Advances in volume scanning in detail
volume scanning CT ultrasound advances
advances in volume scanning CT ultrasound 4D radiology 2024 2025
https://www.dirjournal.org/articles/doi/dir.2024.242926
"volume CT" OR "volumetric scanning" advances imaging
PMID: 40300917
Advances in Volume Scanning
1. Evolution from Single-Slice to Multidetector CT (MDCT)
- Shorter scan times, reducing motion artifact
- Sub-millimeter isotropic voxels enabling high-quality multiplanar reformats (axial, coronal, sagittal) and 3D volume rendering
- CT angiography (CTA) and CT perfusion by dynamic contrast acquisition
- Sections as thin as 0.5–1 mm with 0.4 mm in-plane resolution at 0.3 seconds per rotation; complete brain studies in 1–10 seconds
2. Wide-Area / 320-Detector Row CT: True Single-Rotation Volume Coverage
Clinical Applications
3. Four-Dimensional CT (4D-CT): Adding Time as a Dimension
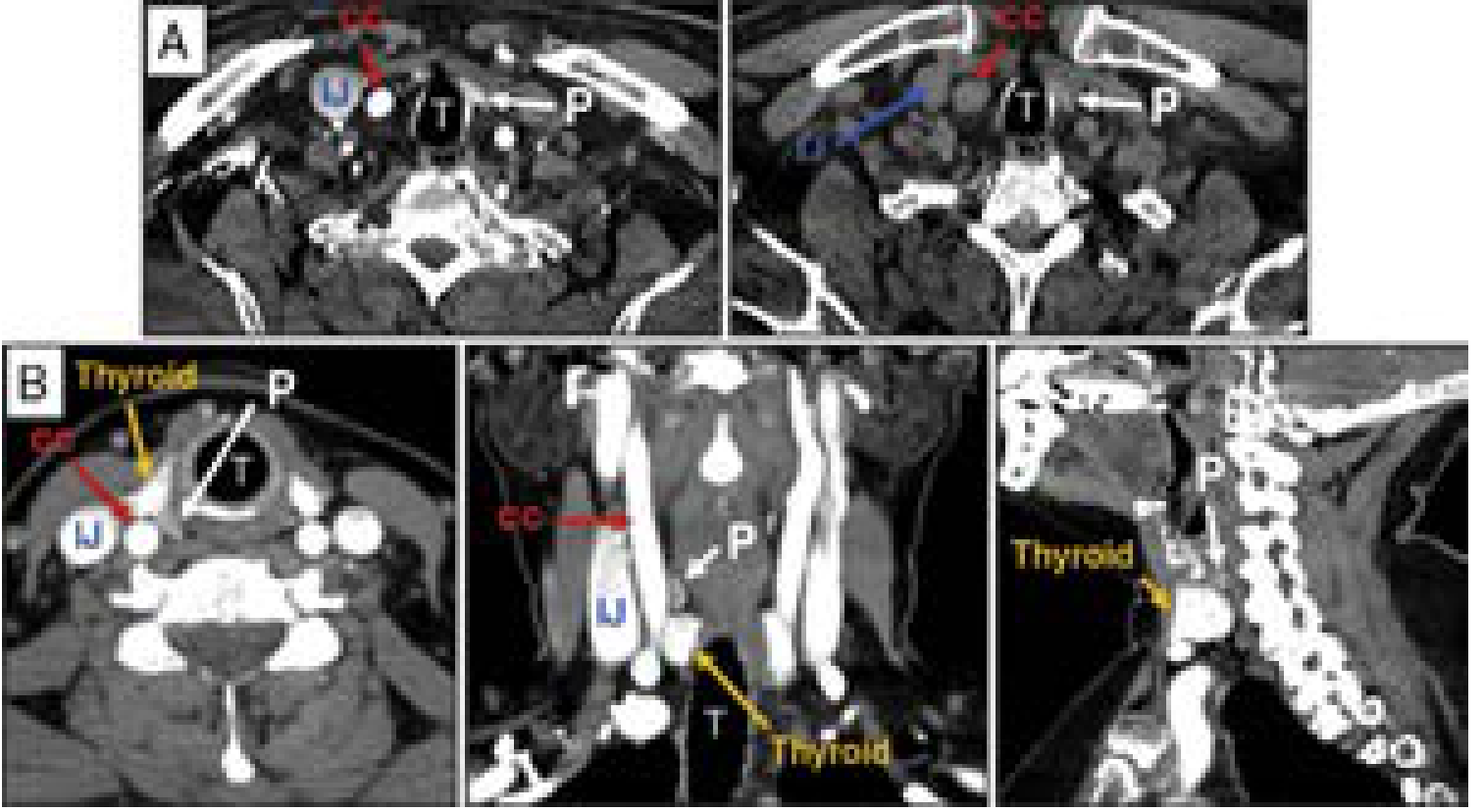
Parathyroid Localization
- Non-contrast
- Arterial
- Venous
- Delayed/washout
Musculoskeletal / Orthopaedic Applications
- Costoclavicular impingement
- Scapholunate instability
- Capitate subluxation
- Pisotriquetral instability
- Acromioclavicular dislocation
- Snapping scapula
Weight-Bearing CT (WBCT)
- Pre/postoperative evaluation of total ankle replacements
- Patellofemoral instability after MPFL reconstruction
- Diabetic foot architecture
- Flatfoot reconstruction
- Syndesmotic instability (a systematic review found WBCT measuring the syndesmotic area to be the most reliable parameter for this diagnosis) — Rockwood & Green's Fractures in Adults 10th ed 2025
4. Photon-Counting CT (PCD-CT): The Latest Detector Revolution
| Feature | Conventional MDCT | Photon-Counting CT |
|---|---|---|
| Resolution | ~0.4–0.5 mm in-plane | ~0.2 mm |
| Electronic noise | Inherent scintillator noise | Greatly reduced |
| Radiation dose | Standard | Often reduced |
| Spectral capability | Limited (dual-energy variants) | Multi-energy bins in each acquisition |
| Contrast dose | Standard iodine volume | Reduced contrast required |
| Metal/bone artifact | Beam hardening present | Improved calcium/bone artifact reduction |
5. 3D and 4D Ultrasound Volume Scanning
Mechanical Scanning
Free-Hand Scanning
2D Phased-Array Transducers (Matrix Arrays) — Real-Time 4D
- Wideband 2D sparse arrays with multiline receiving optimize active component count while maintaining accuracy and speed
- Obstetrics: Real-time 4D visualization of fetal face, movement, anomalies (midline cleft lip, anencephaly, Müllerian anomalies)
