2nd MBBS Pathology - MUHS Exam Notes
Source: Robbins & Kumar Basic Pathology + Robbins, Cotran & Kumar Pathologic Basis of Disease
Q1. FIBROID UTERUS (Uterine Leiomyoma)
Definition
A leiomyoma (fibroid) is a benign smooth muscle tumor (leiomyoma) arising from the myometrium. It is the most common benign tumor of the female genital tract and the most common uterine tumor in women of reproductive age.
Pathogenesis / Etiology (Exam Points)
| Factor | Details |
|---|
| Hormonal dependence | Estrogen and progesterone stimulate growth; tumors shrink after menopause |
| MED12 gene mutation | Present in up to 70% of leiomyomas; encodes a regulator of RNA Polymerase II |
| Chromosomal abnormalities | Rearrangements of chromosomes 6 and 12 |
| Risk factors | Obesity, early menarche, African American women (more common + larger) |
| FH gene (Fumarate Hydratase) | Germline loss-of-function mutations → autosomal syndrome with multiple cutaneous + uterine leiomyomas + renal cell carcinoma |
Classification by Location (FIGO System)
UTERINE CAVITY
┌─────────────────────────────┐
│ ┌──────────────────────┐ │
Submucosal──► │ Intramural │ ◄── Subserosal
(Type 0,1,2)│ │ (within wall) │ │ (under serosa)
│ └──────────────────────┘ │
└─────────────────────────────┘
▼
Parasitic (pedunculated subserosal
attached to adjacent organs)
- Type 0 - Intracavitary (pedunculated submucosal, entirely within cavity)
- Type 1 - <50% diameter within myometrium (submucosal)
- Type 2 - ≥50% diameter within myometrium (submucosal)
- Type 3 - Abuts endometrium, no intracavitary component (intramural)
- Type 4-6 - Intramural
- Type 7 - Subserosal (pedunculated)
- Type 8 - Other (cervical, parasitic)
GROSS PATHOLOGY (High-yield exam point)
GROSS FEATURES OF LEIOMYOMA
─────────────────────────────────────────────
• Single or multiple (most often multiple)
• Sharply circumscribed / well demarcated
• Firm, rubbery consistency
• Gray-white to pinkish-white color
• Cut surface: WHORLED / TRABECULATED appearance ★
• Variable size: few mm to very large (can fill pelvis)
• Pseudocapsule present (can be shelled out)
• Locations: intramural > submucosal > subserosal
─────────────────────────────────────────────
Degenerative Changes (Secondary changes seen on gross / clinically):
| Type | Gross Appearance | Notes |
|---|
| Hyaline degeneration | White, homogeneous areas | Most common |
