Oesophageql varices
Reading File
Finding Sources
Finding Sources
Searching PubMed
"esophageal varices"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have a comprehensive set of textbook content. Let me compile the full, detailed answer.
Oesophageal Varices
Definition and Pathogenesis
Oesophageal varices are dilated, tortuous submucosal and subepithelial veins in the distal oesophagus (and proximal stomach) that form as portosystemic collaterals in the setting of portal hypertension. The fundamental mechanism: portal blood, which normally flows from the left gastric (coronary) veins to the liver, is diverted under high pressure into the systemic venous system via the azygos, hemiazygos and intercostal tributaries - enlarging the submucosal venous plexuses of the oesophagus along the way. These are termed "uphill varices" because blood flows superiorly from portal to systemic tributaries. Much less commonly, "downhill varices" develop in the upper/mid oesophagus due to superior vena cava obstruction.
- Robbins Basic Pathology, p. 546 - "The increased blood flow enlarges and dilates subepithelial and submucosal venous plexi within the distal esophagus."
- Grainger & Allison's Diagnostic Radiology - uphill varices appear as serpentine filling defects at fluoroscopy or CT.
Barium swallow showing oesophageal varices (serpentine filling defects in the distal oesophagus):

Aetiology
| Cause | Notes |
|---|---|
| Hepatic cirrhosis | Most common cause worldwide; alcohol-related disease predominates in Western countries |
| Hepatic schistosomiasis | Second most common cause globally |
| Portal vein thrombosis | Non-cirrhotic cause; splenic vein thrombosis → isolated gastric varices |
| Budd-Chiari syndrome | Hepatic vein outflow obstruction |
| SVC obstruction | Causes "downhill" varices in upper/mid oesophagus |
Epidemiology and Natural History
- Varices are present in ~40% of all cirrhotic patients and up to 60% of cirrhotics with ascites.
- In cirrhotics without varices at initial endoscopy, new varices develop at ~5% per year.
- Small varices progress to large at ~10% per year, related to degree of liver dysfunction.
- Up to 25% of patients with newly diagnosed varices will bleed within 2 years.
- Risk of bleeding by 2 years: 7% for varices <5 mm; 30% for varices >5 mm.
- The hepatic venous pressure gradient (HVPG) is the most important predictor: bleeding is virtually absent when HVPG <12 mmHg.
After a first bleed:
- ~80-90% of episodes are controlled with initial treatment.
