge of Health (State Government) — or equivalent
- Members include:
- At least 3 medical practitioners in psychiatry
- 1 person with experience of mental illness
- 1 NGO representative
- Representatives from State Departments: Health, Social Justice, Education, Finance
- At least 2 mental health professionals from non-medical disciplines
Functions (Section 55):
- Register, regulate, supervise all mental health establishments in the state
- Maintain state register
- Ensure compliance with standards
- Receive and address complaints
- Inspect mental health establishments
- Fund and support mental health programs
CHAPTER VII — MENTAL HEALTH REVIEW BOARDS (MHRB) (Sections 73–98)
One of the most important operational bodies — frequently examined.
Establishment (Section 73):
- State Government shall establish one or more MHRBs for each district
- District-level bodies
Composition (Section 73):
- District Judge or additional district judge (Chairperson)
- At least 2 psychiatrists
- At least 1 person who has/had mental illness
- At least 1 person representing civil society (nominated by State Government)
- Total: minimum 5 members
Functions of MHRB (Section 74):
- Register, review, and update advance directives
- Appoint nominated representatives
- Adjudicate complaints regarding advance directives
- Review orders for admission/treatment without consent (Section 90–92)
- Review long-term supported admission orders (beyond 30 days)
- Receive and dispose applications for admission review
- Order discharge
- Visit and inspect mental health establishments
- Perform such other functions as prescribed
Periodic Review of Admissions (Section 86):
- Any person admitted must be reviewed by MHRB at intervals of 90 days initially
- After continued admission, every 6 months
CHAPTER IX — ADMISSION, TREATMENT, AND DISCHARGE (Sections 85–98)
Most clinically critical chapter for day-to-day psychiatry practice.
Types of Admission Under MHCA 2017:
ADMISSION
├── INDEPENDENT ADMISSION (Section 85)
│ └── Person has capacity and consents → voluntary
│
├── SUPPORTED ADMISSION (Section 86)
│ ├── Without capacity + nominated representative consents
│ └── OR person lacks capacity and no representative
│
└── SUPPORTED ADMISSION — SPECIAL CIRCUMSTANCES (Section 90)
└── Emergency or high-risk situations
Section 85 — Independent Admission (Voluntary)
- Person with mental illness who has capacity can apply for admission themselves
- Must be given information about their rights, treatment plan
- Can leave at any time — giving 72 hours' notice in writing
- During the 72 hours, the treating psychiatrist can apply to MHRB to extend the admission
- If person is a minor — parent/guardian applies
Section 86 — Supported Admission (Formerly "Voluntary" for those lacking capacity)
- If person lacks capacity: nominated representative (NR)
- If no NR: relatives (spouse > parent > sibling > relative)
- May also be on basis of assessment by the treating psychiatrist
- The person has a mental illness
- The person lacks capacity to make admission decision
- The person requires in-patient treatment
- Admission is in the best interest of the person
- The treating psychiatrist supports the admission
- Application to the medical officer/psychiatrist in charge of establishment
- Must be in prescribed form
- If the person is distressed or shows physical resistance → cannot proceed without MHRB review
- Initial period: 30 days
- Review by MHRB at 30 days — can extend for up to 90 more days
- After 90 days — fresh MHRB order needed every 90 days
- NR can apply for discharge at any time
- Treating psychiatrist can discharge
- If psychiatrist refuses discharge despite NR request → MHRB reviews within 7 days
Section 87 — Admission on Application by Relative or Care Giver
- Application can be made by relative or care-giver when:
- Person appears to have mental illness
- Is likely to harm themselves or others, OR is incapacitated
- Is unable to get treatment
- Must be supported by a medical certificate from a registered medical practitioner
- Leads to assessment within 24 hours by a psychiatrist
Section 89 — Duties of Medical Officer on Admission
- Inform patient of their rights (verbally and in writing)
- Inform nominated representative
- Inform nearest relative if no NR
- Record the admission in the register
Section 90 — Admission and Treatment of Persons with High Support Needs Without Consent (Emergency Admission)
- Person has (or is suspected to have) mental illness
