Seizure internal medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"seizure" AND "management" AND "internal medicine"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full response covering all aspects of seizure in internal medicine.
Seizures - Internal Medicine
Definition & Key Distinctions
A seizure is a transient occurrence of signs or symptoms due to abnormal, excessive, or synchronous neuronal activity in the brain. About 5-10% of the population will have at least one seizure in their lifetime.
Seizure vs. Epilepsy:
- A provoked (acute symptomatic) seizure occurs in close temporal relationship with a reversible/acquired precipitating condition (e.g., metabolic derangement, drug toxicity).
- An unprovoked seizure occurs in the absence of a temporary or reversible cause.
- Epilepsy is diagnosed when a patient has: (a) 2+ unprovoked seizures occurring >24 hours apart, OR (b) 1 unprovoked seizure with ≥60% probability of recurrence over the next 10 years, OR (c) a diagnosed epilepsy syndrome.
After a single unprovoked seizure: ~40-50% risk of a second seizure over 2-8 years. After two unprovoked seizures: ~60-90% risk of a third.
(Harrison's Principles of Internal Medicine 22E, Frameworks for Internal Medicine)
ILAE 2017 Classification of Seizure Types
| Category | Subtypes |
|---|---|
| Focal Onset | - With intact awareness - With impaired awareness - Motor vs. nonmotor onset - Focal to bilateral tonic-clonic |
| Generalized Onset | - Motor: tonic-clonic, tonic, clonic, myoclonic, atonic, epileptic spasms - Nonmotor (absence): typical, atypical, myoclonic |
| Unknown Onset | Motor, nonmotor, or unclassified |
Why classification matters: Some antiseizure drugs treat focal seizures but are ineffective (or harmful) in generalized epilepsy (e.g., carbamazepine can worsen absence or myoclonic seizures). Surgical options also exist for certain focal but not generalized seizure disorders.
(Harrison's 22E, Table 436-1; Frameworks for Internal Medicine)
Focal Seizures - Key Features
Focal seizures with intact awareness (formerly simple partial): motor, sensory, autonomic, or psychic symptoms without loss of consciousness. A Jacksonian march (clonic spread through contiguous body parts on the same side) reflects horizontal spread across the motor strip.
Focal seizures with impaired awareness (formerly complex partial): most commonly arise from temporal or frontal lobe. Features include:
- Behavioral arrest/stare
- Complex automatisms (lip-smacking, picking at clothes, repetitive hand movements)
- Postictal confusion, dysphasia (if dominant hemisphere), memory loss
- Duration: seconds to minutes
Mesial Temporal Lobe Epilepsy (MTLE) is the most common focal epilepsy syndrome, associated with hippocampal sclerosis on MRI (small hippocampus with increased T2 signal and loss of internal laminar architecture).