- Cardiology: Real-time 3D echocardiography for valve morphology, ventricular volumes, wall motion
- Oncology: Tumor margin delineation and volume measurements
- Urology: 3D TRUS for prostate volume calculation; cryo-probe placement confirmation
6. Dual-Energy CT and Spectral Imaging
- Material decomposition (iodine vs. calcium vs. uric acid maps)
- Virtual non-contrast reconstructions
- Reduced metal artifact via monoenergetic reconstructions
- Improved lesion characterization (e.g., renal stone composition, gout)
7. 3D Reconstruction and Post-Processing
- Multiplanar reformation (MPR): Axial, coronal, sagittal, oblique
- Maximum-intensity projection (MIP): Vascular and high-density structures
- 3D volume rendering: Surgical planning (fracture, tumor, vascular anatomy)
- "Ghosting" / bone removal for orthopaedic fracture visualization
- 3D printing: CT data used to generate physical models for maxillofacial reconstruction, complex fracture management, deformity correction, and tumor resection planning
- AI-assisted segmentation: Automated organ/lesion volumetry, plaque quantification (FFR-CT), myocardial mass estimation
Summary Table
| Technology | Key Advance | Clinical Gain |
|---|---|---|
| Helical CT | Continuous volumetric acquisition | Replaces sequential slices; CTA enabled |
| MDCT (64–256 row) | Faster, thinner, isotropic voxels | Sub-mm resolution; multiplanar reformat |
| 320-row wide-area CT | Single-rotation organ coverage | 4D cardiac, 4D-CTA, reduced dose |
| 4D-CT | Temporal dimension added | Parathyroid localization; joint kinematics |
| Weight-bearing CBCT | Physiologic loading during scan | Syndesmotic, ankle, flatfoot assessment |
| Photon-counting CT | Direct x-ray→electric conversion | 0.2 mm resolution; reduced dose/contrast |
| Dual-energy/Spectral CT | Multi-energy acquisition | Material decomposition; reduced artifact |
| 4D ultrasound (matrix array) | Real-time volumetric US | Fetal, cardiac, oncology applications |
| AI integration | Automated segmentation & analysis | FFR-CT, volumetry, prognostic biomarkers |
- Harrison's Principles of Internal Medicine 22E, p. 3427 (MDCT, photon-counting CT)
- Grainger & Allison's Diagnostic Radiology (MDCT evolution, 320-row cardiac CT)
- Bradley and Daroff's Neurology in Clinical Practice (4D-CTA, 320-row neurovascular)
- Current Surgical Therapy 14e (4D-CT parathyroid localization)
- Rockwood & Green's Fractures in Adults 10th ed 2025 (4D-CT joints, WBCT, 3D printing)