- Poses imminent danger to themselves or others
- There is no time for supported admission procedure
- Registered medical practitioner (any) → initial assessment
- Must call a psychiatrist within 24 hours
- If psychiatrist confirms criteria → can extend up to 7 days for assessment and treatment
Section 92 — Discharge
- Treating psychiatrist shall discharge when criteria for admission are no longer met
- Discharge plan must be prepared including:
- Aftercare plan
- Follow-up plan
- Information to family
- Community support
CHAPTER X — SPECIAL PROVISIONS FOR MINORS (Sections 83–84)
- Minor = person under 18 years
- A minor cannot be admitted to a mental health establishment in a ward for adults
- Must be in a separate ward or a facility specifically for minors
- All admissions require consent of parent or guardian
- All rights under the Act apply to minors; their views are to be given weight as per age and maturity
CHAPTER XI — MENTAL HEALTH ESTABLISHMENT STANDARDS (Sections 65–73)
Registration:
- Every mental health establishment must be registered with the SMHA
- Application in prescribed form
- Certificate of registration valid for 5 years, renewable
Minimum Standards (Section 66 and Rules):
- Adequate and appropriate indoor and outdoor spaces
- Clean drinking water and sanitary facilities
- Individual privacy
- Separate accommodation for males and females
- Adequate food and clothing
- Recreational activities
- Access to legal aid
- Safeguards against abuse
Section 68 — Annual Report:
CHAPTER XII — RESPONSIBILITY OF OTHER AGENCIES (Sections 99–106)
Prisoners (Section 103):
- If any prisoner appears to have mental illness → medical officer shall report to Magistrate
- Magistrate may order examination by two psychiatrists
- If confirmed → may be transferred to a mental health establishment
Section 104 — Mentally Ill Offenders in Courts:
- If a person before a criminal court appears to have mental illness → court may order psychiatric examination
- If confirmed → court may order treatment before or instead of criminal proceeding
Section 105 — Homeless Persons:
- A police officer or any magistrate may take cognizance of a homeless person who appears to have mental illness
- Can be sent to a government mental health establishment for assessment
CHAPTER XIII — DECRIMINALIZATION OF ATTEMPTED SUICIDE (Section 115)
This is one of the most important and most asked sections in viva.
Impact:
- Does not repeal Section 309 IPC entirely — it creates a presumption
- The burden of proof shifts: the state must prove the attempt was not from severe stress to proceed with prosecution
- In effect: virtually eliminates criminal prosecution for attempted suicide
- Government must provide care, treatment, and rehabilitation to such persons
- Police are instructed not to harass such persons
Section 309 IPC (for context):
CHAPTER XIV — ELECTROCONVULSIVE THERAPY (ECT) — Section 94
Banned provision — always asked in viva.
Section 94:
- Modified ECT (with general anaesthesia and muscle relaxants) remains permitted
- ECT in minors is prohibited unless in emergency and approved by MHRB
- ECT on pregnant women — permitted with consent and opinion of two psychiatrists
- ECT cannot be given without consent unless under Section 94 emergency provisions with specific oversight
Historical context:
- MHA 1987: Allowed both modified and unmodified ECT
- MHCA 2017: Only modified ECT permitted
- In India, unmodified ECT was commonly practiced due to resource constraints; MHCA 2017 effectively ended this practice
CHAPTER XV — HUMAN RIGHTS (Sections 107–115)
Section 108 — Right to Inspection:
- State Government must designate an Inspector for mental health establishments
- Inspector can enter, inspect, examine records
- Must submit annual report to SMHA and Central Government
Section 110 — Penalty for Operating Without Registration:
- Imprisonment: up to 6 months
- Fine: up to ₹5,000 (for each day of default)
- Both
Section 111 — Offences by Companies:
- If a company is guilty of an offence, the person in charge (director, officer) is personally liable
Section 113 — Protection of Action Taken in Good Faith:
- No legal proceedings against Government officer or mental health professional for anything done in good faith under the Act
CHAPTER XVI — MISCELLANEOUS (Sections 116–126)
Section 117 — State Mental Health Care Rules:
Section 121 — Act Overrides Other Laws:
KEY COMPARISONS FOR VIVA
MHCA 2017 vs. UNCRPD Alignment
| UNCRPD Principle | MHCA 2017 Provision |