- ~1/3 of patients who stop bleeding will rebleed within 6 weeks.
- Mortality: 5-8% at 1 week, ~20% at 6 weeks.
- Among survivors, up to 60% will have additional haemorrhage episodes, each potentially fatal.
Sleisenger & Fordtran's GI and Liver Disease
Classification
Grading of Oesophageal Varices (endoscopic):
- Grade I - Small, straight, collapse with insufflation
- Grade II - Enlarged, tortuous, do not collapse fully
- Grade III - Large, coil-shaped, occupy >1/3 of lumen
Endoscopic high-risk stigmata:
- Red wale marks
- Cherry-red spots
- Hematocystic spots
- White fibrin plugs or blood clots over a varix
Gastric varices - Sarin classification:
- GOV1 - Extending 2-5 cm below gastro-oesophageal junction, continuous with oesophageal varices (most common, 70%)
- GOV2 - In cardia/fundus, continuous with oesophageal varices
- IGV1 - Isolated fundal varices (absent oesophageal varices; often splenic vein thrombosis)
- IGV2 - Isolated varices in body, antrum, or pylorus
Clinical Features
- Often asymptomatic until rupture
- Rupture presents as sudden, large-volume haematemesis - a life-threatening emergency
- Associated features of chronic liver disease: jaundice, spider naevi, palmar erythema, caput medusae, splenomegaly, ascites, hepatic encephalopathy
- Variceal bleeding accounts for 59% of upper GI bleeds in cirrhotic patients; in-hospital mortality for GI bleeding in cirrhotic patients is essentially double that of non-cirrhotics
Diagnosis
1. Endoscopy (EGD) - gold standard for diagnosis and treatment
- Diagnosis of active variceal bleed requires: active bleeding from varices OR signs of recent haemorrhage (white fibrin plug, red clot) OR risk stigmata (cherry-red spot, red wale) in the absence of another lesion
2. HVPG measurement - Hepatic venous pressure gradient
- HVPG >12 mmHg required for varices to form
- HVPG >20 mmHg: high risk of treatment failure and rebleeding
- Target of pharmacotherapy: reduce HVPG to <12 mmHg or by ≥20%
3. Imaging
- Doppler ultrasound - assess portal vein patency, direction of flow, splenomegaly
- CT with IV contrast - demonstrates varices, shunts, portal vein thrombosis, cirrhotic liver morphology
- Barium swallow - shows serpentine filling defects (largely superseded by endoscopy)
Management
Treatment is classified into three phases:
1. Primary Prophylaxis (Prevention before first bleed)
Algorithm:
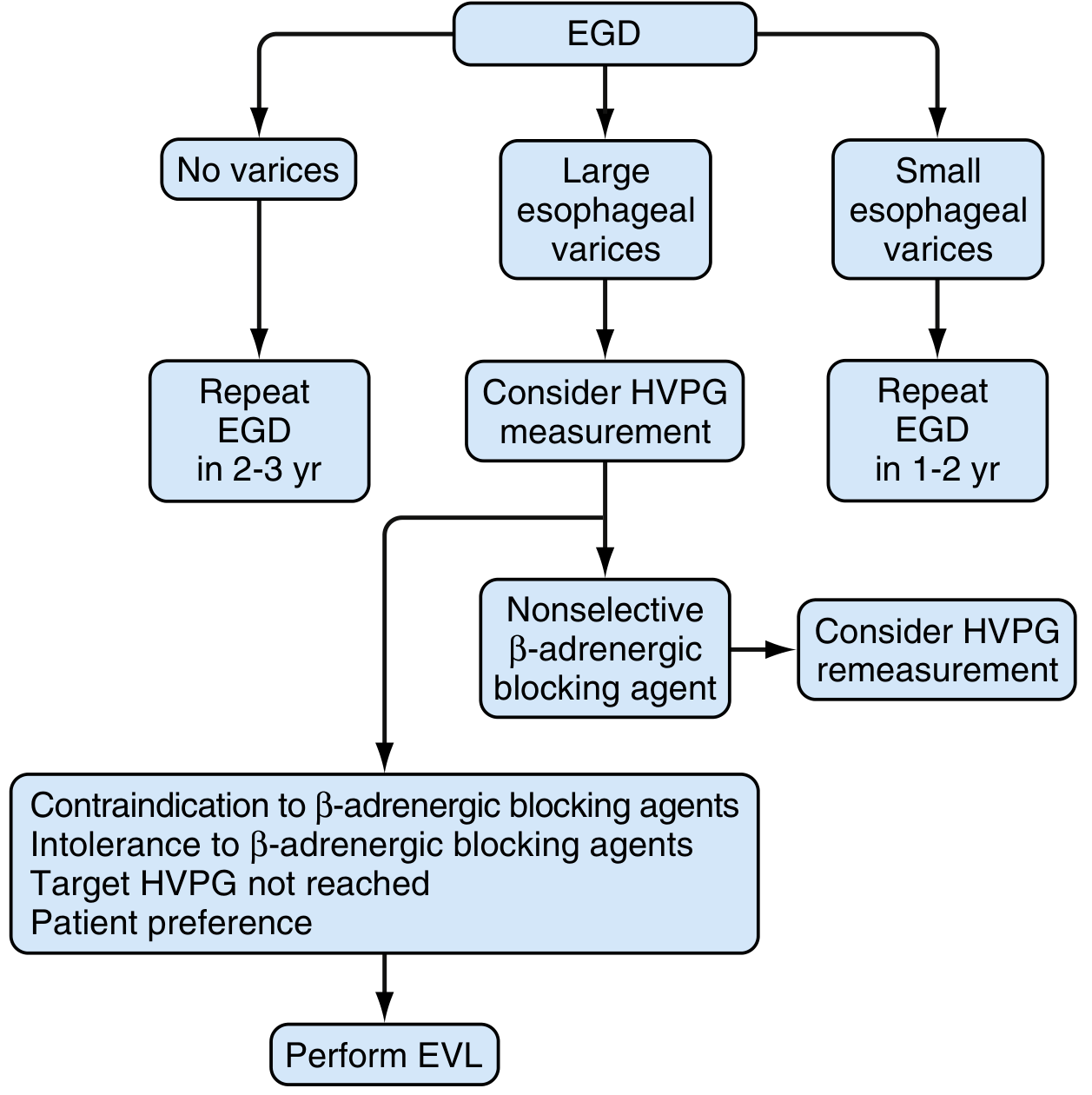
(Fig. 92.13 - Sleisenger & Fordtran's GI and Liver Disease)
Indications: All patients with large varices (>5 mm) should receive prophylactic therapy.
