gram negative cocci full detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
Neisseria gram negative cocci diplococci microscopy
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full, detailed answer.
Gram-Negative Cocci — Full Detail
Gram-negative cocci are a small but clinically critical group of bacteria. The two medically important genera are Neisseria and Moraxella, with anaerobic gram-negative cocci (Veillonella) as a minor addition. Below is a structured, textbook-level review.
1. Classification Overview
| Organism | Genus | Key Disease |
|---|---|---|
| N. gonorrhoeae | Neisseria | Gonorrhea, disseminated gonococcal infection |
| N. meningitidis | Neisseria | Meningitis, meningococcemia |
| Commensal Neisseria spp. | Neisseria | Opportunistic infections |
| Moraxella catarrhalis | Moraxella | COPD exacerbation, otitis media, sinusitis |
| Veillonella spp. | Veillonella | Rare anaerobic infections |
2. General Characteristics of Neisseria
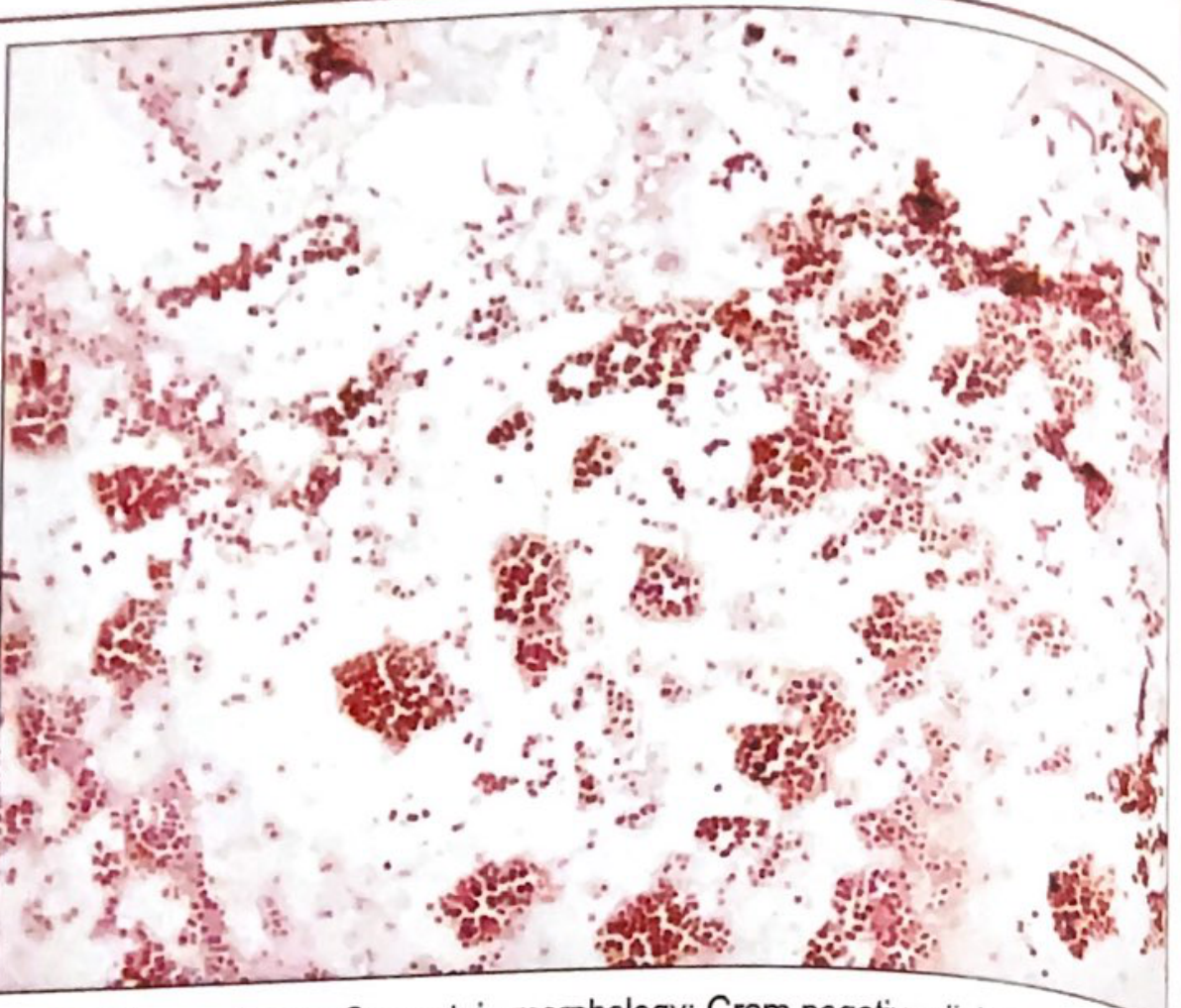
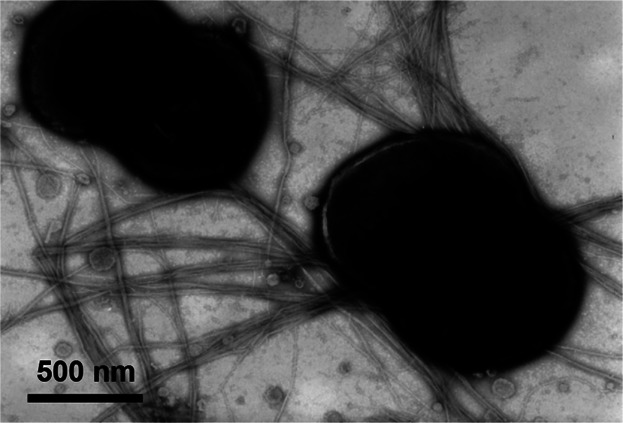
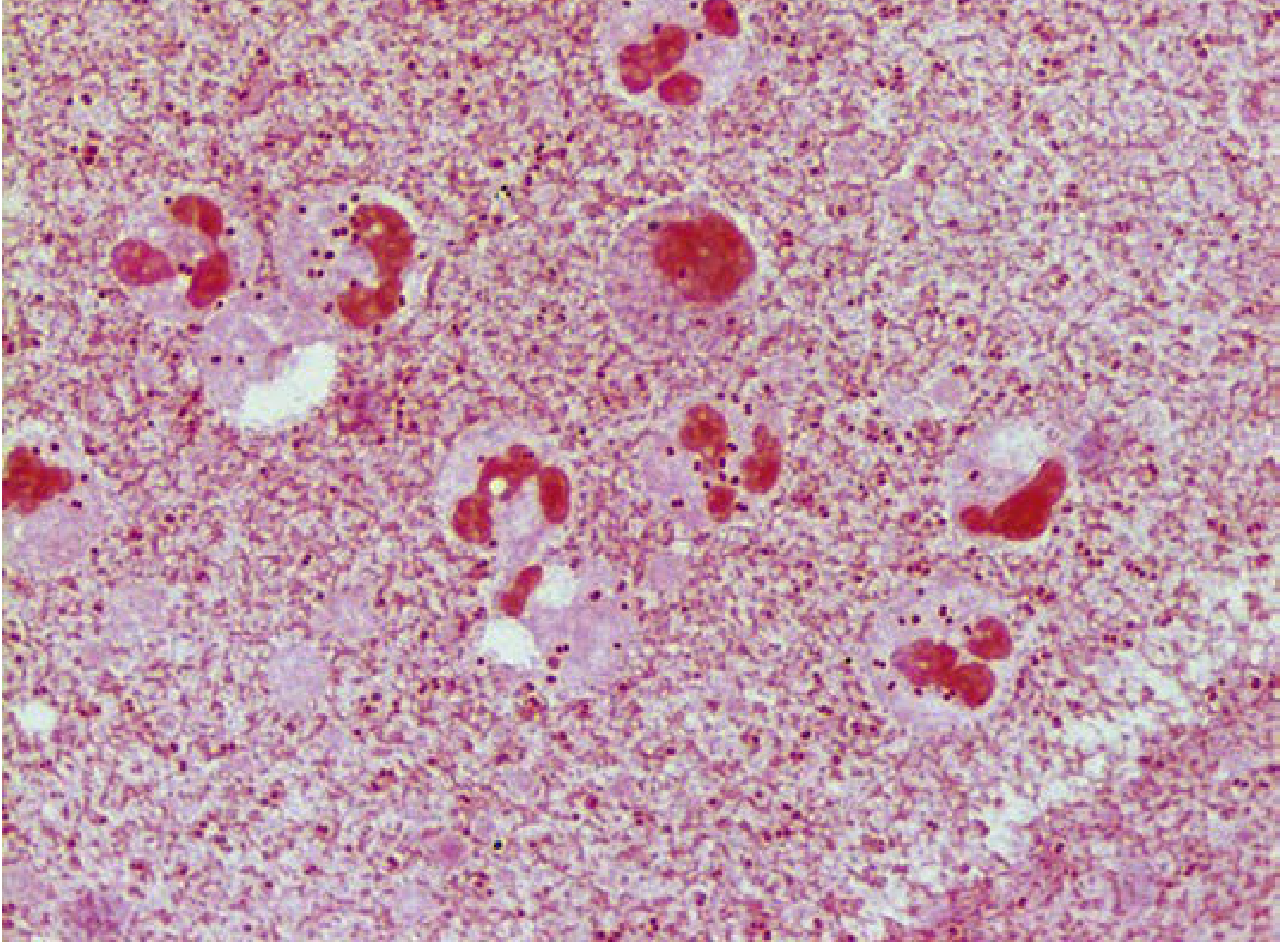
- Morphology: Aerobic gram-negative cocci, 0.6–1.0 µm in diameter, arranged in pairs (diplococci) with flattened adjacent surfaces — resembling coffee beans or kidney beans
- Oxidase positive, catalase positive
- Nonmotile
- Fastidious: Require prompt incubation at 35–37°C in CO₂; need blood, serum, or special media for growth
- Both N. gonorrhoeae and N. meningitidis produce an IgA protease that cleaves mucosal IgA, facilitating colonization
- Carbohydrate utilization (key differential):
| Organism | Glucose | Maltose | Lactose | DNase |
|---|---|---|---|---|
| N. gonorrhoeae | + | − | − | − |
| N. meningitidis | + | + | − | − |
| M. catarrhalis | − | − | − | + |
- 35 species in genus; only N. gonorrhoeae and N. meningitidis are strict human pathogens; others are commensal upper respiratory tract flora
3. Neisseria gonorrhoeae
3.1 Physiology and Virulence Factors
| Virulence Factor | Role |
|---|---|
| Pili (fimbriae) | Mediate attachment to non-ciliated epithelial cells; inhibit phagocytosis; antigenically variable (no protective immunity) |