| Cystic degeneration | Fluid-filled spaces | Follow hyaline degeneration |
| Calcification | Gritty/hard areas | Post-menopausal women ("womb stones") |
| Red degeneration (Carneous) | Red, beef-like appearance | During pregnancy - infarction |
| Fatty degeneration | Yellow areas | Rare |
| Myxoid degeneration | Gelatinous areas | Rare |
| Sarcomatous change | Soft, hemorrhagic, necrotic | Extremely rare (<0.5%) |
MICROSCOPIC (HISTOPATHOLOGY) (Exam diagram point)
HISTOLOGY OF LEIOMYOMA
────────────────────────────────────────────────────
• Bundles/fascicles of smooth muscle cells
• Cells: elongated spindle-shaped with:
- Abundant eosinophilic cytoplasm
- Cigar-shaped (blunt-ended) nuclei ★
- No/rare mitoses (<5 per 10 HPF)
- No nuclear atypia
• Cells arranged in INTERLACING FASCICLES ★
• Connective tissue stroma between bundles
• Foci of FIBROSIS, CALCIFICATION may be present
• Well-defined border from surrounding myometrium
────────────────────────────────────────────────────
Key Histological Diagram Description:
┌─────────────────────────────────────┐
│ Smooth muscle cells in fascicles │
│ ═══════════════════════════════ │
│ ─────────────────────────────── │
│ ═══════════════════════════════ │
│ (interlacing pattern seen) │
│ ○ Cigar-shaped nuclei │
│ Fibrous stroma between bundles │
└─────────────────────────────────────┘
Well-circumscribed, pseudocapsule
(Source: Robbins & Kumar Basic Pathology, Chapter 17)
COMPLICATIONS (★ Very Important for MUHS)
COMPLICATIONS OF UTERINE FIBROIDS
─────────────────────────────────────────────────
MENSTRUAL:
• Menorrhagia (most common symptom) ★
• Metrorrhagia, dysmenorrhea
REPRODUCTIVE:
• Infertility (distortion of cavity)
• Recurrent abortions
• Malpresentation in pregnancy
• Obstructed labour
• Red degeneration in pregnancy (pain)
PRESSURE EFFECTS:
• Urinary frequency/retention (bladder compression)
• Constipation (rectal compression)
• Hydronephrosis (ureteric compression)
• Venous thrombosis (large tumors)
TORSION: Pedunculated fibroid can twist → acute abdomen
MALIGNANT TRANSFORMATION:
• Leiomyosarcoma - EXTREMELY RARE (<0.5%) ★
(Not from leiomyoma → arises de novo in postmenopausal)
─────────────────────────────────────────────────
Q2. GERM CELL TUMORS OF OVARY
Definition
Tumors arising from the germ cells (primitive sex cells) of the ovary. They constitute 15-20% of all ovarian tumors.
