BPH in simple language for university exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent content from multiple authoritative sources. Let me compile a comprehensive, exam-ready answer.
Benign Prostatic Hyperplasia (BPH) - University Exam Notes
What is BPH?
BPH is the non-cancerous enlargement of the prostate gland due to overgrowth of both the glandular (epithelial) and stromal (fibromuscular) components. It is the most common benign disease of the male urinary tract and one of the most common conditions treated by urologists.
- Normal prostate in young men: ~20 mL
- In BPH: volume exceeds 30 mL (can reach 60-100 g, a 3- to 5-fold increase)
- "Benign" means it does NOT spread or become cancer
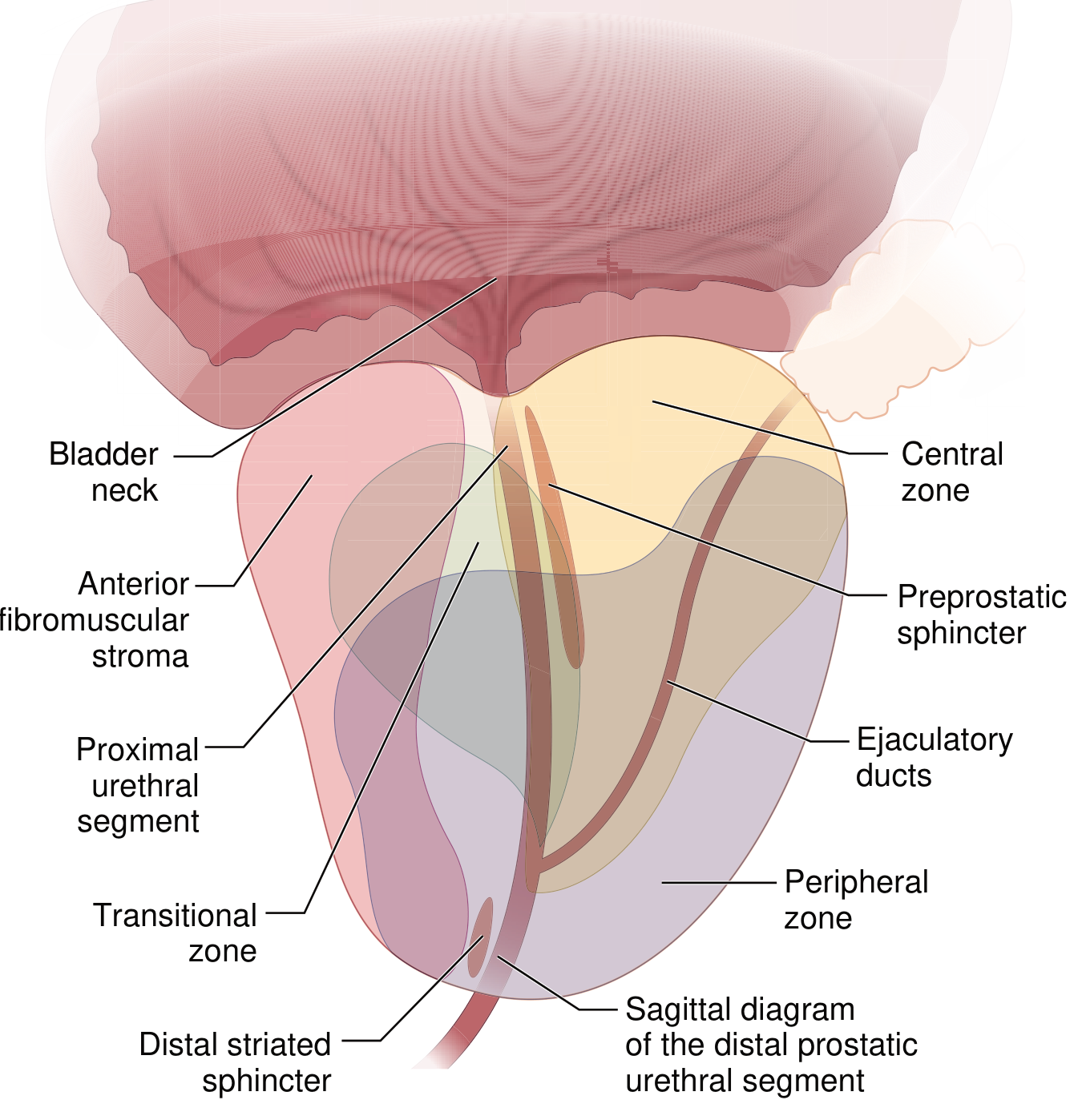
Anatomy Reminder
The prostate has 4 zones: peripheral, central, transitional, and fibromuscular stroma. BPH arises specifically in the transitional zone (periurethral zone) - this is why it squeezes the urethra. Prostate cancer, by contrast, typically arises in the peripheral zone.
Epidemiology
| Age group | Prevalence of histological BPH |
|---|---|
| >50 years | ~50% |
| 60-69 years | ~70% |
| 80s | ~90% |
Of those with histological BPH, ~50% will develop symptomatic lower urinary tract symptoms (LUTS).
Key point: BPH is an age-related disease. It does NOT occur in men castrated before puberty or in men with conditions that block androgen action.
Pathogenesis (Why Does It Happen?)
The key hormone is Dihydrotestosterone (DHT):
- Circulating testosterone enters prostate cells
- The enzyme 5α-reductase type 2 converts testosterone → DHT
- DHT is 10× more potent than testosterone
- DHT binds nuclear androgen receptors → stimulates stromal cell proliferation and prevents epithelial cell death
Aging factor: As men age, testosterone levels fall but estrogen levels remain stable (or rise due to peripheral conversion). Estrogens act synergistically with DHT to further drive growth - both stromal and epithelial cells express estrogen receptors.