| Por proteins (Porin) | Outer membrane porins; facilitate intracellular survival by preventing phagosome–lysosome fusion |
| Opa proteins | Adhesins facilitating tight cell attachment and invasion |
| Rmp protein | Blocks bactericidal antibodies |
| Lipooligosaccharide (LOS) | Endotoxin activity; causes cytokine release and tissue damage |
| IgA protease | Cleaves secretory IgA on mucosal surfaces |
| β-lactamase | Resistance mechanism |
| Transferrin/lactoferrin receptors | Iron acquisition from host |
3.2 Epidemiology
- Humans are the only natural host
- Transmission: sexual contact (primary)
- ~555,608 cases in the US in 2017 (true incidence estimated twice this); ~78 million new cases worldwide annually
- Most common in: ages 15–24, Black Americans, southeastern US, individuals with multiple sexual partners
- Higher risk of disseminated disease in patients with late complement component deficiencies (C5–C9)
- Carriage is often asymptomatic in females (50%) and symptomatic in most males (90%)
3.3 Clinical Diseases
In Men:
- Urethritis: purulent urethral discharge, dysuria — onset 2–5 days post-exposure
- Complications: epididymitis, prostatitis, periurethral abscess; recurrent infections → scarring → sterility
In Women:
- Primary site: endocervix (columnar epithelial cells; NOT squamous cells of vagina)
- Endocervicitis: purulent vaginal discharge, dysuria, abdominal pain
- Pelvic Inflammatory Disease (PID) in 10–20%: salpingitis, tubo-ovarian abscess → ectopic pregnancy, infertility
Other Sites:
- Pharyngitis (purulent exudate, often asymptomatic)
- Proctitis (rectal infections in men who have sex with men)
- Ophthalmia neonatorum: purulent conjunctivitis in neonates born through infected birth canal → can rapidly lead to blindness if untreated
Disseminated Gonococcal Infection (DGI) (1–3% of infected women, rare in men):
- Migratory arthralgia → septic arthritis (wrists, knees, ankles)
- Pustular rash on erythematous base over extremities (dermatitis-arthritis syndrome)
- Gram stain of synovial fluid positive in only 10–30% of cases (culture often negative)
3.4 Laboratory Diagnosis
| Method | Notes |
|---|---|