Classification (Must-Know for MUHS)
GERM CELL TUMORS OF OVARY
│
├── A. TUMORS OF GERM CELLS THEMSELVES
│ ├── 1. Dysgerminoma ★ (most common malignant GCT)
│ └── 2. Gonadoblastoma
│
├── B. TUMORS SHOWING EMBRYONIC DIFFERENTIATION
│ └── Teratoma
│ ├── Mature (Benign) Teratoma / Dermoid Cyst ★
│ ├── Immature (Malignant) Teratoma
│ └── Monodermal Teratoma (Struma ovarii, Carcinoid)
│
└── C. TUMORS SHOWING EXTRA-EMBRYONIC DIFFERENTIATION
├── Yolk Sac Tumor (Endodermal Sinus Tumor) ★
├── Choriocarcinoma (Primary ovarian)
└── Embryonal Carcinoma
Note: Mixed germ cell tumors (containing combinations) also occur.
DYSGERMINOMA (High-yield MUHS topic)
Definition
Dysgerminoma is the ovarian counterpart of testicular seminoma. It is the most common malignant germ cell tumor of the ovary.
Epidemiology (Exam points)
| Feature | Detail |
|---|
| Incidence | ~2% of ovarian cancers; ~50% of malignant GCTs |
| Age group | 2nd and 3rd decades; 75% in age 10-30 years |
| Gonadal dysgenesis | Associated with pseudohermaphroditism, gonadal dysgenesis |
| Hormonal activity | Most are non-functional |
| Rare cases | Elevated hCG (due to syncytiotrophoblastic giant cells) |
Molecular / Genetics (★ Exam)
- Expresses stem cell markers: OCT3, OCT4, NANOG (pluripotency markers)
- Associated with isochromosome 12p (i12p) - same as testicular seminoma
- KIT receptor tyrosine kinase expressed; 30-50% have activating KIT mutations ★
- 30% have amplification of KIT
GROSS PATHOLOGY of Dysgerminoma
GROSS FEATURES
───────────────────────────────────────────
• Unilateral in 80-90% ★
• Large tumors - may fill the abdomen
• Solid tumor ★ (NOT cystic)
• Cut surface: Yellow-white to GRAY-PINK ★
• Soft, FLESHY consistency ★
• May have areas of necrosis in large tumors
• Smooth, lobulated external surface
───────────────────────────────────────────
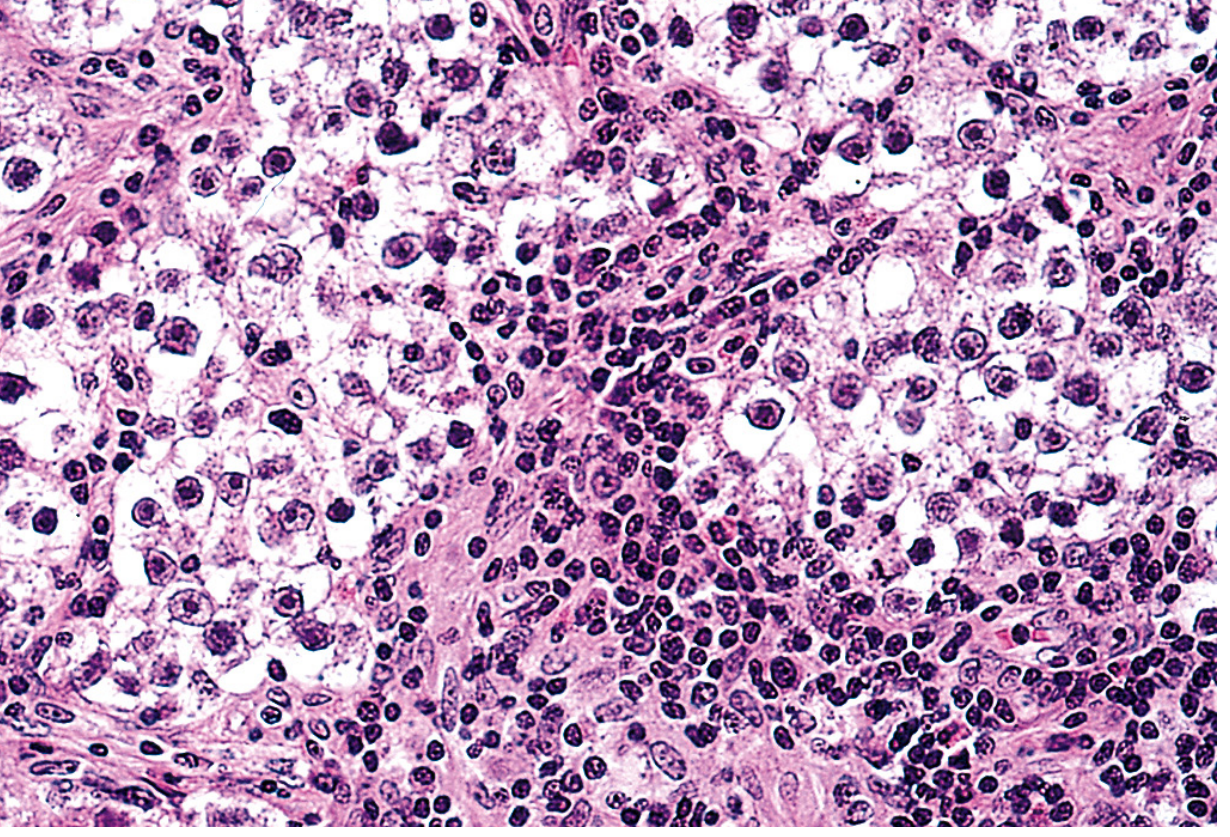
MICROSCOPIC (HISTOPATHOLOGY) of Dysgerminoma
Classic description (must write in exam):
HISTOLOGY OF DYSGERMINOMA
────────────────────────────────────────────────────
• Large VESICULAR cells (polyhedral/round) ★
• Clear cytoplasm ★
• Well-defined cell boundaries
• Centrally placed REGULAR NUCLEI ★
• Prominent nucleoli
• Cells arranged in SHEETS or CORDS ★
• Separated by SCANT FIBROUS STROMA
• Stroma infiltrated by LYMPHOCYTES ★ (key feature!)