|---|---|
| Equal recognition before the law (Article 12) | Presumption of capacity; advance directive; legal capacity preserved |
| Liberty and security (Article 14) | Conditions for supported admission; MHRB review; 72-hour notice |
| Freedom from torture (Article 15) | Ban on cruel treatment; ban on unmodified ECT |
| Right to independent living (Article 19) | Right to community living (Section 19) |
| Right to health (Article 25) | Right to access mental health care (Section 18) |
| Access to justice (Article 13) | Right to free legal aid (Section 26) |
Types of Admission — Quick Reference
| Type | Section | Capacity | Consent | Who applies | Max initial | Review |
|---|---|---|---|---|---|---|
| Independent | 85 | Has capacity | Self | Person themselves | No limit | 72-hr notice to leave |
| Supported | 86 | Lacks capacity | NR/relative | NR/relative | 30 days | MHRB at 30 days, then 90 days |
| Emergency (high support needs) | 90 | Any | Not required | Registered medical practitioner | 7 days | Must convert to Sec 86 or discharge |
| Court-ordered | 104 | Any | Not required | Court | Per court order | MHRB |
CRITICISMS AND LIMITATIONS OF MHCA 2017
-
Infrastructure gap: Rights cannot be realized without community mental health services, which are severely deficient in India. The Act mandates rights but not resources.
-
Definitional tension: The definition of mental illness excludes intellectual disability — problematic as many individuals with ID need mental health protections.
-
Advance directive practical limitations: Requirement of magistrate countersignature is cumbersome; many patients in rural areas cannot access magistrates.
-
MHRB establishment delays: Many districts still do not have functioning MHRBs.
-
Section 309 IPC not fully repealed: Still technically on the books — creates confusion for law enforcement.
-
Nominated representative vs. family: May create conflict between NR and family; no clear dispute resolution mechanism beyond MHRB.
-
ECT for minors: Prohibition unless emergency is seen by some clinicians as potentially harmful in cases where ECT might be genuinely indicated in adolescents.
-
Overrides clinical judgment in some areas: Critics argue advance directives can be used to refuse clearly life-saving treatment.
-
AYUSH integration: The Act includes AYUSH practitioners in mental health establishments — controversial, as they may lack training.
-
Private sector regulation: Implementation in private hospitals and nursing homes remains weak.
VIVA QUESTIONS — PREDICTED AND ANSWERS
MODEL 20-MARK LONG ANSWER
Introduction (2 marks)
Definitions (2 marks)
Rights of Persons with Mental Illness (4 marks)
- Section 18: Right to access mental health care from government services, at par with physical illness
- Section 19: Right to live in the community; separation only with consent or MHRB authorization
- Section 20: Protection from cruel, inhuman, degrading treatment; no punitive restraint; seclusion max 24 hours
- Section 21: Non-discrimination; emergency care cannot be denied
- Section 22: Right to information about diagnosis and treatment
- Section 23: Right to confidentiality of mental health records
- Section 25: Right to communicate with family, representative, legal counsel, and MHRB
- Section 26: Right to free legal aid
Advance Directive (4 marks)
Types of Admission (4 marks)
- Independent Admission (Section 85): For persons with capacity who consent; can leave after 72 hours' notice.
- Supported Admission (Section 86): For persons lacking capacity; nominated representative or relative applies; initial 30 days; MHRB reviews and can extend by 90 days at a time.
- Emergency Admission (Section 90): For imminent danger; authorized by any registered medical practitioner; psychiatric assessment within 24 hours; maximum 7 days; must then convert to supported admission or discharge.
Decriminalization of Attempted Suicide (2 marks)
ECT (Section 94) (1 mark)
MHRB — Composition and Functions (2 marks)
Comparison with MHA 1987 (1 mark)
Conclusion
SUMMARY MNEMONICS
- Access to mental health care
- Community living
- Information about treatment
- Dignity (protection from cruel treatment)
- Equality (non-discrimination)
- Confidentiality
- Legal aid
- Right to complain
- Independent (capacity, self-consent)
- Supported (no capacity, NR consent, 30 days)
- Emergency (danger, no consent needed, 7 days)
- Signed
- Witnesses (two)
- Magistrate countersignature
- Capacity at time of making