| Gram stain | Sensitive for symptomatic males (urethral discharge); GNID in PMNs — but NOT reliable in cervical specimens |
| Culture on Thayer-Martin or Martin-Lewis agar | Modified chocolate agar + vancomycin + colistin + nystatin — inhibits normal flora; sensitive & specific |
| NAAT (Nucleic Acid Amplification Tests) | Gold standard now — most sensitive, used for urine, swabs; replaced culture in most labs |
| Oxidase test | Positive |
3.5 Treatment, Prevention, and Control
- Treatment of choice: Ceftriaxone 500 mg IM single dose (with doxycycline if chlamydia co-infection not excluded)
- High-level resistance to cephalosporins and azithromycin is emerging
- Previous dual therapy with ceftriaxone + azithromycin is now modified to ceftriaxone alone (due to azithromycin resistance)
- Ophthalmia neonatorum prophylaxis: 1% silver nitrate OR erythromycin ointment (0.5%) applied to newborn eyes
- No effective vaccine available
- Prevention: condoms, spermicides with nonoxynol-9 (partially effective), partner notification
4. Neisseria meningitidis
4.1 Physiology and Virulence Factors
| Virulence Factor | Role |
|---|---|
| Polysaccharide capsule | Principal virulence factor — inhibits phagocytosis; basis of serogroup classification |
| Pili (Type IV) | Adherence to nasopharyngeal epithelium; twitching motility; DNA uptake |
| LOS (Lipooligosaccharide) | Endotoxin — activates clotting cascade → hemorrhage in adrenals and other organs; alters peripheral vascular resistance → shock and death |
| IgA protease | Cleaves mucosal IgA |
| Outer membrane proteins | Immune evasion |
4.2 Serogroups (based on capsule polysaccharide)
- A, B, C, W-135, X, Y — Six major pathogenic serogroups
- In the US: most common are B, C, Y, W-135
- Serogroup A: responsible for "meningitis belt" epidemics in sub-Saharan Africa
- Serogroup B: particularly difficult to vaccinate against (capsule mimics human neural cell adhesion molecules)
4.3 Epidemiology
- 5–15% of healthy adults are asymptomatic nasopharyngeal carriers
- Colonization followed 7–10 days later by formation of bactericidal antibodies (provides serogroup-specific immunity)
- Disease mostly in children < 5 years and adolescents/young adults (college freshmen)