• Non-caseating granulomas may be present
• Occasional syncytiotrophoblastic giant cells (hCG +ve)
────────────────────────────────────────────────────
Exam Diagram - Dysgerminoma Histology:
Fig: Dysgerminoma - large vesicular cells with clear cytoplasm, round nuclei, and lymphocytic stromal infiltrate (H&E). Source: Robbins, Cotran & Kumar Pathologic Basis of Disease
Prognosis of Dysgerminoma
- All dysgerminomas are malignant but behavior is variable
- Only ~1/3 are aggressive
- Unilateral tumor without capsular breach: >90% 10-year PFS after salpingo-oophorectomy
- Highly radiosensitive and chemosensitive ★
- Even metastatic disease can often be cured
Q3. TERATOMA
Definition
A teratoma is a germ cell tumor composed of tissue elements derived from two or three embryonic germ layers (ectoderm, mesoderm, endoderm) that are foreign to the anatomical site where the tumor arises.
Key concept: Teratomas contain tissues NOT normally found at the site of origin - they can contain teeth, hair, cartilage, neural tissue, thyroid, etc.
Classification of Teratoma (Most Important)
TERATOMA CLASSIFICATION
│
├── 1. MATURE (BENIGN) TERATOMA ★★
│ ├── Mature Cystic Teratoma (Dermoid Cyst) - MOST COMMON
│ └── Mature Solid Teratoma (rare)
│
├── 2. IMMATURE (MALIGNANT) TERATOMA ★
│ └── Graded I, II, III based on amount of immature neuroepithelium
│
└── 3. MONODERMAL (HIGHLY SPECIALIZED) TERATOMA ★
├── Struma Ovarii (composed entirely of thyroid tissue)
└── Carcinoid Tumor (from intestinal tissue in teratoma)
└── Strumal Carcinoid (rare combination)
A. MATURE (BENIGN) TERATOMA (Dermoid Cyst) (Most common GCT of ovary)
Gross Pathology (Exam Diagram)
GROSS - MATURE CYSTIC TERATOMA (DERMOID CYST)
──────────────────────────────────────────────────
• Most common ovarian GCT
• Usually UNILOCULAR CYST ★
• Bilateral in 10-15% of cases ★