Focal to bilateral tonic-clonic seizure: previously called "secondarily generalized" - a focal seizure that spreads to both hemispheres.
(Harrison's 22E, Bradley and Daroff's Neurology)
Generalized Seizures - Key Features
| Type | Features |
|---|---|
| Tonic-clonic (grand mal) | Sudden loss of consciousness, tonic phase (limb stiffening, cry, cyanosis) then clonic phase (rhythmic jerking); postictal confusion/drowsiness |
| Absence (petit mal) | Brief (5-30 sec) behavioral arrest/stare, no postictal confusion; 3-Hz spike-and-wave on EEG; often in children |
| Myoclonic | Brief, shock-like muscle jerks; may be bilateral; characteristic of juvenile myoclonic epilepsy |
| Tonic | Sustained muscle stiffening without clonic phase |
| Atonic (drop attack) | Sudden loss of muscle tone causing falls; risk of injury |
| Clonic | Rhythmic jerking only, without initial tonic phase |
Causes of Seizures by Age Group
| Age Group | Common Causes |
|---|---|
| Neonates | Perinatal hypoxia/ischemia, intracranial hemorrhage, CNS infection, metabolic (hypoglycemia, hypocalcemia, hypomagnesemia, pyridoxine deficiency), genetic |
| Infants/Children | Febrile seizures, genetic disorders, developmental disorders, CNS infection, trauma |
| Adolescents/Young Adults | Idiopathic (genetic) epilepsy, trauma, drug/alcohol use |
| Adults | Tumor, trauma, alcohol withdrawal, CNS infection, stroke, metabolic disorders |
| Elderly (>65) | Cerebrovascular disease (most common), tumor, metabolic disorders, Alzheimer's/neurodegenerative disease |
Common metabolic/toxic causes (provoked seizures):
- Hyponatremia, hypoglycemia, hypocalcemia, hypomagnesemia
- Uremia, hepatic encephalopathy
- Drug toxicity: bupropion, cocaine, isoniazid, theophylline, tramadol, fluoroquinolones
- Drug/alcohol withdrawal (especially benzodiazepine and alcohol withdrawal)
- CNS infections: meningitis, encephalitis, abscess, neurocysticercosis
(Harrison's 22E, Table 436-4)
Differential Diagnosis
Conditions that mimic seizures must be excluded:
- Syncope (vasovagal, cardiac) - brief LOC, posture-related, rapid recovery; can have brief myoclonic jerks
- Transient ischemic attack (TIA) - typically negative symptoms (weakness, sensory loss), not positive (jerking); no postictal phase
- Migraine with aura - sensory or visual spread is slower (minutes), not Jacksonian march (seconds)
- Psychogenic non-epileptic seizures (PNES) - often prolonged, pelvic thrusting, eyes closed during event, no postictal confusion, normal EEG during event
- Hypoglycemia - may cause focal deficits or LOC; check glucose first
- Acute psychosis
- Transient global amnesia
(Harrison's 22E; Frameworks for Internal Medicine)
Evaluation of the Adult Patient with a Seizure
The diagnostic flowchart from Harrison's 22E guides management:
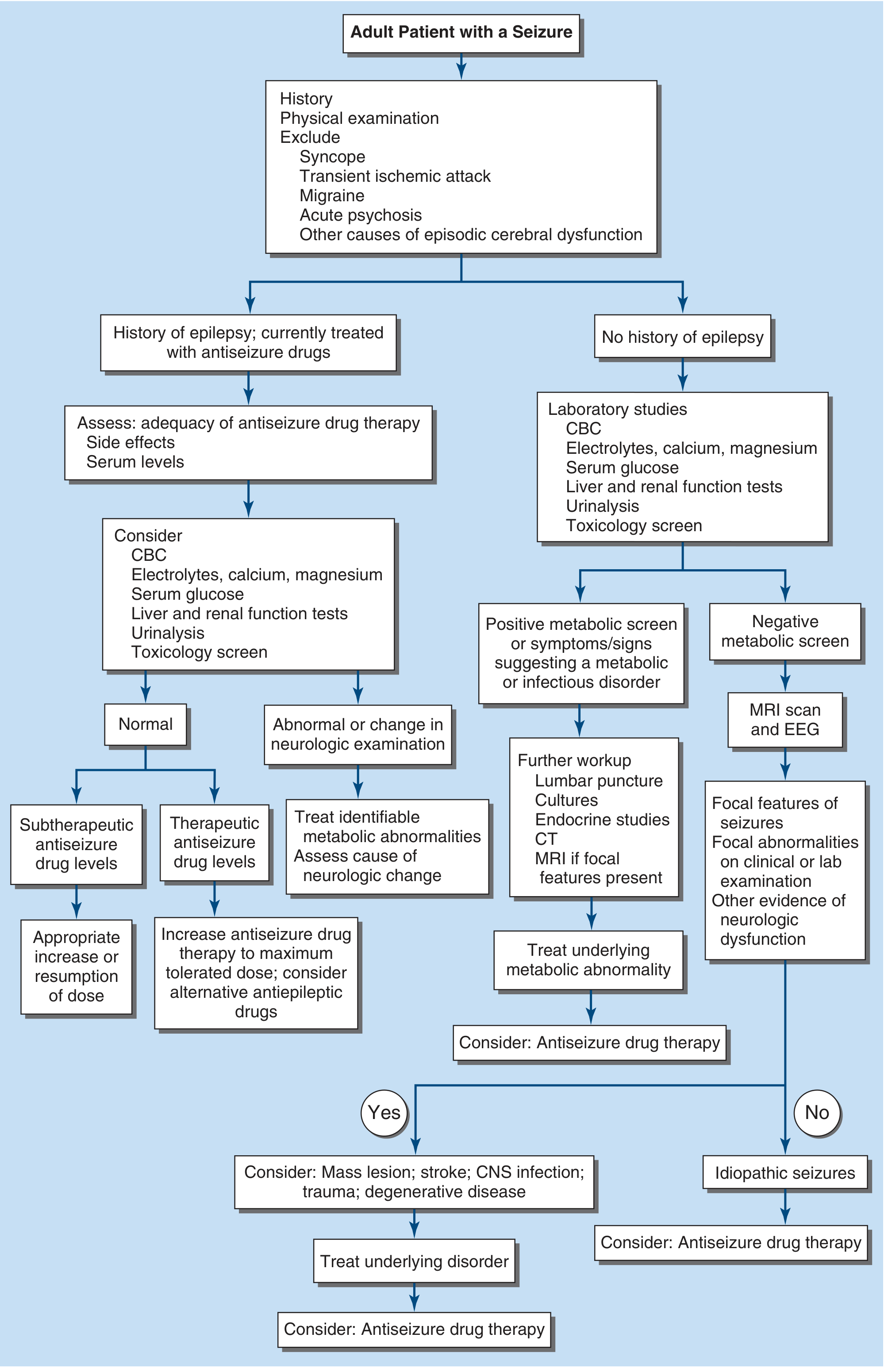
History priorities:
- Was this truly a seizure? (pre/ictal/postictal details; eyewitness account)
- First seizure or known epilepsy?