- Transmission: respiratory droplets and direct contact with oral secretions
- Risk factors: complement deficiencies (C5–C9), asplenia, crowding (military barracks, dormitories), IgG subclass deficiency
4.4 Clinical Diseases
Meningitis:
- Purulent inflammation of meninges
- Classic triad: fever, severe headache, nuchal rigidity
- Photophobia, phonophobia, altered consciousness
- High mortality if untreated; 10–15% mortality even with treatment; 20% morbidity with neurological sequelae
Meningococcemia:
- Disseminated bloodstream infection
- Petechial/purpuric rash — small petechiae coalesce into larger hemorrhagic lesions (pathognomonic)
- Thrombosis of small blood vessels → Waterhouse-Friderichsen syndrome: bilateral adrenal hemorrhage → adrenal insufficiency → shock
- DIC (Disseminated Intravascular Coagulation)
- Multiorgan failure; rapidly fatal without treatment
Other:
- Meningococcal pneumonia (milder, in patients with underlying pulmonary disease)
- Pleuritis, pericarditis, arthritis (serous membrane involvement)
- Mild pharyngitis (early/asymptomatic colonization)
4.5 Laboratory Diagnosis
| Method | Notes |
|---|---|
| CSF Gram stain | Gram-negative diplococci in PMNs (intracellular) |
| Culture | Blood and CSF; chocolate agar or blood agar |
| Latex agglutination | Rapid CSF antigen detection (serogroups A, B, C, W-135, Y) |
| PCR | Increasingly used, especially when antibiotics given before culture |
4.6 Treatment, Prevention, and Control
- Treatment: IV Penicillin G (if sensitive), Ceftriaxone (drug of choice), or cefotaxime
- Chemoprophylaxis for close contacts: Rifampin (drug of choice), ciprofloxacin (single dose), or ceftriaxone IM
- Close contacts = household members, those with contact with oral secretions
Vaccines:
| Vaccine | Coverage | Indication |
|---|---|---|
| MenACWY (conjugate) | Serogroups A, C, W-135, Y | Routine for all adolescents at 11–12 and 16 years; military recruits; college freshmen; asplenic patients |
| MenB (Bexsero/Trumenba) | Serogroup B | Adolescents/young adults; specifically recommended for asplenic patients, complement-deficient patients |
5. Moraxella catarrhalis
5.1 Key Features