Think of it as: Too much DHT + estrogen effect = overgrowth of the prostate's inner (transitional) zone → squeezes the urethra like a fist squeezing a garden hose.
Pathology (What Does It Look Like?)
Gross:
- Prostate weight 60-100 g (normal ~20 g)
- Hyperplastic nodules seen on cross-section - may be solid or cystic
- Urethra compressed to a slit-like orifice
Microscopic:
- Nodules made of variable proportions of glands + fibromuscular stroma
- Hyperplastic glands lined by two cell layers: tall columnar inner cells + flattened basal outer cells (KEY exam point - this distinguishes BPH from prostate carcinoma, which lacks the basal cell layer)
- Glandular lumina may contain corpora amylacea (laminated protein secretions)
Symptoms (LUTS - Lower Urinary Tract Symptoms)
BPH causes symptoms through two mechanisms:
- Mechanical obstruction - the enlarged gland physically compresses the urethra
- Dynamic obstruction - smooth muscle in the prostate contracts, further narrowing the urethra
Symptoms are divided into three groups:
Voiding (Obstructive) Symptoms
- Hesitancy (difficulty starting urination)
- Weak/poor urine stream
- Straining to void
- Prolonged voiding time
- Overflow dribbling
Storage (Irritative) Symptoms
- Urinary frequency (needing to go often)
- Urgency (sudden strong need to urinate)
- Nocturia (waking at night to urinate)
- Dysuria (painful urination)
Post-void Symptoms
- Feeling of incomplete bladder emptying
- Post-void dribbling
Exam note: Prostate size does NOT reliably correlate with severity of symptoms.
Complications (if untreated)
| Complication | Mechanism |
|---|---|
| Bladder hypertrophy | Bladder muscle works harder against obstruction |
| Residual urine (incomplete emptying) | Increased infection risk (UTIs) |
| Acute urinary retention | Complete obstruction |
| Hydronephrosis | Back-pressure on kidneys from chronic obstruction |
| Recurrent UTIs (bladder + kidney) | Stagnant urine = bacterial culture medium |
Diagnosis
- History - LUTS symptoms, symptom scoring (International Prostate Symptom Score, IPSS)
- Digital Rectal Exam (DRE) - prostate feels smooth and rubbery (unlike the hard, irregular feel of cancer)
- Urinalysis - rule out infection
- PSA (Prostate-Specific Antigen) - used in patients with >10-year life expectancy; BPH can mildly raise PSA
- Post-void residual urine volume - measured by bladder ultrasound
- Uroflowmetry - measures urine flow rate
- Cystoscopy / Urodynamics - if initial evaluation is inconclusive
Treatment
Step 1 - Watchful Waiting + Lifestyle Changes
For mild symptoms. Reduce evening fluid intake, limit caffeine and alcohol, bladder training.
Step 2 - Medical Therapy
| Drug Class | Examples | Mechanism | Side Effects |
|---|---|---|---|
| α1-blockers | Tamsulosin, Alfuzosin, Doxazosin | Relax smooth muscle in prostate/bladder neck → reduce outflow resistance | Dizziness (orthostasis), retrograde ejaculation, rhinitis |
| 5α-reductase inhibitors | Finasteride, Dutasteride | Block testosterone → DHT conversion → shrink prostate over months | Reduces serum PSA by ~50% (important for cancer screening interpretation), sexual side effects |
| Combination | α1-blocker + 5α-RI | Synergistic effect, best for large prostates | Combined side effects |
| Muscarinic antagonists | Oxybutynin | Target overactive bladder/storage symptoms | Dry mouth, constipation |
Key exam point: 5α-reductase inhibitors work slowly (months) but actually shrink the gland; α1-blockers work fast but only relax muscle without shrinking the gland.
Step 3 - Surgical / Minimally Invasive (for refractory cases)
- TURP (Transurethral Resection of the Prostate) - the gold standard surgery; "reaming out" the inner gland through a scope
- Laser therapy (HoLEP, GreenLight laser)
- HIFU (High-Intensity Focused Ultrasound)
- Transurethral electrovaporization
- Radiofrequency ablation
- Simple open prostatectomy - for very large glands (>100 g)
BPH vs Prostate Cancer - Key Differences (High-Yield Exam Table)
| Feature | BPH | Prostate Cancer |
|---|---|---|
| Zone of origin | Transitional zone | Peripheral zone |
| Nature | Benign (non-invasive) | Malignant |
| DRE | Smooth, rubbery, enlarged | Hard, irregular nodule |
| PSA | Mildly elevated | Often significantly elevated |
| Histology | Two cell layers (columnar + basal) | Lacks basal cell layer |
| Treatment goal | Symptom relief | Cure / disease control |
Quick Summary for Revision
- What: Non-cancerous enlargement of prostate (transitional zone)
- Who: Men >50, incidence rises with age
- Why: DHT (from testosterone via 5α-reductase) + estrogen in older men
- Where: Transitional zone → compresses urethra → LUTS
- Symptoms: Hesitancy, weak stream, frequency, nocturia, incomplete emptying
- Diagnose: IPSS score, DRE, PSA, flow rate, post-void residual
- Treat: Lifestyle → α1-blockers / 5α-RI → TURP if needed
Sources: Robbins & Kumar Basic Pathology, 10th ed.; Goldman-Cecil Medicine; Sabiston Textbook of Surgery, 27th ed.; Campbell Walsh Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.