- Identify risk factors: prior head trauma, stroke, CNS infection, tumor, family history, febrile seizures
- Precipitating factors: sleep deprivation, medications, alcohol/drug use, fever, metabolic issues
Physical exam: Vital signs, signs of CNS infection (fever, meningismus), skin (neurocutaneous disorders), organomegaly, head trauma, complete neurological exam (focal deficits, postictal Todd's paralysis)
Lab workup (all first seizures):
- CBC, electrolytes, calcium, magnesium, glucose
- Liver and renal function tests
- Urinalysis, toxicology screen
- Consider: LP (if meningitis/encephalitis suspected; mandatory in HIV patients)
- Autoantibody panel (serum + CSF) if fulminant onset with psychiatric/cognitive features (e.g., anti-NMDA receptor encephalitis)
EEG:
- All patients with possible seizure should have an EEG as soon as possible
- Normal interictal EEG does not exclude epilepsy
- Epileptiform spikes/sharp waves are abnormal interictal discharges
- 3-Hz spike-and-wave is characteristic of absence epilepsy
- Activating procedures: hyperventilation (provokes absence), photic stimulation, sleep deprivation
Neuroimaging:
- MRI is the preferred modality (superior to CT for most epileptic etiologies)
- CT is acceptable in emergencies (rule out hemorrhage, large mass)
- Indications for urgent neuroimaging: first seizure with abnormal neurological exam, focal features, no clear metabolic cause, HIV-positive patient
(Harrison's 22E)
Antiseizure Drug (ASD) Therapy
When to Start
- Recurrent unprovoked seizures: always treat
- Single seizure: treat if high-risk features are present:
- Prior brain lesion (stroke, trauma, tumor)
- EEG with epileptiform abnormalities
- Significant brain imaging abnormality
- Nocturnal seizure
- Provoked (metabolic) seizures: correct the underlying cause; ASD usually not needed long-term
Drug Choice by Seizure Type
| Seizure/Syndrome | First-Line Agents |
|---|---|
| Focal onset ± secondary generalization | Carbamazepine, oxcarbazepine, lamotrigine, levetiracetam, lacosamide |
| Generalized tonic-clonic | Valproate, lamotrigine, levetiracetam, topiramate |
| Absence | Ethosuximide (drug of choice), valproate, lamotrigine |
| Juvenile myoclonic epilepsy (JME) | Valproate, levetiracetam, lamotrigine (avoid carbamazepine - worsens myoclonus) |
| Atonic/tonic seizures (Lennox-Gastaut) | Valproate, lamotrigine, rufinamide, clobazam |
Mechanisms of Action (Katzung)
- Sodium channel blockade (carbamazepine, phenytoin, lamotrigine, lacosamide): reduces high-frequency neuronal firing
- GABA enhancement (benzodiazepines, phenobarbital, vigabatrin, tiagabine): enhances inhibitory tone
- Calcium channel modulation (ethosuximide, valproate): reduces T-type Ca²⁺ currents (important for absence)
- Synaptic vesicle protein (SV2A) binding (levetiracetam): unique mechanism, modulates synaptic release
- HCN channel/multiple mechanisms (valproate, topiramate, zonisamide)
Key Drug Notes
| Drug | Key Points |
|---|---|
| Phenytoin | Oldest nonsedating ASD (since 1938); zero-order kinetics - small dose increases cause disproportionate level rises; enzyme inducer; risk of gingival hyperplasia, hirsutism, cerebellar atrophy |
| Carbamazepine | First-line for focal seizures; enzyme autoinducer (half-life decreases from 36h to 8-12h with continued use); therapeutic level 4-8 mcg/mL; can worsen absence/myoclonic seizures |
| Valproate | Broad-spectrum; teratogenic (neural tube defects) - avoid in women of childbearing age if possible; hepatotoxicity risk; weight gain, tremor |
| Lamotrigine | Broad-spectrum; Stevens-Johnson syndrome risk (slow titration required); safe in pregnancy (relatively) |
| Levetiracetam | Broad-spectrum; minimal drug interactions; mood/behavioral side effects (irritability) |
| Ethosuximide | Only for absence seizures; T-type Ca²⁺ channel blocker |
| Topiramate | Broad-spectrum; cognitive slowing ("dopamax"), kidney stones, weight loss |
Monotherapy is effective in <50% of patients with epilepsy; combination is commonly required. Overall, ~60-70% of patients achieve long-term remission with medication.