- Formerly called Neisseria catarrhalis then Branhamella catarrhalis; renamed based on genetic analysis
- Unencapsulated gram-negative diplococcus (Harrison's) / some sources describe encapsulated with pili
- Oxidase positive, catalase positive, nonsaccharolytic (does not ferment glucose, maltose, or lactose)
- DNase positive — key differential from Neisseria
- Butyrate esterase positive
- >90% produce β-lactamase (assume penicillin resistance)
- "Hockey puck" colonies: smooth, white, opaque — can be pushed around a plate without disrupting colony integrity
- Grows on blood agar (unlike Neisseria, which requires chocolate agar)
- Poor or no growth on MacConkey agar
5.2 Epidemiology
- Ecologic niche: human respiratory tract
- Nasopharyngeal colonization common in infants (33–100%); decreases with age
- Widespread pneumococcal vaccination has increased M. catarrhalis colonization rates (ecological shift)
5.3 Pathogenesis
- Causes infection by contiguous spread from upper airway colonization
- Adhesin molecules attach to respiratory epithelial cells; intracellular survival in lymphoid tissue
- Sheds outer membrane vesicles that mediate inflammation and deliver β-lactamase (protects co-pathogens like H. influenzae and Strep A)
- New strain acquisition critical in COPD exacerbations
5.4 Clinical Diseases
| Disease | Notes |
|---|---|
| Otitis media (children) | 15–20% of acute otitis media cases (by culture); 30–50% by PCR |
| Sinusitis | ~20% of acute bacterial sinusitis in children |
| COPD exacerbations | Most common cause in adults with COPD |
| Bronchitis, laryngitis, tracheitis | Particularly in patients with underlying lung disease |
| Pneumonia | Usually in immunocompromised or COPD patients |
| Bacteremia, endocarditis, meningitis | Infrequent |
| Ophthalmia neonatorum | Rare |
5.5 Treatment
- Assume penicillin resistance (>90% β-lactamase producers)
- Susceptible to: cephalosporins (oral 2nd/3rd gen), TMP-SMX, β-lactamase inhibitor combinations (amoxicillin-clavulanate), fluoroquinolones, macrolides
6. Commensal Neisseria Species
Several Neisseria species colonize the upper respiratory tract as normal flora. They may cause opportunistic infections in immunocompromised hosts.