• Contains HAIR and SEBACEOUS material ★
• Cut surface:
- Cyst wall lined by opaque, GRAY-WHITE, WRINKLED epidermis
- PROTRUDING HAIR SHAFTS ★
- TOOTH structures and CALCIFICATION visible grossly ★
- Sebaceous (greasy/cheesy) material fills cyst
• Rokitansky's protuberance (dermoid plug) - solid nodule on cyst wall
──────────────────────────────────────────────────
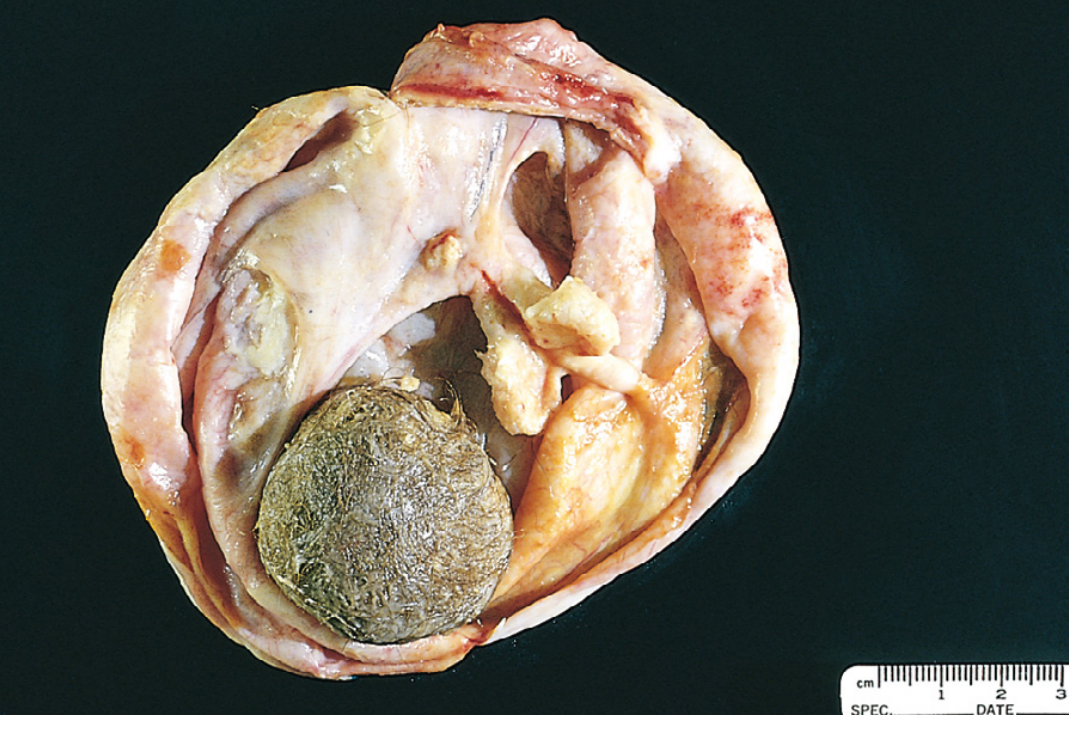
GROSS IMAGE - Mature Cystic Teratoma (Dermoid Cyst):
Fig 22.36: Opened mature cystic teratoma (dermoid cyst). Hair (bottom) and a mixture of tissues are evident. Source: Robbins, Cotran & Kumar Pathologic Basis of Disease
Microscopic Pathology of Mature Teratoma (Exam Diagram)
HISTOLOGY - MATURE CYSTIC TERATOMA
──────────────────────────────────────────────────────
CYST WALL: Lined by STRATIFIED SQUAMOUS EPITHELIUM ★
SKIN ADNEXA (ECTODERM):
• Sebaceous glands ★
• Hair follicles / hair shafts ★
• Sweat glands
OTHER GERM LAYER ELEMENTS:
MESODERM: Cartilage, bone, smooth muscle, fat
ENDODERM: Bronchial epithelium, GI epithelium, thyroid tissue
• NEURAL TISSUE may be present
• NO mitotic activity, NO atypia in mature teratoma
──────────────────────────────────────────────────────
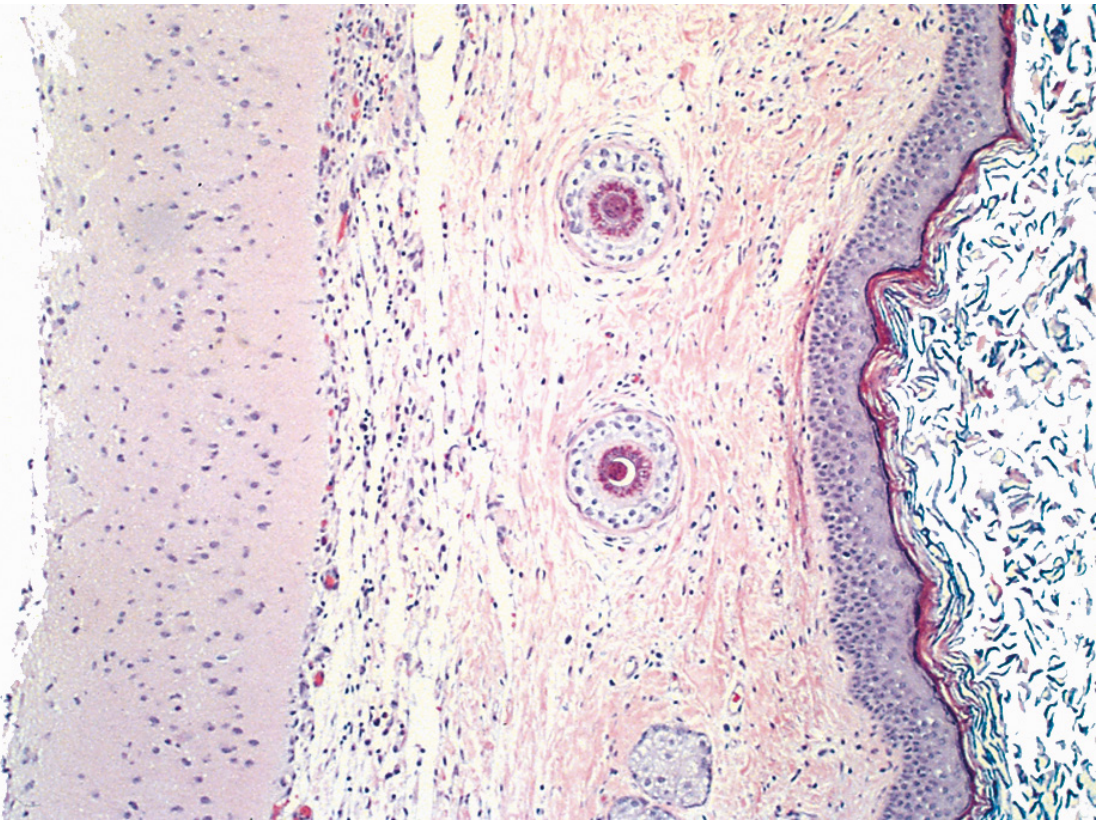
HISTOLOGY IMAGE - Benign Cystic Teratoma:
Fig 22.37: Benign cystic teratoma - cyst wall lined by stratified squamous epithelium with hair follicles (arrowed) and sebaceous glands. Source: Robbins, Cotran & Kumar Pathologic Basis of Disease
Genetics of Mature Teratoma
- Karyotype: 46, XX in almost all cases
- Arise from ovum after first meiotic division (majority)
- Remainder arise before first meiotic division
Malignant Transformation
- Occurs in ~1% of dermoid cysts (mainly in postmenopausal women)
- Most common: Squamous cell carcinoma ★
- Others: Thyroid carcinoma, melanoma