(Katzung Basic & Clinical Pharmacology 16e; Harrison's 22E)
Status Epilepticus
Definition: Seizure lasting ≥5 minutes, OR recurrent seizures without return to baseline between episodes.
This is a medical emergency with ~20% mortality in convulsive SE.
Management Timeline
| Time | Action |
|---|---|
| 0-5 min | ABCs, IV access, oxygen, monitor; finger-stick glucose; thiamine 100 mg IV (before glucose) if alcoholism/malnutrition suspected |
| 5-20 min (Benzodiazepine phase) | Lorazepam 0.1 mg/kg IV (first-line) OR diazepam IV/PR OR midazolam IM (if no IV access) |
| 20-40 min (2nd agent) | Fosphenytoin 20 PE/kg IV (preferred over phenytoin - less cardiac toxicity) OR valproate IV OR levetiracetam IV OR lacosamide IV OR phenobarbital IV |
| >40 min (Refractory SE) | Intubation + propofol, midazolam, or pentobarbital infusion with continuous EEG monitoring |
Always look for the underlying cause: hypoglycemia, hyponatremia, CNS infection, drug toxicity, stroke, non-compliance with ASD, alcohol withdrawal.
Specific Situations
Febrile Seizures
- Most common seizure type in children (6 months - 5 years)
- Simple febrile seizure: single, brief (<15 min), symmetric - no ASD required; antipyretics for comfort
- Complex febrile seizure: >15 minutes, focal features, or recurrence within 24h - investigate and consider short-term treatment
Pregnancy
- Seizure risk changes with pregnancy (hormonal, volume distribution changes)
- Preferred agents: lamotrigine, levetiracetam (lower teratogenicity); valproate should be avoided (highest neural tube defect risk among ASDs)
- All women of childbearing age on ASDs should take folic acid 5 mg/day
Alcohol Withdrawal Seizures
- Typically occur 6-48 hours after the last drink
- Generalized tonic-clonic
- Treat with benzodiazepines (lorazepam or diazepam)
- Phenytoin is NOT effective for alcohol withdrawal seizures
First Unprovoked Seizure - To Treat or Not?
- Consider treating if EEG abnormal, MRI abnormal, nocturnal onset, prior brain injury
- Recurrence risk ~40-50% in 2 years without treatment; treatment reduces risk by ~50%
Non-Pharmacologic Treatment
- Epilepsy surgery: resection of seizure focus; most effective for drug-resistant mesial temporal lobe epilepsy. Anterior temporal lobectomy yields ~60-70% seizure freedom.
- Vagus nerve stimulation (VNS): palliative; reduces seizure frequency ~50% in ~50% of patients
- Ketogenic diet: high-fat, low-carbohydrate; particularly effective in children; useful in GLUT-1 deficiency
- Responsive neurostimulation (RNS): closed-loop brain stimulation for drug-resistant focal epilepsy
- Lifestyle: avoid sleep deprivation, excessive alcohol, known triggers; stress reduction
Postictal State
After a generalized tonic-clonic seizure, patients typically have:
- Confusion, drowsiness, headache (minutes to hours)
- Todd's paralysis: focal weakness/paralysis lasting minutes to hours; localizes to the contralateral hemisphere of the seizure focus
- Elevated serum prolactin (within 20 minutes of a generalized seizure) can help differentiate from PNES (though not diagnostic)
- Muscle soreness, tongue biting, urinary incontinence
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 436
- Frameworks for Internal Medicine, Chapter 42
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 100
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Chapter 24
This is a shared conversation. Sign in to Orris to start your own chat.