Pharmacological - Non-selective beta-blockers (NSBBs):
- Propranolol (long-acting): start 60 mg once daily at night; titrate to target HR 25% below baseline or 55-60 bpm; max 160 mg/day
- Nadolol: start 20 mg once daily; similar titration
- Carvedilol: start 6.25 mg daily; max 25 mg daily (used in hypertension or CAD)
- Target: systolic BP >90 mmHg at all times
- Absolute risk reduction ~10%; NNT to prevent 1 bleed = ~10
- Mortality reduction: 28.4% → 23.9%
- ~15% need to discontinue due to side effects
- Treatment should be continued indefinitely
Endoscopic - Endoscopic Variceal Ligation (EVL):
- Used when contraindication/intolerance to beta-blockers, target HVPG not reached, or patient preference
- Banding sessions every 2-4 weeks until variceal obliteration
2. Control of Acute Variceal Bleeding
Algorithm for Management:
This is a medical emergency requiring an MDT approach (hepatologist, endoscopist, intensivist, radiologist, surgeon).
Initial Resuscitation:
- Two large-bore IV lines
- Restrictive transfusion strategy: transfuse RBCs only when Hgb drops below 7 g/dL (improved survival vs. <9 g/dL threshold in Child-Pugh A/B)
- Protect airway - endotracheal intubation for active bleeding
- Correct coagulopathy
Antibiotics (mandatory in ALL patients):
- Norfloxacin 400 mg orally twice daily × 7 days (preferred)
- If unavailable: ciprofloxacin 500 mg orally bd × 7 days
- IV ciprofloxacin 400 mg q12h or ceftriaxone 1 g q24h × 7 days if oral intake impossible
- Failure to control infection → significantly increased mortality and rebleeding risk
Vasoactive Drugs (start as early as possible):
| Drug | Dose | Notes |
|---|---|---|
| Terlipressin | 2 mg IV q4h | First choice in many countries; only agent shown to improve survival |
| Octreotide | 50 mcg bolus then 50 mcg/hr infusion | Most used in USA |
| Somatostatin | 250 mcg bolus then 250 mcg/hr | Similar efficacy |
| Vapreotide | 50 mcg bolus then 50 mcg/hr | Similar efficacy |
- Continue for up to 5 days to prevent early rebleeding
- Pharmacological + endoscopic combination is superior to pharmacological alone
Endoscopic Therapy:
- Performed as soon as patient is haemodynamically stabilised
- EVL is the preferred method - bleeding controlled in 85-90% with combined pharmacological + endoscopic treatment
- Ligation begins at/below bleeding site, then other large varices banded
- If active bleeding obscures view: circumferential bands at gastro-oesophageal junction
Failure to control bleeding (criteria: transfusion of ≥4 units RBCs to maintain Hct >25%, inability to increase systolic BP by 20 mmHg or to >70 mmHg, HR persistently >100 bpm):
- TIPS (Transjugular Intrahepatic Portosystemic Shunt) - salvage therapy if 2 endoscopic sessions within 24 hours fail
- Early TIPS (within 72 hours): indicated in high-risk patients: Child-Pugh class C, Child-Pugh class B with active bleeding, or MELD >18 requiring >4 units RBCs - associated with reduced mortality and treatment failure
- Oesophageal stents - to stabilise until definitive treatment (preferred over balloon tamponade when available)
- Balloon tamponade (Sengstaken-Blakemore or Minnesota tube) - only when oesophageal stents unavailable; temporising measure
- Surgical portosystemic shunts - largely abandoned due to high mortality
Bailey & Love's Short Practice of Surgery 28th Ed., Sleisenger & Fordtran's GI and Liver Disease
3. Prevention of Rebleeding (Secondary Prophylaxis)
All patients who survive a variceal bleed must receive secondary prophylaxis.