B. IMMATURE (MALIGNANT) TERATOMA
Gross Pathology
GROSS - IMMATURE TERATOMA
───────────────────────────────────────────
• BULKY tumor
• SMOOTH external surface
• SOLID on sectioning ★
• May contain hair, sebaceous material, cartilage
• Areas of NECROSIS and HEMORRHAGE ★
• May have calcification
───────────────────────────────────────────
Microscopic Pathology
HISTOLOGY - IMMATURE TERATOMA
───────────────────────────────────────────────────────
• Tissues resemble EMBRYONAL and IMMATURE FETAL tissue ★
• Key: IMMATURE NEUROEPITHELIUM in varying amounts ★
(resembles developing neural tube/rosettes)
• Immature cartilage, bone, muscle
• Graded I-III based on amount of immature neuroepithelium
• Grade I (<1 low-power field), Grade II (1-3 LPF), Grade III (>3 LPF)
• Mitotic figures present
───────────────────────────────────────────────────────
Prognosis
- Age: Mean 18 years (prepubertal adolescents)
- Stage I, Grade 1: Excellent prognosis
- Higher grade: Chemotherapy required
- Recurrences mainly in first 2 years
C. MONODERMAL (SPECIALIZED) TERATOMA (★ Exam - Functional Tumors)
| Subtype | Key Feature | Complication |
|---|
| Struma Ovarii | Composed entirely of mature thyroid tissue | Hyperthyroidism (if functional) |
| Ovarian Carcinoid | From intestinal tissue in teratoma | Carcinoid syndrome if >7cm (5-HT directly into systemic circulation) ★ |
| Strumal Carcinoid | Combination of struma + carcinoid | Rare |
Exam point: Primary ovarian carcinoid can cause carcinoid syndrome WITHOUT hepatic metastases because ovarian veins connect directly to systemic circulation. ★
EXTRAGONADAL SITES OF TERATOMA (★ Important - Frequently asked)
Teratomas can arise at sites other than gonads. These extragonadal teratomas occur along the midline of the body because primordial germ cells migrate along the midline during development.