| Species | Notes |
|---|---|
| N. lactamica | Common in children; ferments lactose; rarely pathogenic |
| N. sicca, N. mucosa, N. subflava | Oropharyngeal commensals |
| N. flavescens | Yellow-pigmented |
These can occasionally cause endocarditis, meningitis, or septicemia in immunocompromised patients.
7. Related Genera (Neisseriaceae Family)
| Genus | Key Species | Disease | Notes |
|---|---|---|---|
| Eikenella | E. corrodens | Human bite infections, endocarditis (HACEK) | Gram-negative rod/coccobacillus; normal oral flora |
| Kingella | K. kingae | Endocarditis (HACEK), septic arthritis in children | Common in children <5 |
8. Anaerobic Gram-Negative Cocci
Veillonella spp.:
- Gram-negative anaerobic cocci
- Normal flora of the mouth, intestine, and vagina
- Rare cause of infection: endocarditis, bacteremia, dental abscesses
- Distinguished by: obligate anaerobe, inability to ferment most carbohydrates, characteristic nitrate reduction
9. Diagnostic Comparison Summary
| Feature | N. gonorrhoeae | N. meningitidis | M. catarrhalis |
|---|---|---|---|
| Gram stain | GN diplococci | GN diplococci | GN diplococci |
| Oxidase | + | + | + |
| Catalase | + | + | + |
| Glucose | + | + | − |
| Maltose | − | + | − |
| Lactose | − | − | − |
| DNase | − | − | + |
| Capsule | No | Yes | No (generally) |
| β-lactamase | Variable | Rare | >90% |
| Growth on blood agar | Poor | Fair | Good |
| Growth on Thayer-Martin | Yes | Yes | No |
| Special media needed | Yes (chocolate/TM) | Yes | No |
| Butyrate esterase | − | − | + |
| IgA protease | Yes | Yes | No |
10. Key Clinical Pearls
- Gonorrhea cannot infect the squamous epithelium of the vagina in postpubescent women — infects only columnar epithelial cells (cervix, fallopian tubes)
- Disseminated N. gonorrhoeae → classically presents as dermatitis-arthritis syndrome (migratory polyarthritis + pustular rash) — culture often negative; treat empirically
- Waterhouse-Friderichsen syndrome = bilateral adrenal hemorrhage from N. meningitidis — presents as overwhelming sepsis + purpura + adrenal crisis
- N. meningitidis vs N. gonorrhoeae: meningitidis uses both maltose AND glucose; gonorrhoeae uses glucose only — mnemonic: "Men use more sugars"
- Complement deficiency (C5–C9, terminal complement) → increased risk of disseminated Neisseria infections (both species)
- M. catarrhalis "hockey puck" sign on agar is a quick bedside lab clue
- Ophthalmia neonatorum prophylaxis with erythromycin eye drops prevents both gonorrheal AND chlamydial neonatal conjunctivitis
- NAAT has replaced culture for routine gonorrhea diagnosis but culture is still needed for antibiotic susceptibility testing
Sources: Medical Microbiology 9e; Henry's Clinical Diagnosis and Management by Laboratory Methods; Quick Compendium of Clinical Pathology 5th ed.; Harrison's Principles of Internal Medicine 22E (2025); Murray & Nadel's Textbook of Respiratory Medicine.
sterptococci detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
Streptococcus gram positive cocci chains microscopy hemolysis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.