Secondary Prophylaxis Algorithm:
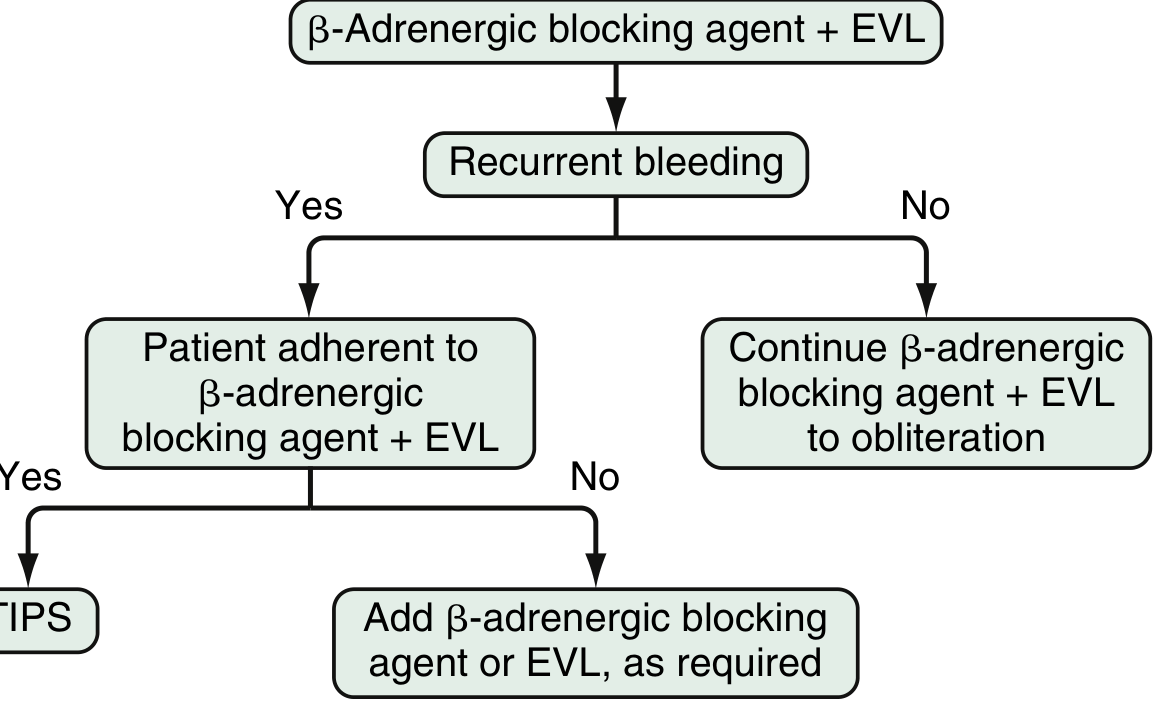
(Fig. 92.16 - Sleisenger & Fordtran's GI and Liver Disease)
First-line: Combination of NSBB + EVL
- Combined therapy reduces rebleeding risk in Child-Pugh A patients compared to NSBB alone
- Combination + beta-blocker reduces mortality in Child-Pugh B and C patients compared to EVL alone
- EVL performed every 2-4 weeks until variceal obliteration, then surveillance EGD at 3 months, then every 6-12 months
Rebleeding despite optimal therapy:
- Patient adherent to therapy → TIPS (or distal splenorenal shunt in Child-Pugh A; equally effective)
- Patient non-adherent → add missing component (EVL or beta-blocker)
- Liver transplantation - definitive treatment for end-stage liver disease
Summary of Key Management Principles
| Phase | Intervention |
|---|---|
| Primary prophylaxis | NSBB (propranolol/nadolol/carvedilol) ± EVL |
| Acute bleed - resuscitation | Restrictive RBC transfusion (Hgb <7), airway protection, coagulopathy correction |
| Acute bleed - pharmacological | Terlipressin or octreotide (up to 5 days) + antibiotics |
| Acute bleed - endoscopic | EVL (preferred) or sclerotherapy |
| Salvage | TIPS, oesophageal stents, balloon tamponade |
| Secondary prophylaxis | NSBB + EVL → TIPS if recurrent |
| Definitive | Liver transplantation |
Pathology (Morphology)
Varices appear on endoscopy as tortuous dilated veins within the submucosa of the distal oesophagus and proximal stomach. The overlying mucosa may be intact, thinned, or ulcerated/necrotic after rupture. Histologically, they represent dilated venous channels in the lamina propria and submucosa; the thin wall and lack of supporting tissue in the lower oesophagus (unlike the stomach) makes them particularly prone to rupture.
Robbins & Kumar Basic Pathology, p. 546; Robbins, Cotran & Kumar Pathologic Basis of Disease
Sources:
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 92 - detailed natural history, pharmacology, and management algorithms
- Bailey & Love's Short Practice of Surgery, 28th Ed., Chapters 66 & 69 - surgical management
- Robbins & Kumar Basic Pathology - pathogenesis and morphology
- Grainger & Allison's Diagnostic Radiology - imaging features
- Tintinalli's Emergency Medicine - acute bleeding in the ED context
This is a shared conversation. Sign in to Orris to start your own chat.