- Rubio PM et al. J Cardiovasc Comput Tomogr 2025 — Key advances in cardiac CT (PMID: 40300917)
- DIR Journal 2024 — New imaging techniques and trends in radiology
Advances in volume scanning in ct in detail , firstly define volume scanning and it principle , components and u want to add , and then advances
"computed tomography" volumetric scanning advances review
volume CT scanning definition principle components advances 2024 2025 radiology review
https://aditum.org/images/article/1769068116Advances_in_CT_I…
- MDCT evolution (single-slice → 320 row)
- Wide-area detectors & 320-row CT (single-rotation organ coverage)
- Four-dimensional CT — parathyroid & joint biomechanics
- Iterative reconstruction (30–80% dose reduction)
- Photon-counting CT — 0.2 mm resolution, direct x-ray conversion, multi-energy spectral bins
- Dual-Energy / Dual-Source CT — material decomposition and spectral imaging
- Deep Learning Reconstruction + AI (FFR-CT, automated segmentation, biomarkers)
- High-Resolution thin-section protocols from volumetric data
- Cone-beam CT and weight-bearing CT
- Portable/point-of-care volume CT
Interventional guidance tools in CT what to write ?
interventional guidance tools CT-guided procedures biopsy ablation drainage navigation 2024 2025 review
"CT-guided" interventional procedures needle guidance tools
CT-guided percutaneous interventional radiology biopsy ablation
CT guided interventional tools needle guidance systems robotic navigation augmented reality 2024 2025
- Definition — what CT interventional guidance is and why CT is chosen over US/fluoroscopy
- CT vs US vs Fluoroscopy comparison table
- Standard workflow — pre-planning, positioning, localization
- Core guidance modes (the main exam topic):
- Conventional / quick-check CT
- CT Fluoroscopy (real-time) — mechanism, advantages, radiation danger
- Gantry tilt
- Combined CT + Fluoroscopy
- Cone-Beam CT with fluoroscopic overlay
- Interventional procedures performed under CT guidance:
- Biopsy (FNA, core, coaxial technique, complications)
- Drainage (abscess, pleural, nephrostomy)
- Ablation — full detail on RFA, Microwave, Cryoablation, IRE, Laser, HIFU — mechanisms, advantages, CT monitoring role
- Bone/spine interventions
- Advanced guidance tools (emerging/advances section):
- Electromagnetic navigation
- Optical tracking + Robotics
- Augmented Reality (AR/XR)
- CT-US Fusion
- AI needle companion software
- Hybrid CT-angiography suites
- Decision framework — when to use which modality
- Summary table + 12 Key Exam Points