EXTRAGONADAL SITES OF TERATOMA
(In order of frequency)
──────────────────────────────────────────────────────────
SITE NOTES
──────────────────────────────────────────────────────────
1. SACROCOCCYGEAL ★★ • Most common extragonadal site
• Most common tumor of newborns
• More common in females (4:1)
• Can be benign or malignant
2. ANTERIOR MEDIASTINUM • 2nd most common
• Young adults
• Can compress mediastinal structures
3. RETROPERITONEUM • 3rd most common extragonadal site
• Often large at diagnosis
4. PINEAL GLAND • Intracranial (most common intracranial GCT)
• Parinaud syndrome (upward gaze palsy)
5. NECK (CERVICAL) • Neonates; may cause airway obstruction
6. ORBIT • Rare
7. LIVER, STOMACH • Very rare
──────────────────────────────────────────────────────────
Mechanism - Why midline?
- During embryogenesis, primordial germ cells migrate from yolk sac along the midline to gonadal ridges
- If germ cells are misplaced along this migratory pathway → form extragonadal teratomas
COMPARISON TABLE - Mature vs Immature Teratoma (MUHS Exam)
| Feature | Mature (Benign) | Immature (Malignant) |
|---|
| Nature | Benign | Malignant |
| Age | Young adults | Adolescents (mean 18 yrs) |
| Common form | Cystic (dermoid cyst) | Solid |
| Bilateral | 10-15% | Rare |
| Contents | Hair, teeth, skin | Neuroepithelium dominant |
| Histology | All mature elements | Immature/fetal elements |
| Mitoses | Absent/rare | Present |
| Malignant change | 1% (SCC most common) | Malignant itself |
| Prognosis | Excellent | Depends on grade/stage |
| Karyotype | 46,XX | Complex |
DYSGERMINOMA vs SEMINOMA (Comparison - MUHS)
| Feature | Dysgerminoma (Ovary) | Seminoma (Testis) |
|---|
| Origin | Ovarian germ cell | Testicular germ cell |
| Age | 2nd-3rd decade | 3rd-4th decade |
| Gross | Solid, fleshy, gray-pink | Solid, lobulated, creamy white |
| Histology | Large clear cells + lymphocytes | Same |
| Bilateral | 10-15% | Rare |
| Markers | OCT3/4, NANOG, KIT, i(12p) | Same |
| Malignancy | All malignant; 1/3 aggressive | All malignant |
| Chemo/Radio | Highly sensitive ★ | Highly sensitive ★ |
TUMOR MARKERS SUMMARY (MUHS Short-Answer Tip)
| GCT | Marker |
|---|
| Dysgerminoma | OCT3/4, NANOG; elevated hCG (if syncytiotrophoblastic cells present) |
| Yolk Sac Tumor | AFP (α-fetoprotein) ★★ |
| Choriocarcinoma | β-hCG ★★ |
| Mature Teratoma | None specific |
| Immature Teratoma | AFP (if yolk sac elements) |
KEY EXAM POINTS - QUICK RECAP
Fibroid Uterus:
- Most common = menorrhagia (★)
- Whorled cut surface (★)
- Estrogen dependent, shrinks after menopause (★)
- Degenerations: Hyaline (most common), Red (in pregnancy) (★)
- Malignant change = extremely rare
Dysgerminoma:
- = Ovarian counterpart of testicular seminoma (★)
- Solid, fleshy, gray-pink tumor
- Large clear cells + lymphocytic stroma (★)
- OCT3/4, NANOG, KIT, i(12p) (★)
- Highly chemo/radiosensitive (★)
Teratoma:
- Mature cystic = dermoid cyst = most common ovarian GCT (★)
- Contains hair, teeth, skin adnexa
- 1% malignant change → SCC most common (★)
- Immature = graded by immature neuroepithelium (★)
- Struma ovarii → hyperthyroidism; Carcinoid → carcinoid syndrome (★)
- Extragonadal: Sacrococcygeal (most common) > Mediastinum > Retroperitoneum (★)
Sources: Robbins & Kumar Basic Pathology (10th ed.), Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), Berek & Novak's Gynecology